
Abstract
Purpose
School teachers show higher levels of internalized distress compared to those in many other professions. In two exploratory studies, we examine the relative and interactive impacts of mindfulness training (MT) and medication use on reductions in depressive and anxious symptoms in teachers over time.
Design/Approach/Methods
These questions are explored using data from two randomized, waitlist-controlled trials of an 8-week teacher MT program. Data on medication use for anxiety or depression were assessed at baseline and revealed that 20% of the study samples reported such use. In addition, symptoms of anxiety and depression were assessed at baseline, post-program, and 3-month follow-up.
Findings
Results showed that MT significantly reduced depressive symptoms at post-program and at 3-month follow-up even after accounting for medication use. A similar pattern was found for anxious symptoms in Study 2 (but not Study 1). Comparative effects analysis indicated that MT resulted in stronger declines in depressive and anxious symptoms over time, while the effects of medication remained relatively stable.
Originality/Value
Results suggest that MT is an effective tool for reducing internalized distress in public school teachers, adds benefits above and beyond the use of medication for such symptoms in this population, and may result in greater long-term symptom reduction.
Teaching is a highly stressful profession (Jepson & Forrest, 2006), and teacher stress and burnout is an internationally recognized problem (Bermejo-Toro et al., 2015). In addition to higher levels of stress, burnout, and job turnover, teachers suffer from higher rates of internalizing (depressive and anxious) symptoms compared to those in other occupations (Stansfeld et al., 2011; Wulsin et al., 2014) and in the general population (Jones-Rincon & Howard, 2019). These problems have worsened among teachers during the course of the COVID-19 pandemic, with one study from early 2021 finding that 27% of teachers have experienced symptoms consistent with depression, while 37% have experienced symptoms consistent with generalized anxiety disorder (Steiner & Woo, 2021).
To manage symptoms of internalized distress, teachers may turn to therapy or psychopharmacological treatments (Wulsin et al., 2014), drugs and alcohol (Richards, 2012; Watts & Short, 1990), or other coping strategies (Austin et al., 2005). One alternative approach to addressing symptoms of internalized distress is mindfulness training (MT; Grossman et al., 2010; Kim et al., 2009). A growing body of work suggests that MT can be effectively adapted for the school setting to help teachers reduce levels of internalized distress (Benn et al., 2012; Roeser et al., 2013, 2022).
A gap in this literature, however, concerns controlling for other treatments teachers may already be pursuing to manage these symptoms. Given the elevated rates of internalizing symptomatology in this population, as well the widespread usage of antidepressant and anxiolytic medication more generally (Greenblatt et al., 2018), it is likely that teachers may already be pursuing medication therapies to manage depression and anxiety. Thus, it is imperative to understand what additional benefits MT may provide over and above medications that teachers may be taking to manage depressive and anxious symptoms. The aim of the present research was to investigate the impacts of MT on reductions in depressive and anxious symptoms while accounting for the fact that some teachers may already be using medications for such symptoms, and to investigate the relative contributions of MT and medication use to change in symptoms of anxiety and depression in teachers over time.
Internalized distress among school teachers
Depression and anxiety have been conceptualized as internalizing problems, meaning that both depression and anxiety can be characterized by a tendency to cope with one’s distress through directing negative emotions inwards (Caspi et al., 2014). The teaching profession has been shown to have high prevalence rates of depression and anxiety compared to other occupations in the United Kingdom (Stansfeld et al., 2011). These results have been replicated in U.S. samples, with an estimated 10.3% prevalence of depression for teachers in the United States, even after adjusting for age and gender (Wulsin et al., 2014).
Prevalence for anxiety is similarly high. In a study of 3,321 teachers in the United States, fully 14% met criteria for generalized anxiety disorder (Jones-Rincon & Howard, 2019). Furthermore, evidence suggests that teachers who experienced burnout were more likely to exhibit symptoms of anxiety and depression (Burke et al., 1996; Mahan et al., 2010), and that teachers with anxious symptoms were more likely to report intent-to-quit (Jones-Rincon & Howard, 2019). Given the costs associated with the alarmingly high turnover rates in the teaching profession (Ingersoll, 2002), finding effective methods of managing and preventing internalizing symptomatology is essential.
Medication use for internalized distress in school teachers
Studies in the United Kingdom indicate that over 1 in 10 teachers are taking antidepressants to cope with work stresses (NASUWT, 2023). While comprehensive data on U.S. school teachers, medical health records indicating antidepressant use is not available, given that around 77% of all U.S. middle and high school teachers are women (Goldring et al., 2017), estimates of such use are possible. For instance, given that women experience nearly twice the rates of both depression and anxiety compared to men (Kessler et al., 2022), and data suggest that over 17% of all U.S. women are taking some form of antidepressant (Brody & Gu, 2020), it is likely that antidepressant use among U.S. school teachers is similar or greater than rates found in the United Kingdom (e.g., 10%). Thus, finding effective ways to prevent and manage mental health symptoms in teachers is critical in order to increase teachers’ health and well-being, foster their retention, improve teaching practices and student outcomes, and reduce health care costs.
Efficacy of MT for school teachers
In addition to randomized controlled trials (RCTs) that demonstrate the effectiveness of MT for depression and anxiety in clinical samples (Kim et al., 2009; Mackenzie & Kocovski, 2016), a growing body of work suggests that MT can be effective in reducing depressive and anxious symptoms in school teachers (Benn et al., 2012; Flook et al., 2013; Roeser et al., 2013, 2022). For instance, research on the Cultivating Awareness and Resilience in Education (CARE for Teachers) teachers program (Jennings et al., 2017) and an adapted version of Mindfulness-Based Stress Reduction (MBSR; Kabat-Zinn, 1982) for school teachers (Flook et al., 2013) found significant reductions in teachers’ depressive and anxious symptomatology over time due to MT.
Consistent with research on MT in community samples of adults (Chiesa & Serretti, 2009), a recent meta-analysis of the extant database on MT for teachers reveals small to medium teacher-level impacts of MT on changes in mindfulness skills (Hedge's g = 0.69), occupational stress and burnout (Hedge's g = 0.55), and psychological well-being (Hedge's g = 0.43) from before to after training, compared with controls (Klingbeil & Renshaw, 2018). In addition, Klingbeil and Renshaw (2018) reported a small effect of MT on classroom climate and quality of teachers’ interactions with students in the classroom from pre- to post-program compared with controls across their reviewed studies (Hedge's g = 0.31).
In a decades-long research program on the Mindfulness-Based Emotional Balance (MBEB) program for teachers (see Cullen et al., 2019), our research group has also documented medium to large effects of MBEB on reductions in teachers’ symptoms of anxiety and depression at post-program and 2- to 3-month follow-up (see Benn et al., 2012; Roeser et al., 2013, 2022). In a combined study of Canadian and American school teachers, Roeser et al. (2013) reported large effect sizes for reductions in symptoms of anxiety at post-program (d = 0.71) and 3-month follow-up (d = 1.10), and for reductions in depressive symptoms at post-program (d = 1.06) and 3-month follow-up (d = 1.56). In addition, in a study of the MBEB program with American middle school teachers, Roeser et al. (2022) found large effect sizes for reductions in symptoms of anxiety at post-program (g = 0.82) and 3-month follow-up (g = 0.88), and medium effect sizes for reductions in depressive symptoms at post-program (g = 0.34) and 3-month follow-up (g = 0.32). Finally, in a combined sample of educators and parents of special needs students, Benn et al. (2012) reported medium to large program effects for reductions in symptoms of anxiety at post-program (d = 0.52) and 2-month follow-up (d = 0.75), and medium effect sizes for reductions in depressive symptoms at post-program (d = 0.51) and 2-month follow-up (d = 0.27).
Given the literature on MTs for school teachers is still relatively limited (about 10–12 studies; Klingbeil & Renshaw, 2018), and only some of these studies assess depressive and anxious symptoms specifically, as compared to more general stress measures, more research on depressive and anxious symptom reduction in school teachers is needed. Furthermore, one study (Gold et al., 2010) found that teachers’ participation in an 8-week MBSR program resulted in statistically significant reductions in depressive, but not anxious, symptoms, leaving open the question of whether MT may be more effective for particular types of internalizing symptomatology. Furthermore, less work has examined how MTs perform in relation to other treatment options that teachers may be using to manage internalized distress. Understanding the benefits of MT for teachers with internalized distress remain after accounting for medication use for depression and anxiety is important in order to assess the efficacy of MTs, and to examine the incremental and long-term benefits of MT. Given that MT has been shown to reduce repetitive negative thinking processes that worsen depression and anxiety (e.g., rumination and worry; Delgado et al., 2010; Hawley et al., 2014), it is likely that MT is effective in symptom reduction above and beyond medications.
The present study
Using data from two RCTs that showed reductions in depressive and anxious symptoms in teachers (Roeser et al., 2013; described above), exploratory analyses examined if the benefits of MT with regard to reducing symptoms of internalized distress remain after accounting for medication use for depression and anxiety, and also, the relative benefits of MT versus medication use on change in symptoms over time. In addition, in Study 2, we examined the interaction of MT and medication use on symptom change over time. Specifically, we examined the following research questions: (1) Does MT reduce internalizing symptoms when accounting for those already taking medications for these conditions? (2) What are the relative impacts of MT after accounting for medication use (effect size)? (3) Are there long-term benefits of MT for those taking medications? (4) Does taking medications moderate the impacts of MT on internalizing symptoms?
These exploratory analyses in a sample of teachers are, to the best of our knowledge, the first to examine the impacts of MT on internalizing symptoms in teachers accounting for medication use. Because neither of the two studies reported here block-randomized teacher participants to experimental condition based on medication use, these analyses fall outside the causal inferences made possible by the RCT designs of these studies and are meant to extend previously reported results. Accordingly, we did not generate specific hypotheses but hope that the present study could help in framing such hypotheses in future work.
Study 1
Method
Sample
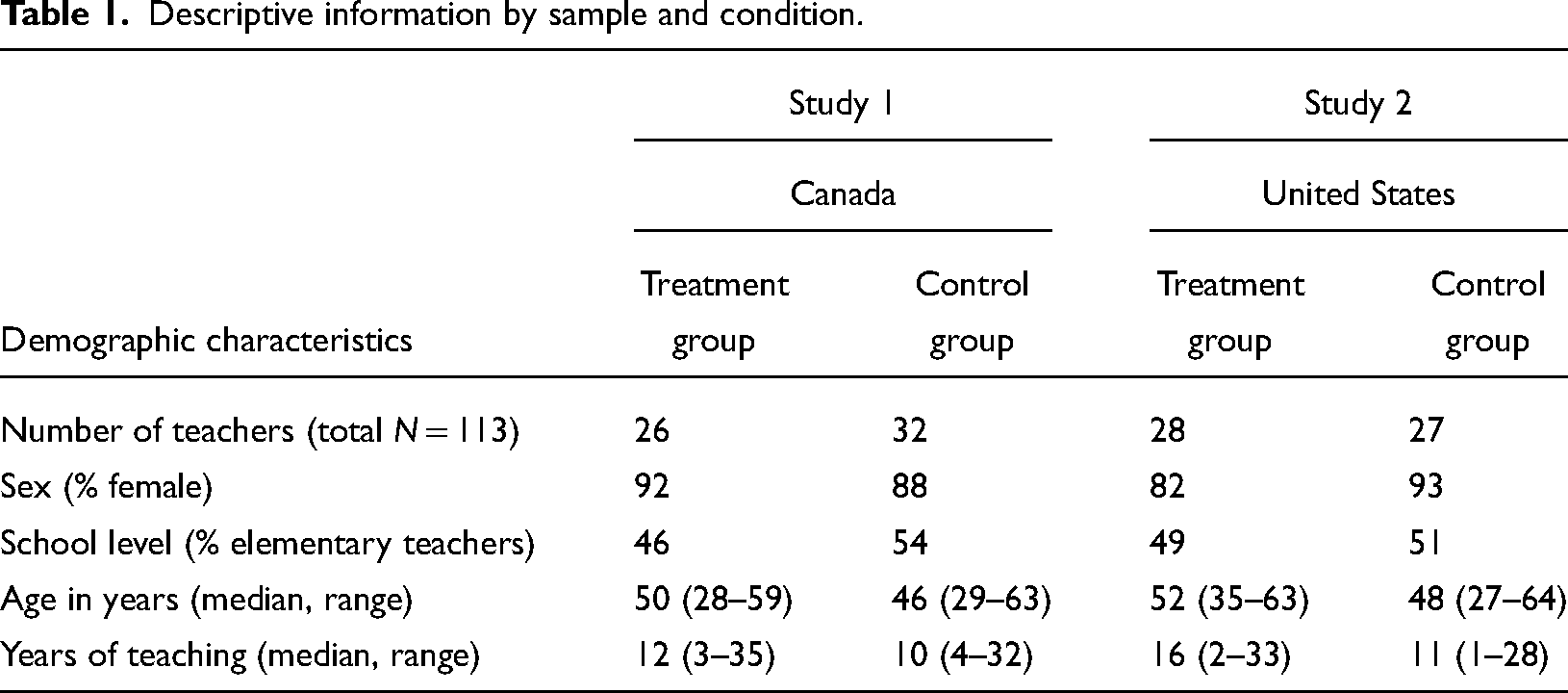
Descriptive information by sample and condition.
Means, standard deviations, and effect sizes for depressive and anxious symptoms at each timepoint in Study 1.
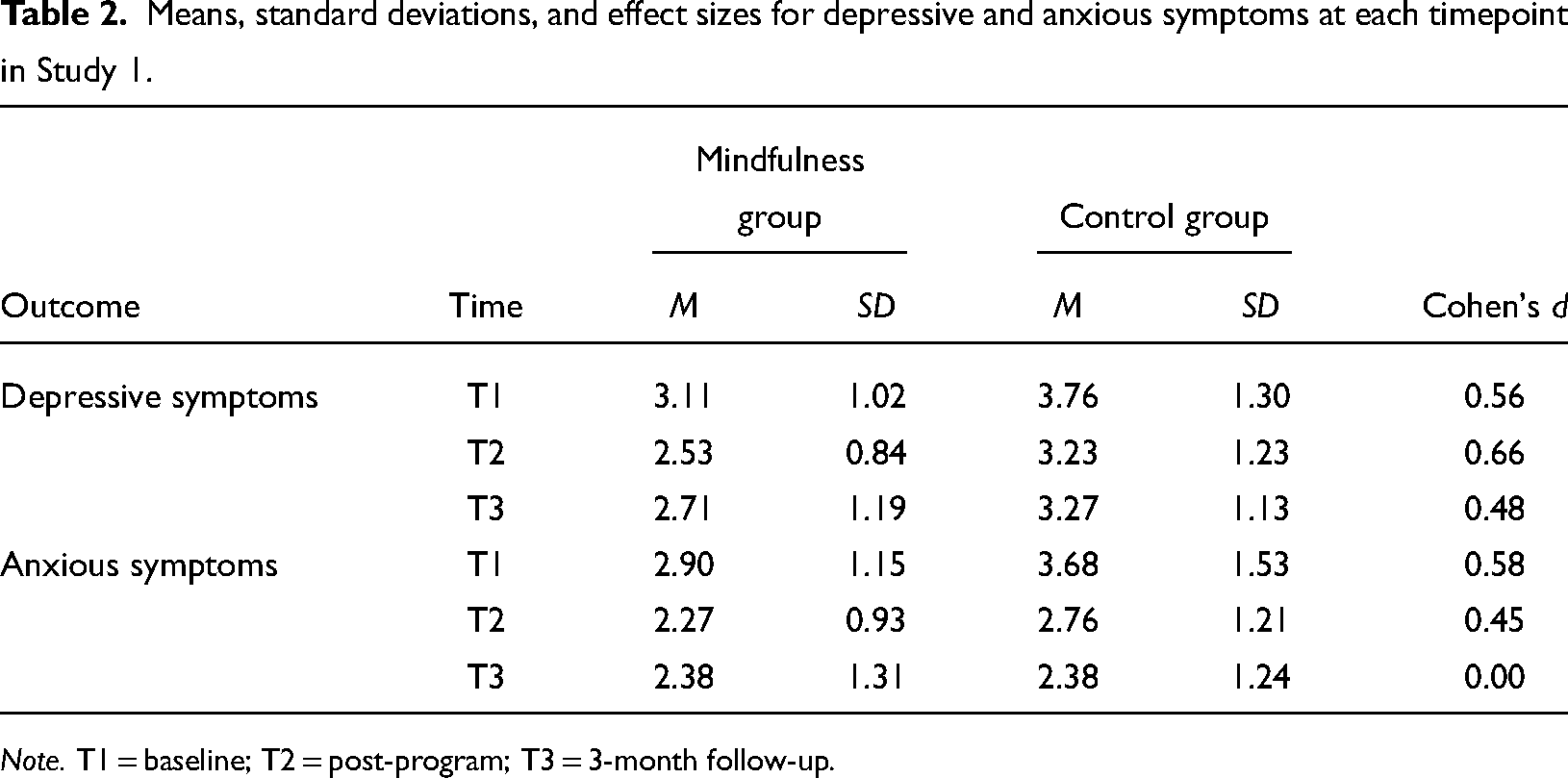
Note. T1 = baseline; T2 = post-program; T3 = 3-month follow-up.
Procedures
Recruited teachers were screened for prior exposure to training for the Goldie Hawn Foundation's MindUp program (https://mindup.org), a mindfulness-based program for students that was popular in this Canadian school district. Teachers who had received MindUp training were excluded from the study. Participants were allocated to groups based on a simple randomization procedure—flipping a coin (Suresh, 2011). Sample sizes were equivalent across groups (Supplementary Materials, Table S1).
After randomization to study conditions, participants in the mindfulness condition received the 8-week MT program from April to May of the school year. Participants in the waitlist control condition had the opportunity to complete the MT from October to December during the next school year and after the follow-up data had been collected. Teachers in both conditions completed study assessments at three time points: pre-randomization/baseline (T1, February–March), post-program (T2, May–June); and at 3-month follow-up (T3, October). All participants received the MT for free and were compensated for completing assessments. Those in the control groups were offered the program after the 3-month follow-up was completed.
MT program
The MT program that was taught and evaluated in both studies was called the Stress Management and Relaxation Training (SMART) Program at the time (see Cullen et al., 2019 for history), a fully manualized mindfulness program designed specifically for teachers. This program is based upon Jon Kabat-Zinn's widespread MBSR (Grossman et al., 2004) program, and uses approximately 50% of the same mindfulness meditation and movement practices (e.g., body scan, focused-attention, and open-monitoring practices). About 30% of the program is devoted to emotion theory (e.g., definitions, triggers, imported scripts) and mindful emotion regulation. The remaining 20% of the program focuses on the theory and practice of compassion and forgiveness (see Cullen et al., 2019 for program overview). Implementation fidelity was high across both studies. The original impacts study showed that teachers at both sites practiced mindfulness for an average of about 15 min per day, stated that the program delivered on its stated learning objectives, and that 98% of the teachers who went through the program would recommend it to other teachers (see Roeser et al., 2013 for further details).
Measures
Demographic characteristics
Teachers’ gender and years of teaching experience were included as statistical controls in assessing the impacts of MT on symptom change given that prior literature suggests that both factors (e.g., woman gender, less experience) are related to internalizing symptomatology (Ferguson et al., 2012; Kessler et al., 1994). Sample descriptions in terms of demographics are presented in Table 1.
Depressive symptoms
Depressive symptoms were assessed with 13 items from the Bischof Adult Symptom Inventory (BSI; Bischof, personal communication, September 19, 2019). The BSI is a 41-item initial screening instrument developed for clinical practice that screens for a number of psychological disorders. It was developed and validated by a team of seven clinical psychologists and is based closely on Diagnostic and Statistical Manual of Mental Disorders, Third Edition (DSM-III) criteria (Supplementary Materials, Appendix A). Participants were asked to rate the difficulty they have been experiencing in each area recently using a 5-point Likert scale from 0 = no difficulty to 4 = extreme difficulty. We took the mean of 13 items that were face-valid for depression and that formed a reliable index at Time 1 (α = .91), Time 2 (α = .90), and Time 3 (α = .92). Furthermore, test–retest reliability was adequate as indicated by autocorrelations of r = .81 from T1 to T2, and r = .71 from T1 to T3. 1
Anxious symptoms. Anxious symptoms were assessed with four items from the BSI that were face-valid for anxiety. The items were: “Fearful or anxious about upcoming situations or events,” “Restlessness or feeling keyed-up, on edge,” “Episodes of terror or panic,” and “Unwanted persistent and intrusive thoughts.” The mean score of these items was taken to create an index of anxious symptoms. These items formed a reliable index at Time 1 (α = .83), Time 2 (α = .78), and Time 3 (α = .81). Furthermore, autocorrelations indicated modest test–retest reliability, r = .70 from T1 to T2, and r = .50 from T1 to T3. 2
Medication use
A comprehensive list of medications was also asked of participants. At baseline, 5% of the sample were taking medications for depression, and only 2% were taking medications for anxiety. Furthermore, there were differences between groups in medication use in this study following randomization. Specifically, in the mindfulness group, 0% were taking medications for depression and 4% for anxiety, compared to 11% and 0% for the control group, respectively (see Supplementary Materials, Table S2). Because of these group differences in medication use, we could not test the interaction of MT with medication use in Study 1. Thus, use of these medications was entered into the regression equations as independent predictors in order to estimate the relative impacts of MT and medication use on change in symptoms over time in Study 1 (e.g., rather than as moderators). Medication use was coded dichotomously, where 0 = no medication and 1 = medication (Table 2).
Data analytic approach
We undertook two types of analyses in this study. First, preliminary analyses examined study attrition and baseline equivalence of groups following randomization on demographic and outcome variables. Second, we conducted a series of sequential, hierarchical regression analyses to assess the impacts of MT and medication use on change in symptoms over time—from baseline to post-program and baseline to 3-month follow-up. In Step 1, we entered teachers’ gender, years of teaching experience, and baseline symptoms as covariates; in Step 2, medication use status was entered, and in Step 3, experimental condition (MT vs. waitlist control) was added. We opted for the current analytic approach to retain consistency across prior publications using the same data (Braun et al., 2020; Roeser et al., 2013) and for ease of interpretation. To examine the unique variance explained by MT and medications, we include the change in R2 as a measure of effect size (Cohen et al., 2001). Given the exploratory nature of this work, the small sample size, and the fact that we examined the same research questions in two different studies using the same interaction, we did not adjust for familywise error rates.
Results
Study attrition
Of the total of 29 participants in the mindfulness condition, 11% dropped out of the study from baseline to post-program, and 14% dropped out from post-program to 3-month follow-up. In the control group, attrition rates were 3% from baseline to post-program, and 6% from post-program to 3-month follow-up (see Supplementary Materials, Table S1), in line with average dropout rates for mindfulness interventions (Williams & Crane, 2010). The rate of attrition was relatively equivalent across study conditions. The primary reasons for attrition were due to scheduling conflicts or changes in family responsibilities (e.g., having a new child). There was no indication of iatrogenic effects of the program as a reason for attrition.
Baseline equivalence of groups
Results of t-tests revealed that there were no differences at baseline between groups in levels of depressive or anxious symptoms, or demographic characteristics (e.g., gender, years of teaching experience).
Impacts analyses
To examine the relative impacts of MT and medications on depressive and anxious symptoms, a series of hierarchical linear regression models were conducted. Results of the regression impact analyses are presented in Table 3, with comparative effects of MT and medications, as indicated by unique variance explained (change in R2) represented in Figure 1. In all models, the strongest predictor of depressive and anxious symptoms was baseline level of these symptoms. Thus, impacts for MT and medication use represent impacts on change in symptoms over time in these models.
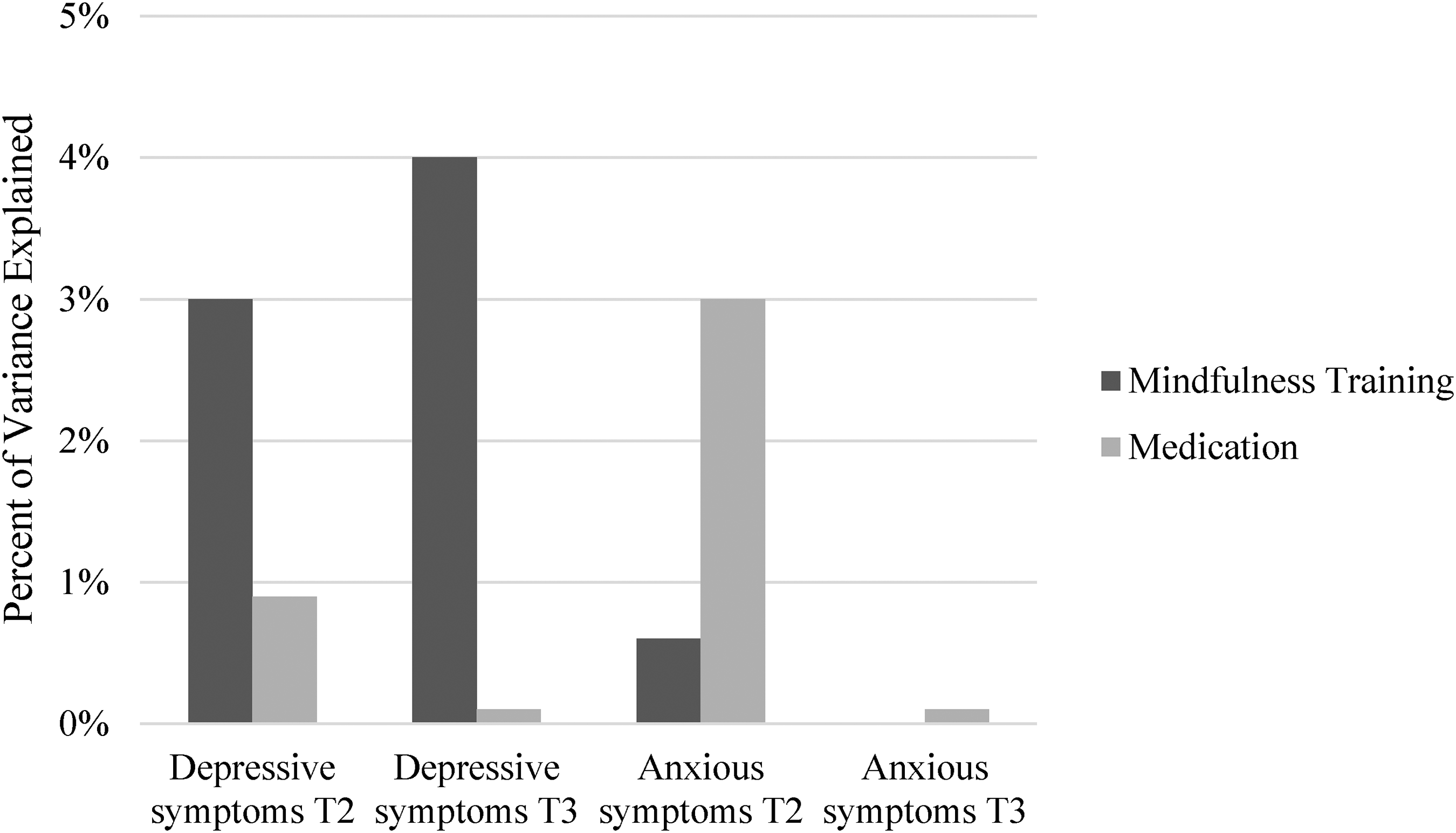
Percentage of variance explained (R2 change) in symptom change based on mindfulness training and medication use (Study 1).
Summary of regression analyses predicting symptoms at post-program and 3-month follow-up in Study 1.
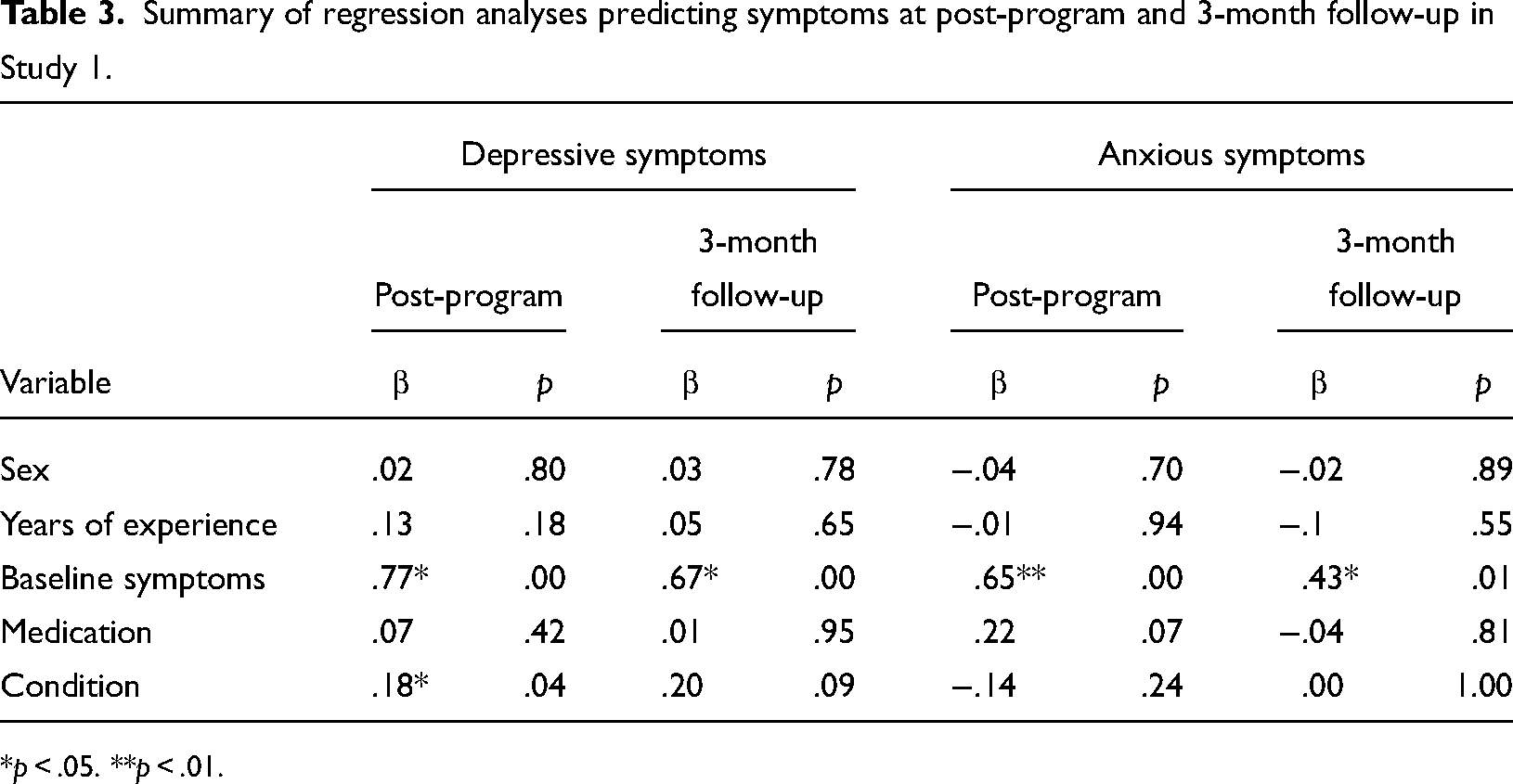
*p < .05. **p < .01.
Means, standard deviations, and effect sizes for depressive and anxious symptoms at each timepoint in Study 2.
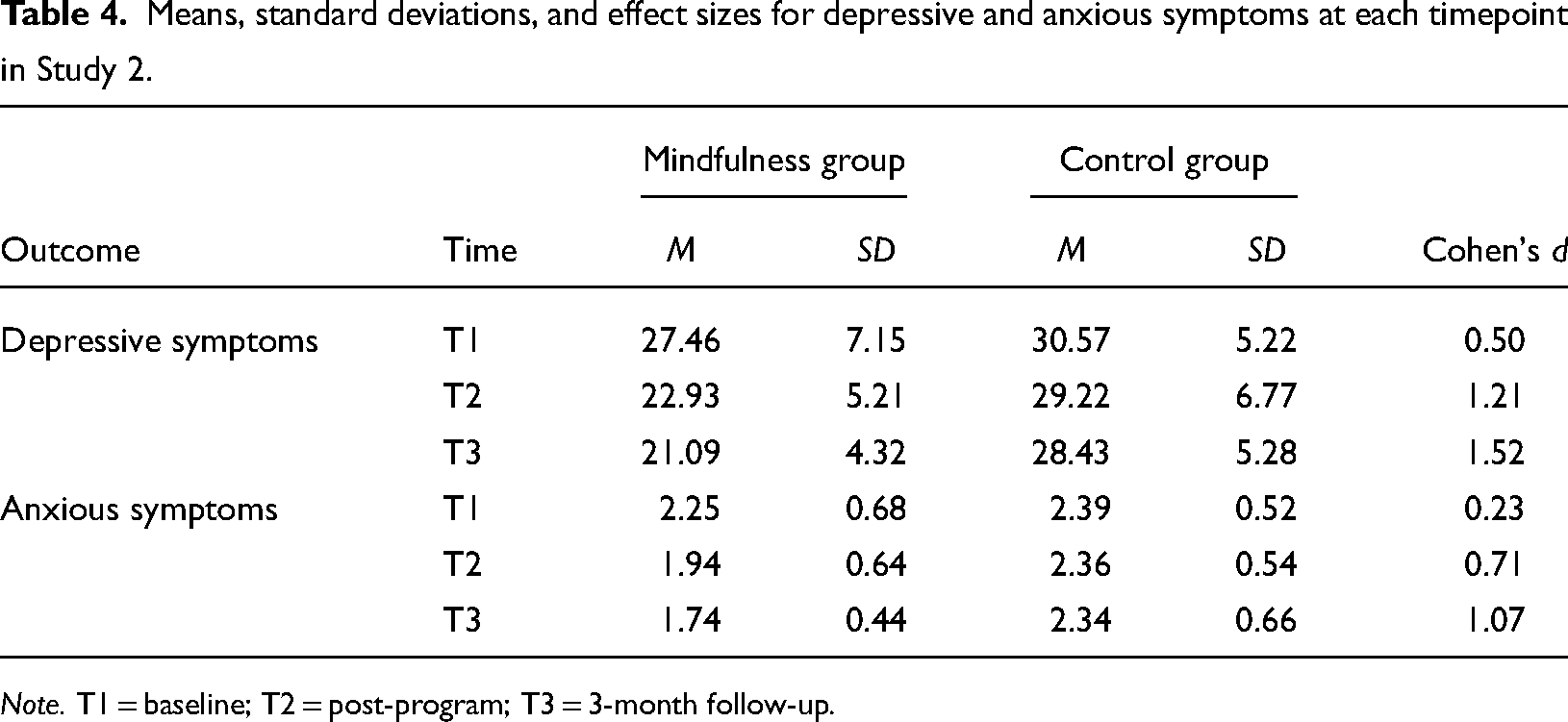
Note. T1 = baseline; T2 = post-program; T3 = 3-month follow-up.
Depressive symptoms
Results of hierarchical linear regression analyses (Table 3; Figure 1) revealed that at post-program, MT had a significant impact on change in depressive symptoms (β = −.18, p < .05; R2 change = .03) after controlling for other variables in the model. Medication use had no impact on depressive symptoms at post-program (β = .07, p = .42; R2 change = .00). At the 3-month follow-up, the same pattern of results was found: MT had an impact on change, but this impact was smaller and reduced to non-significance (β = −.20, p = .09; R2 change = .04). The impact of medication use on symptom change remained non-significant (β = .01 p = .95; R2 change = .00).
Examination of relative impacts of MT and medication as indicated by the amount of variance explained (see Figure 1) indicated that MT explained 3% of the variance in change in depressive symptoms at post-program, whereas medications explained 0% of the variance at post-program. At the 3-month follow-up, MT uniquely accounted for 4% of the variance in symptom change, while 0% was explained by medications.
Anxious symptoms
Results of hierarchical linear regression analyses (Table 3; Figure 1) revealed that at post-program, neither MT (β = −.14, p = .24; R2 change = .00) nor medication use (β = .22, p = .07; R2 change = .03) had a significant impact on change in anxious symptoms. These results did not change at follow-up—namely, there was no effect of MT (β = .00, p = 1.00; R2 change = .00) or medication (β = −.04, p = .81; R2 change = .00) at the 3-month follow-up.
Examination of relative impacts of MT and medication as indicated by the unique amount of variance explained is presented in Figure 1. Results indicated that MT accounted for less than 1% of the variance in change in anxious symptoms at post-program, whereas medications explained 3% of the variance at post-program. At the 3-month follow-up, MT and medications both had a negligible contribution to anxious symptoms (0% of variance explained for both variables).
Study 2
Method
Sample
Participants in Study 2 were recruited from the western region of the U.S. Participants were recruited through distribution of flyers advertising the study as a stress-reduction program, in a similar procedure to that used in Study 1. The results of the main trial are reported in Roeser et al. (2013). The final sample consisted of 59 public school teachers (87% women; 51% elementary level). Participants identified their race/ethnicity as 93% European American, 5% mixed (e.g., Japanese and American), and 2% Asian American. In terms of educational attainment, 20% reported having a bachelor's degree, 73% reported having a master's degree, and 7% reported having a JD or PhD. Participants had an average of 14.88 years of teaching experience (range 1–33; SD = 7.86) and had a median age of 50 (range 27–64, see Table 1).
Procedures
The same procedures for randomization, assessments, and incentives as described above were employed in this study. For all participants, data collection included a take-home survey on mindfulness, subjective well-being, and health collected at baseline, post-program, and 3-month follow-up. The survey measures of depressive and anxious symptoms were different than those used in Study 1 and are reported below. The mindfulness program was identical to Study 1 and was also delivered by the same instructor.
Measures
Beck Depression Inventory-II, Second Edition (BDI-II)
Depressive symptoms were assessed with the BDI-II. The BDI-II (Beck et al., 1988; Beck, Ball, et al., 1996) is a 21-item self-report instrument used to assess the severity of depressive symptoms on a 4-point scale (0–3), with a total score ranging from 0 to 63. Cutoff scores are: 0–13, minimal depression; 14–19, mild depression; 20–28, moderate depression; and 29–63, severe depression (Beck et al., 1988). The BDI-II has a coefficient alpha of .92 with depressed outpatients and .93 with nonclinical samples, and a test–retest reliability coefficient across the period of 1 week of .93 (Beck et al., 1988; Dozois et al., 1998). Scale reliabilities in this sample were high at each timepoint, α = .84–.90.
State-Trait Anxiety Inventory-State Version
Anxious symptoms were assessed with the state anxiety scale of the Spielberger State-Trait Anxiety Inventory (STAI-S; Spielberger et al., 1970). The STAI-S is a 20-item self-report instrument developed to assess levels of situation-related (state) anxiety. Items are rated on a 4-point Likert-type scale to produce a summative score ranging from 20 to 80 with higher scores indicating higher levels of anxiety. The STAI-S has demonstrated reliability and validity, including test–retest reliability (.76–.84; Spielberger et al., 1983), and is frequently used in clinical research (Julian, 2011). In this study, Cronbach's alpha was high at all timepoints, α = .94–.96.
Medication use
As part of a more comprehensive health assessment administered by nurse practitioners (see Roeser et al., 2013 for full details), participants reported on their prescription drug use for depression and anxiety. Specifically, they were provided with a list of common physical and mental health diagnoses, and were asked to indicate whether they were taking prescription drugs for these conditions by checking the relevant box. At baseline, 21.7% of the sample were taking medications for depression, and 16.7% were taking medications for anxiety (see Supplementary Materials, Table S1). There were no significant differences between groups on these medication use variables after randomization (Table 4).
Data analytic approach
We undertook two same analytic approaches as in Study 1—examining study attrition and baseline equivalence of groups following randomization, and impacts analyses of MT and medication use on symptoms. In this study, because the distribution of medication use was more equal across treatment and control groups, we were able to examine both the relative independent impacts of MT and medication on change in symptoms over time, as well as the moderated impacts of MT due to medication use. To examine comparative effects of MT and medication use, we included change in R2 as a measure of effect size in order to examine the unique contribution of each of these treatment variables to teacher symptoms at each time point.
In addition, in order to help clarify the practical importance of the intervention's effect, and to assess the additive practical benefit of MT above and beyond that of medications, an improvement index was used, based on Cohen's U3. This index converts a program impact into a percentile gain manifested by the target group (Durlak, 2009). The improvement index represents the difference between the percentile rank of the MT mean and the percentile rank corresponding to the control group mean (i.e., 50th percentile) in the control group distribution. Alternatively, the improvement index may be interpreted as the expected change in percentile rank for an average control group teacher when the teacher has been subjected to the intervention.
Results
Study attrition
From baseline to post-program, there was no attrition; however, from post-program to 3-month follow-up, 7% of the treatment group and 15% of the control group dropped out of the study (see Supplementary Materials, Table S1).
Baseline equivalence of groups
Results of t-tests revealed that there were no differences at baseline between groups in levels of depressive or anxious symptoms, or demographic characteristics (e.g., gender, years of teaching experience).
Impacts analyses
Finally, to examine the impacts of MT, medications, and their interactions on depressive and anxious symptoms, a series of hierarchical linear regression analyses were conducted. Results of these impact analyses are presented in Table 5 and Figure 2. As in Study 1, in all models, the strongest predictor of depressive and anxious symptoms was baseline level of these symptoms.
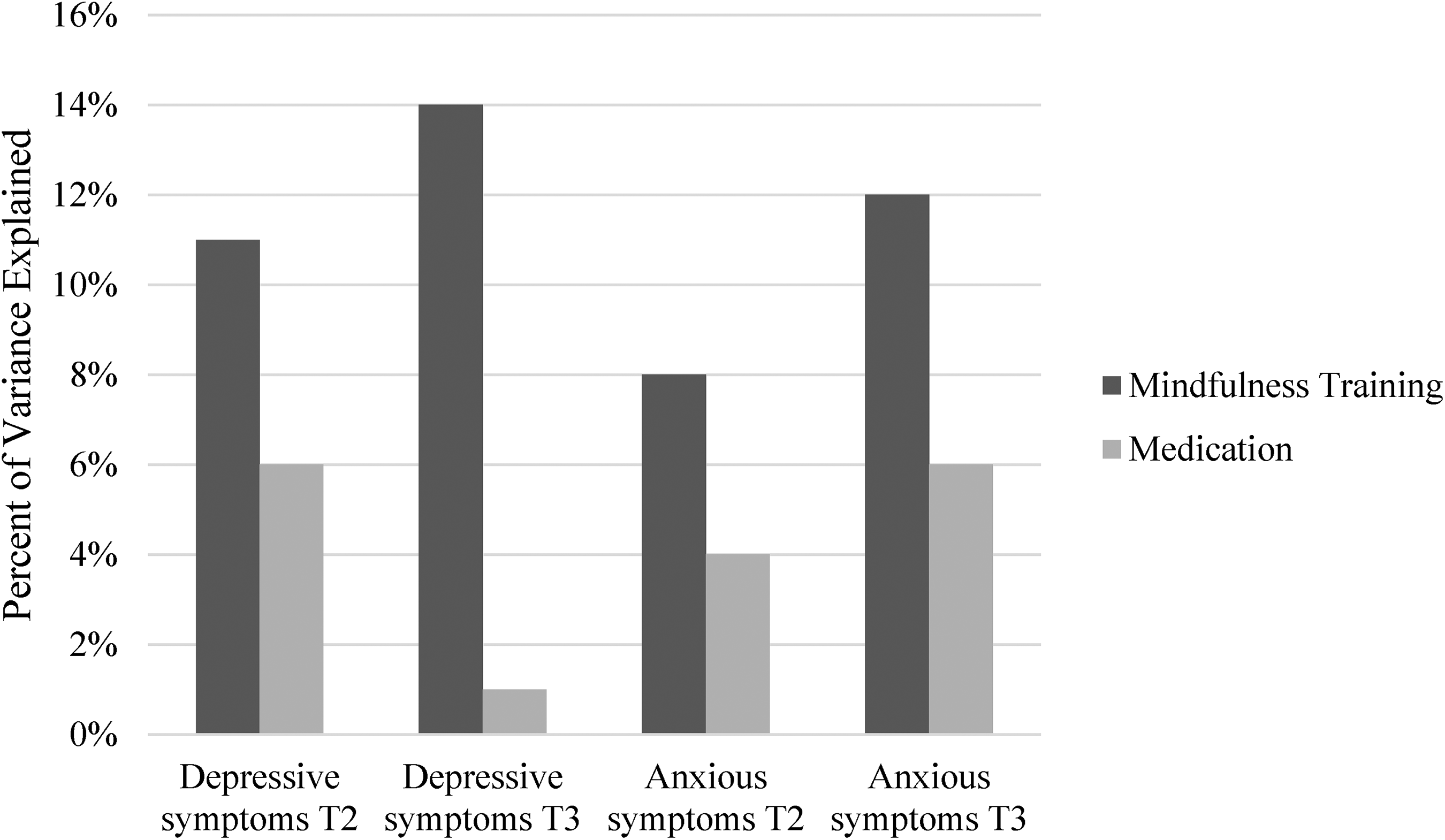
Percentage of variance explained (R2 change) in symptom change based on mindfulness training and medication use (Study 2).
Summary of regression analyses predicting symptoms at post-program and 3-month follow-up in Study 2.
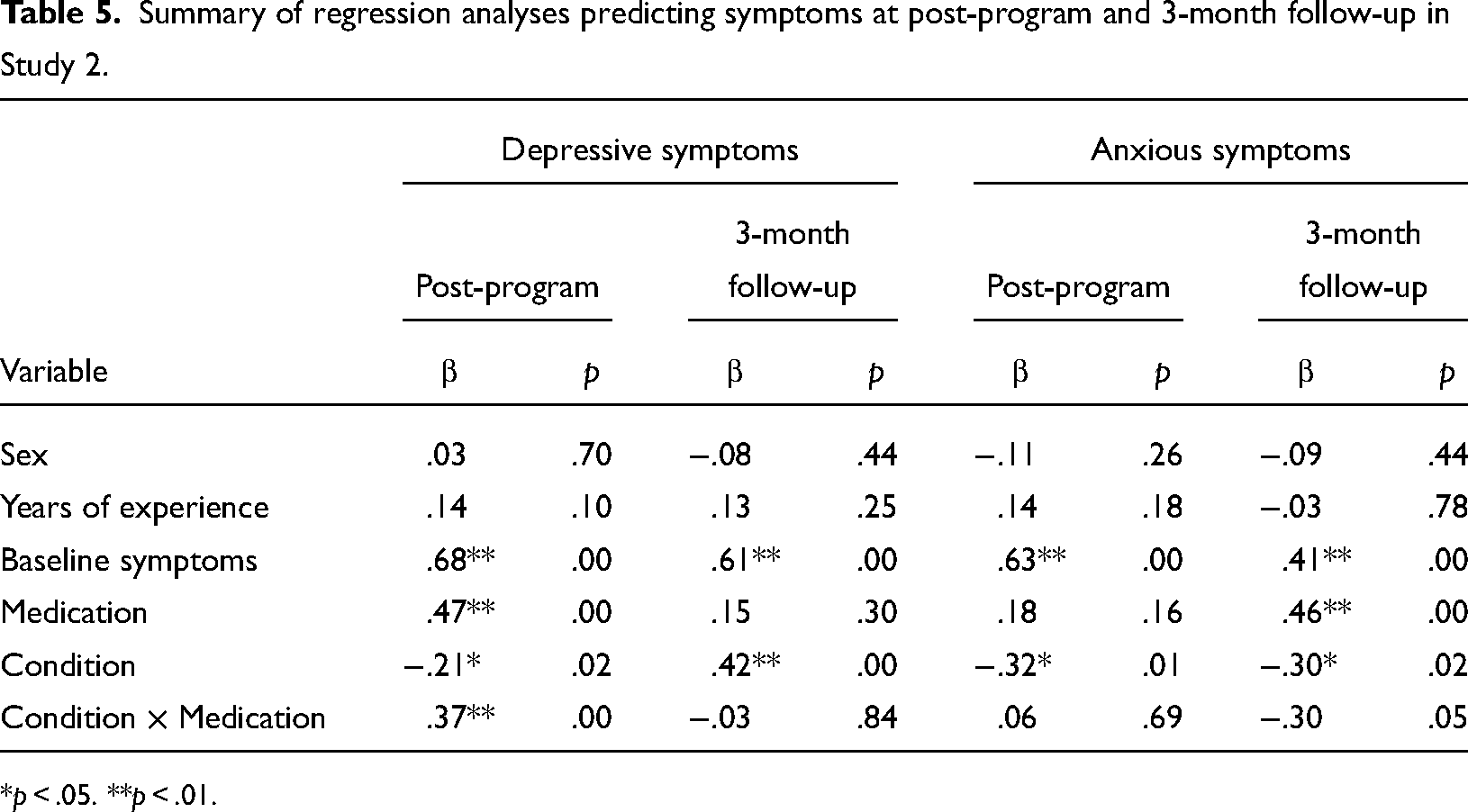
*p < .05. **p < .01.
Depressive symptoms
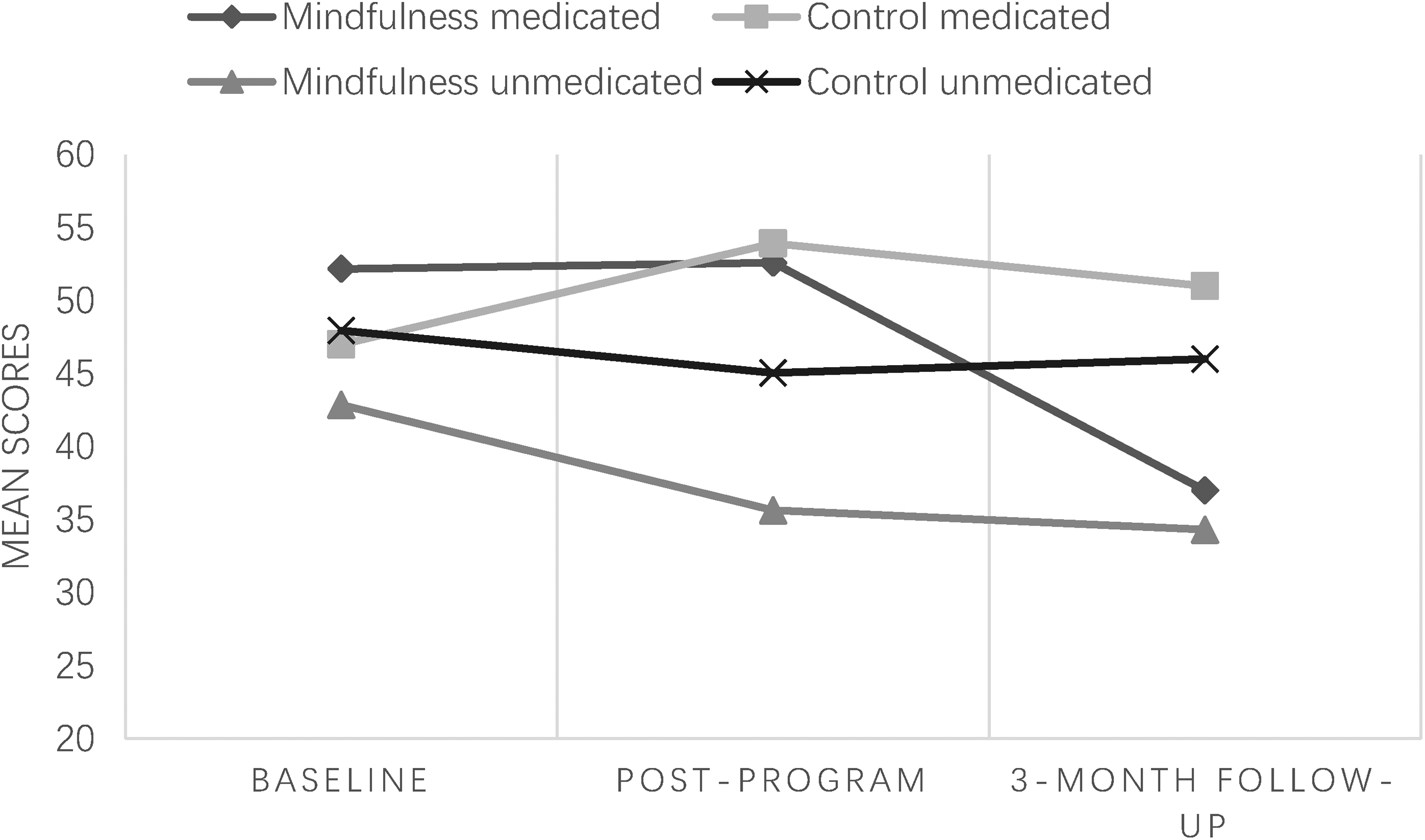
At post-program, both MT (β = −.21, p < .05; R2 change = .11) and medication use (β = .47, p < .01; R2 change = .06) were significant predictors of change in depressive symptoms over time after controlling for the other variables in the model. These main effects were qualified by an interaction between MT and medication on symptom change (β = −.37, p < .001). Analysis of simple effects (Table 6) showed that while effects of MT were significant in both medicated (β = −.75, p < .05) and unmedicated participants (β = −.23, p < .05), the effects of MT were stronger for medicated participants. Further examination of change trajectories in the four groups (Figure 3) suggests that these effects are driven by increases in depressive symptoms at Time 2 for control group participants on medications, who showed a relative increase in symptoms over time. Examination of relative impacts of MT and medication as indicated by the amount of variance explained (Figure 2) indicated that MT explained 11% of the variance in change in depressive symptoms over time, whereas medication explained 6% of the variance in depressive symptom change.
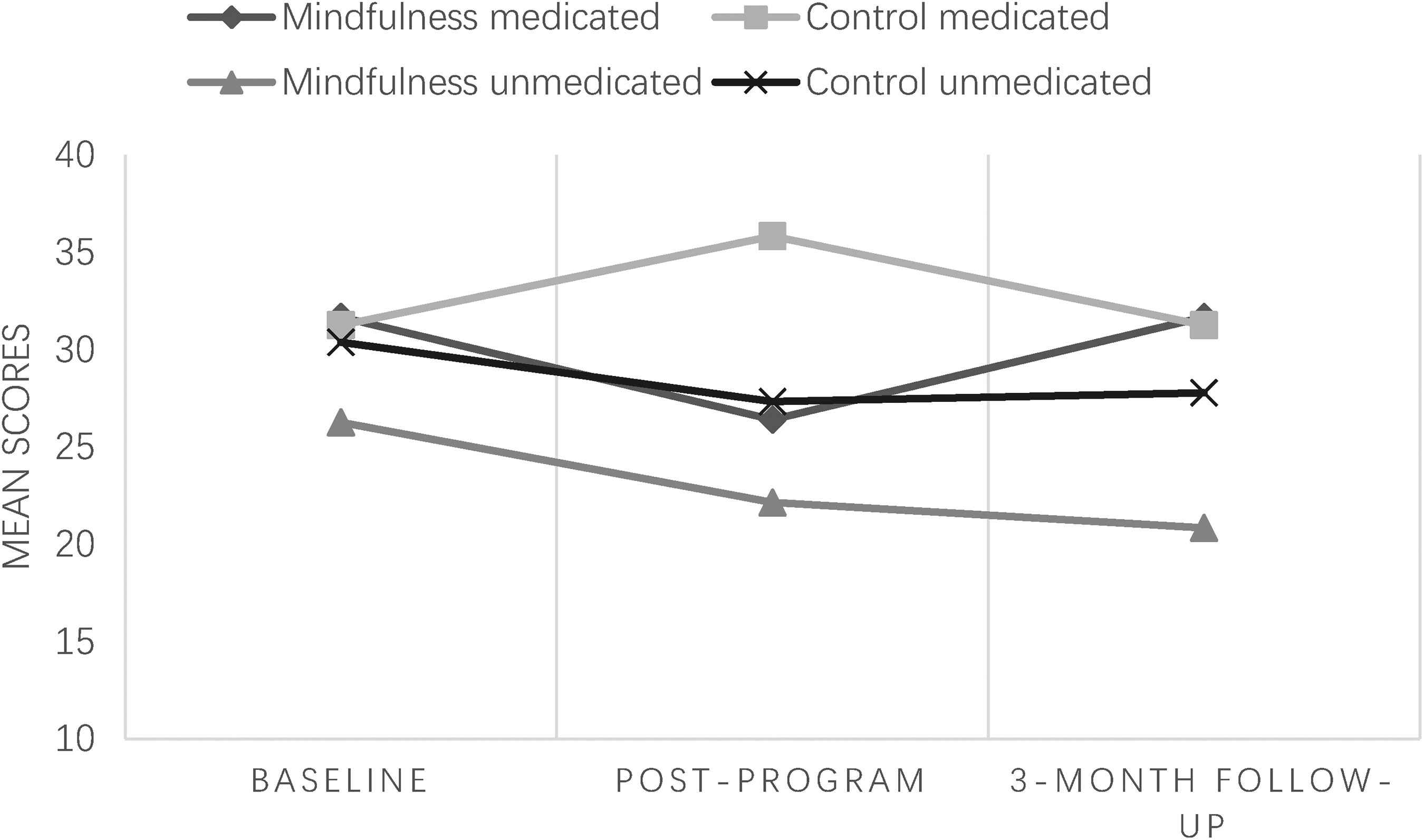
Mean changes in depressive symptoms across all three timepoints by subgroup in Study 2.
Simple effects of mindfulness training on depressive symptoms within each medication group at post-program (T2) in Study 2.
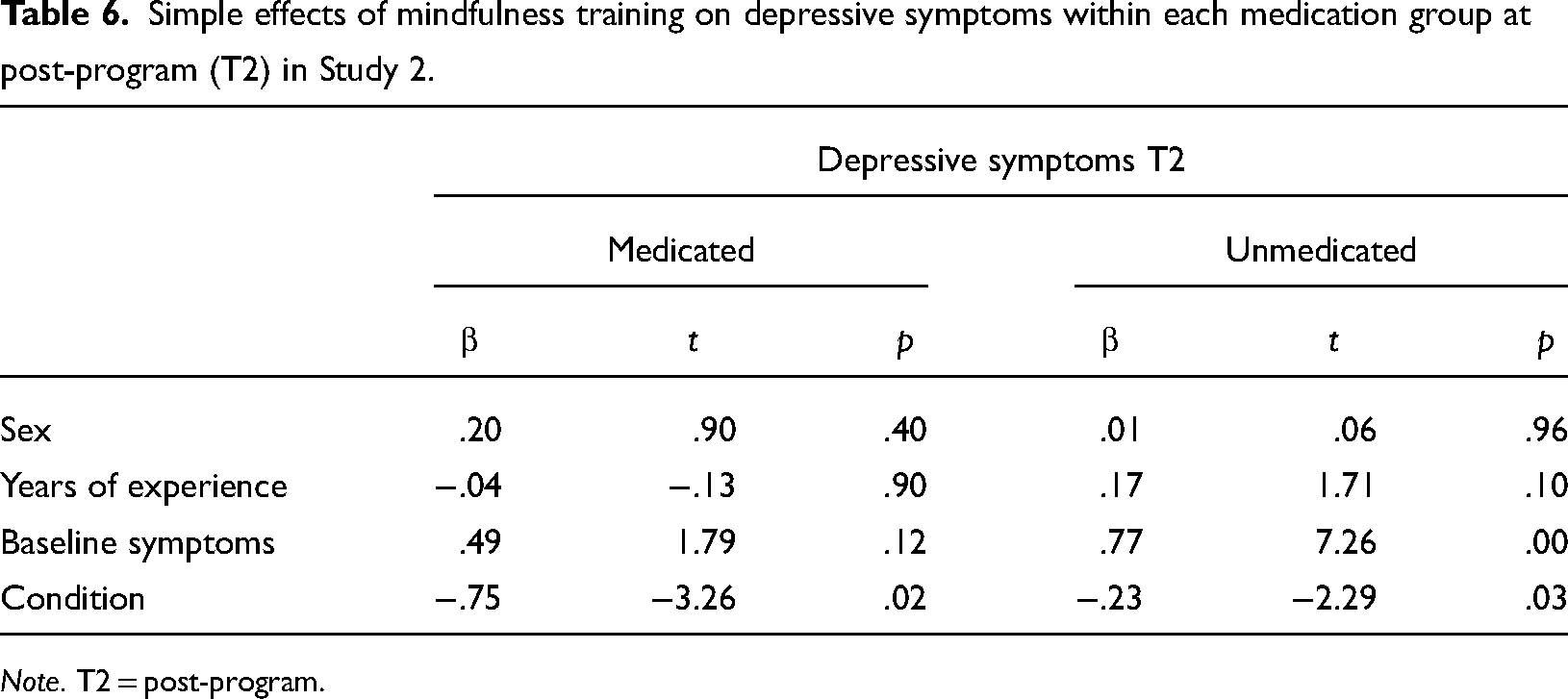
Note. T2 = post-program.
At 3-month follow-up, MT showed a significant impact on change in depressive symptoms over time (β = −.42, p < .001; R2 change = .14) whereas the impact for medication use was non-significant (β = .15, p = .30; R2 change = .01). At follow-up, there was no longer a significant interaction between training and medication on symptom change. Examination of relative impacts of MT and medication as indicated by the unique amount of variance explained (Figure 2) showed that MT explained 14% of the variance in change in depressive symptoms over time, whereas medication explained only 1% of the variance in depressive symptom change at the 3-month follow-up.
Anxious symptoms
Figure 4 depicts the change trajectories in anxious symptoms across the four groups. At post-program, MT had a significant impact on change in anxious symptoms after controlling for other variables in the model (β = −.32, p < .05; R2 change = .08), whereas medication use did not (β = −.18, p = .16; R2 change = .04). The interaction between MT and medication on symptom change was not significant. While MT explained 8% of the variance in anxious symptom change, medication use explained half of that amount (4%; Figure 2).
Mean changes in anxious symptoms across all three timepoints by subgroup in Study 2.
At 3-month follow-up, MT showed a significant on change in anxious symptoms (β = −.30, p < .05; R2 change = .12), as did medication use (β = .47, p < .01; R2 change = .06). The interaction between MT and medication on symptom change was not significant. At follow-up, MT explained fully 12% of the variance in anxious symptom change, while medication use explained 6%.
Relative effects
To assess the practical significance of these impacts of MT, we calculated Cohen's U3 “improvement” index to reflect the average difference between the percentile rank of the mindfulness and control groups on depressive symptoms (Figures 5 and 6). We found a 37% reduction in depressive symptoms post-program, and a 42% reduction in depressive symptoms at follow-up. By comparison, use of medications was associated with a 34% reduction in depressive symptoms post-program, and a 17% reduction in depressive symptoms at follow-up. Regarding anxious symptom reduction, we found a 25% reduction in anxious symptoms post-program, and a 35% reduction in anxious symptoms at follow-up compared to the control condition. By comparison, use of medications was associated with a 37% reduction post-program, which remained the same at follow-up.
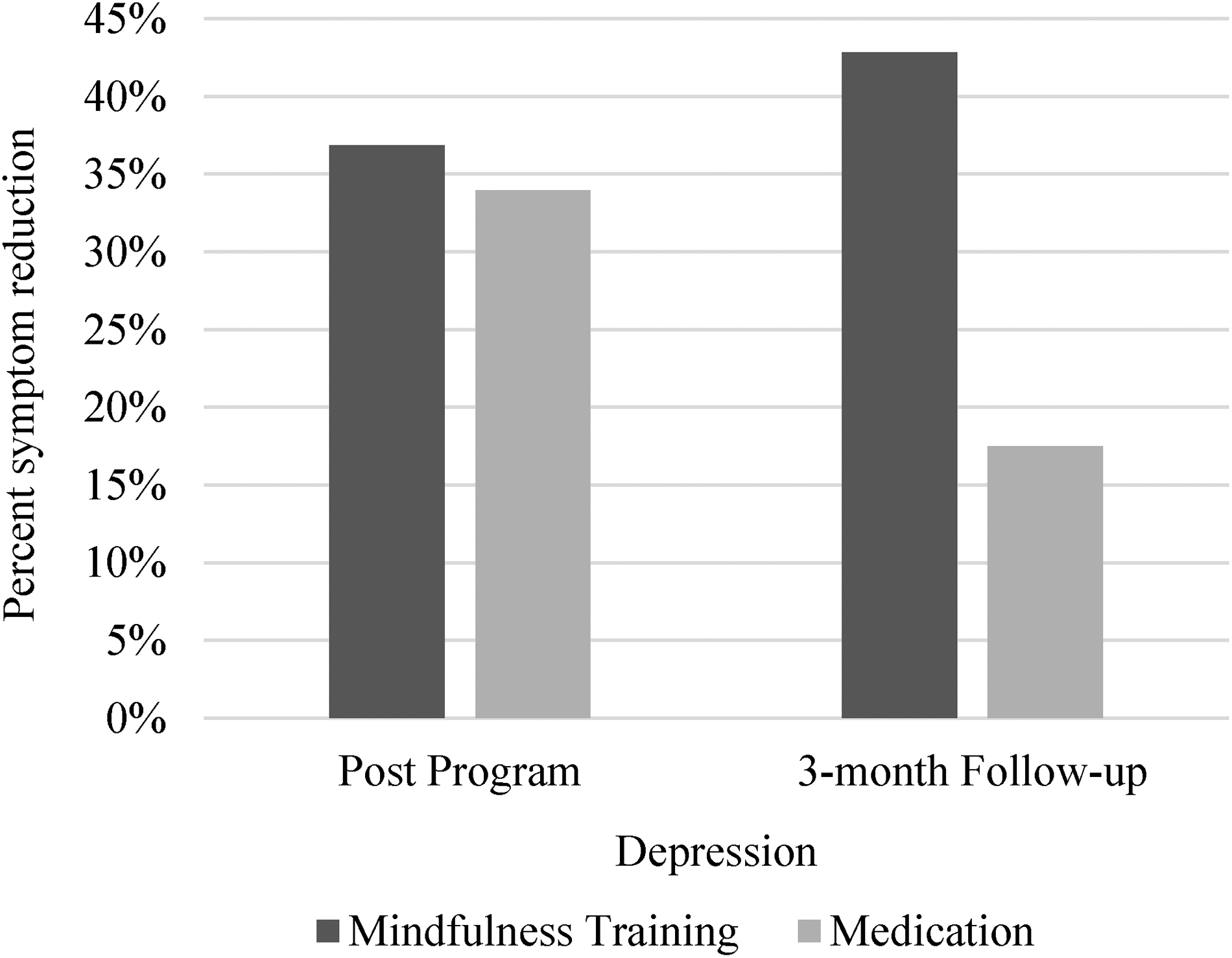
Cohen's U3 effects of mindfulness training on depressive symptoms (Study 2) compared to medication effects at post-program and at 3-month follow-up.
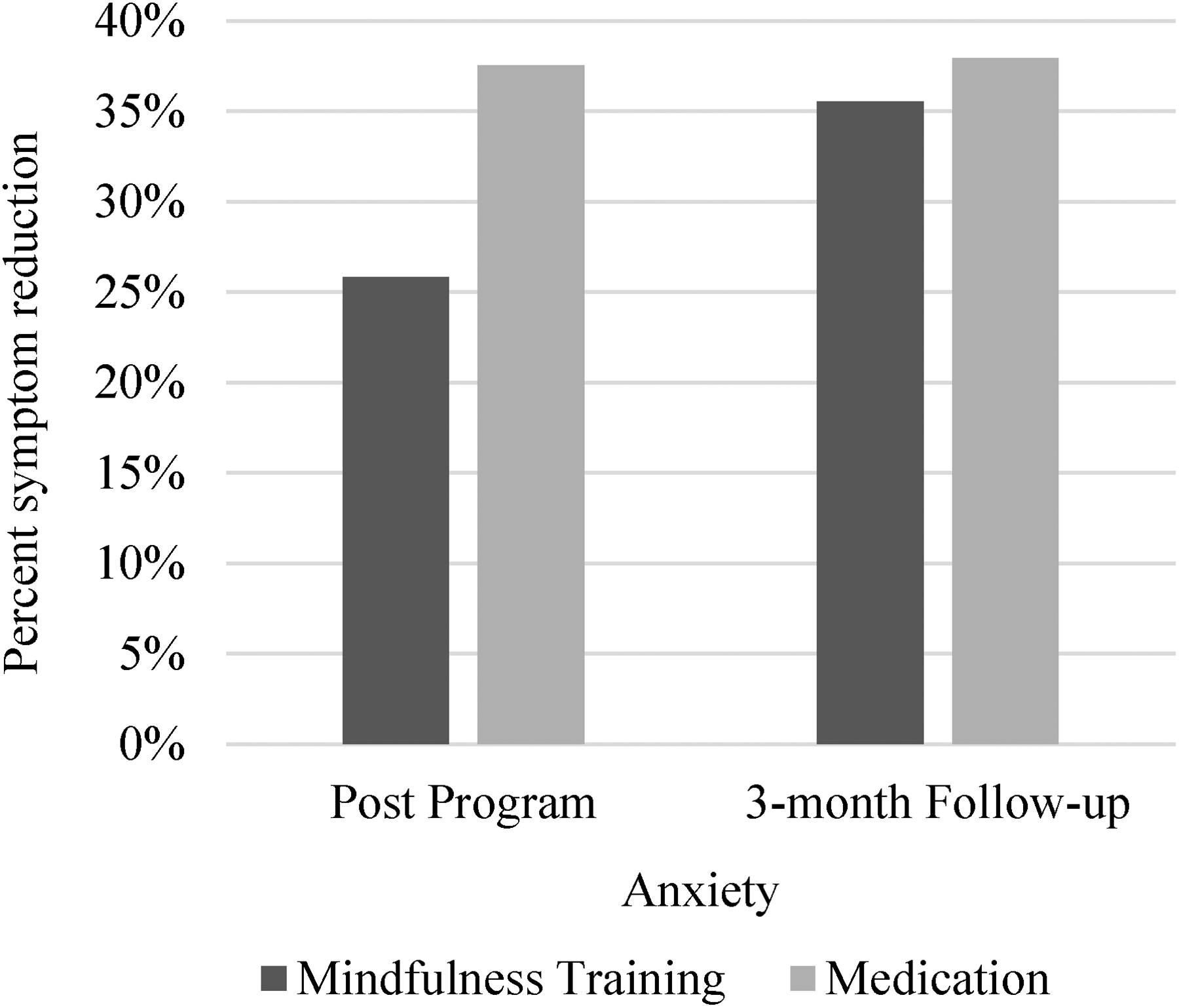
Cohen's U3 effects of mindfulness training on anxious symptoms (Study 2) compared to medication effects at post-program and at 3-month follow-up.
Discussion
The aim of the present study was to investigate the impacts of MT on reductions in depressive and anxious symptoms in public school teachers while accounting for medication use and to investigate the relative and interactive impacts of medications and MT on symptom change over time. Findings across two randomized controlled trials suggest that randomization to MT resulted in significant and consistent reductions in depressive symptoms across both studies as reported in the original RCT paper (Roeser et al., 2013), even after controlling for teachers’ medication use. Furthermore, the effects of MT on depression were generally larger than those of medication in both samples and studies.
The effects of randomization to MT on anxiety were somewhat less consistent, with no significant reductions in anxious symptoms in Study 1, while in Study 2, MT did have a significant effect on anxious symptom reduction when controlling for medication use, and this effect held at the 3-month follow-up. The amount of variance explained by MT in change anxious symptoms (i.e., symptom reduction over time) showed a similar pattern, namely, effects of MT were smaller than that of medications in Study 1, but MT explained a larger proportion of unique variance than medications in Study 2.
Findings dovetail prior literature on the efficacy of mindfulness-based interventions for teachers (Klingbeil & Renshaw, 2018), and add to the literature by studying the effects of MTs on symptom reduction while accounting for medication use. Examination of effect sizes (change in R2) in Study 2 showed the pattern that MT explained more of the variance in symptom reductions in depressive and anxious symptoms at post-program, and that the proportion of variance explained increased at the 3-month follow-up compared to that of medications. Furthermore, the changes in variance explained from post-program to follow-up suggest that the effects of MT accrued over time, so that effects were generally larger at the 3-month follow-up compared to effects of medication. Examination of practical significance effect sizes (Cohen's U3) in Study 2 showed a similar pattern, which may suggest that MT could have a greater long-term impact on reducing internalizing symptoms than do medications, and that individuals may build upon their skills as they continue to practice mindfulness (e.g., Roeser et al., 2022).
It is worth noting that the effects of MT and medications were more consistent for changes in depressive rather than anxious symptoms over time. Findings are consistent with prior literature on mixed effects of mindfulness on anxiety (Bandelow et al., 2015; Gold et al., 2010; Kim et al., 2009). Such mixed findings may arise from differences in how anxiety and depression manifest cognitively (Hong, 2007). Depression involves rumination (Nolen-Hoeksema et al., 2008), while anxiety hinges on worry, which can foster avoidance of feared situations (Borkovec et al., 1983; Newman et al., 2013). MT focuses on present-moment awareness, a core aspect of cognitive behavioral therapy (CBT) for both conditions (Brewin, 1996). However, CBT for anxiety often additionally incorporates exposure to disrupt avoidance patterns, as well as worry-specific interventions (Borkovec & Sharpless, 2004; Newman et al., 1994). Enhancing MT for teachers may involve adding behavioral elements from CBT, such as exposure exercises, to reduce anxiety symptoms. Future research can explore these possibilities.
Overall, study results are in line with conceptualizations of MT as participatory medicine—the idea that mindfulness empowers individuals to take an active role in treatment (Kabat-Zinn, 2000). By participating in skills-based MT that provides tools for managing internalized distress, teachers can continue to improve and deepen their experience of mindfulness over time, resulting in additional long-term benefits. By contrast, medications commonly prescribed for depression and anxiety, such as selective serotonin reuptake inhibitors (SSRIs) and benzodiazepines, have a host of negative side effects, and do not have long-term effects on symptom reduction without continuous use (Morgan et al., 2018). Furthermore, the use of medication as therapy is costly (Vos et al., 2005), while group-based workplace interventions have the potential to save costs for employers and communities (Baicker et al., 2010). Our results suggest that MT could provide an alternative for teachers suffering from internalizing problems, which may provide added value in terms of preventing more serious mental health problems.
The issue of occupational burnout holds significant prominence in the field of education, as evidenced by the departure of approximately 50% of new teachers from the profession within the initial 5 years of their classroom experience (Greenberg et al., 2015; Ingersoll & Smith, 2003). The findings of the current study suggest that mindfulness could emerge as a valuable tool for assisting teachers in managing the substantial daily stress associated with their occupation. By doing so, it has the potential to enhance both their professional and psychological well-being and foster higher retention rates. In this context, embracing mindfulness practices might offer benefits that extend beyond what conventional medications alone can provide for addressing issues of depression and anxiety.
Limitations and future directions
Despite several strengths of these studies, including the use of randomization to test the effects of mindfulness, the use of a community sample from the target population for the intervention, and the use of a well-validated MT program, there are several limitations to our study that should be kept in mind when interpreting the results. First, participants were not block-randomized to receive medications—rather, we conducted our analyses in an exploratory manner based on the available data on teachers’ self-reported medication use. At the same time, due to the naturalistic nature of our approach, it is likely that our results may be more generalizable to real-world settings (Leichsenring, 2004).
Second, the effects of MT and medications were more consistent for changes in depressive rather than anxious symptoms over time. Third, while we screened teachers for participation in other mindfulness-based programs for teachers (e.g., MindUp), we did not screen for participation in other formal or informal mindfulness-based practices (e.g., Zen meditation; yoga). Fourth, the use of a waitlist control group could inflate effect sizes (Cunningham et al., 2013); thus, future MT RCTs are encouraged to use an active control. Fifth, the BSI measure used in Study 1 was based on DSM-III criteria and has not been psychometrically validated in prior work. In the present study, reliability values were .5 from T1 to T3 for anxiety; thus, findings regarding anxiety in Study 1 should be interpreted with caution. Future work should conduct similar studies with validated measures, similar to our Study 2 herein. Finally, the present study did not measure the impact of teacher MT on student outcomes, which could help elucidate how decreases in internalizing symptoms may provide benefits for students via modeling (e.g., increased forgiveness skills; Braun et al., 2020) and more positive teacher–student interactions (e.g., those that are more autonomy-supportive; Roeser et al., 2022).
Limitations notwithstanding, our study presents an exploratory analysis of the effects of MT on internalizing symptoms while accounting for medication use, providing important preliminary findings that can be expanded upon in future research to better serve teachers and school districts, and to ameliorate the various burdens imposed by such distress on teachers, classrooms, students, and districts.
Conclusion
The present study aimed to explore questions that were left unaddressed in previous research on MT for teachers (e.g., Roeser et al., 2013). Overall, the exploratory results presented here showed that MT significantly reduced depressive and anxious symptoms at post-program and at 3-month follow-up when controlling for medication use. Furthermore, comparative effects indicated that MT resulted in more long-term gains for depressive and anxious symptom reduction, while the effects of medication remained relatively stable over time (Study 2). These findings extend those from the original impacts analyses of these two RCTs. Present findings suggest that MT is an effective tool for reducing internalized distress in public school teachers and adds benefits above and beyond the use of medication for such symptoms in this population. If replicated in future RCTs that block-randomize for medication versus MT among participating teachers, these results hold promise for ameliorating teacher distress and providing cost savings to schools and the healthcare system.
Supplemental Material
sj-docx-1-roe-10.1177_20965311241265122 - Supplemental material for Exploring the Relative Impacts of Mindfulness Meditation and Medication Use on Changes in Teachers’ Internalizing Symptoms Over Time
Supplemental material, sj-docx-1-roe-10.1177_20965311241265122 for Exploring the Relative Impacts of Mindfulness Meditation and Medication Use on Changes in Teachers’ Internalizing Symptoms Over Time by Natalia Van Doren and Robert W. Roeser in ECNU Review of Education
Footnotes
Contributorship
This research was conceptualized by Natalia Van Doren and Robert W. Roeser. Natalia Van Doren conducted the formal analysis of the data and drafted the manuscript. Robert W. Roeser supervised the project, provided guidance on the methodology, collected the data for the RCTs, and reviewed and edited the manuscript. Robert W. Roeser also secured the funding for this research and managed the project administration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Both studies had IRB approval and the consent of the adult participants. The human subjects protocol numbers for the two studies are as follows: Vancouver, Canada Study 1 = IRB #09783; Boulder, USA Study 2 = IRB #101178. Both studies were reviewed and approved by Portland State University.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by the National Institute on Drug Abuse (T32DA017629 and T32DA007250). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse or the National Institutes of Health. The research reported here was also supported in part by the Edna Bennett Pierce Endowed Chair in Care and Compassion at the Pennsylvania State University held by the second author.
Notes
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.