
Abstract
Introduction
Hypertrophic scarring is a common and debilitating consequence of burn scars. While there is limited evidence for current treatment options, laser therapy has been shown to be effective, low risk and minimally invasive. This study assesses the use of carbon dioxide lasers and intense pulsed light devices in the treatment of hypertrophic burn scars.
Methods
In this case series, patients were recruited from a hypertrophic burn scar waitlist and completed a Patient and Observer Scar Assessment Scale prior to and six weeks after laser therapy. The Nordlys (intense pulsed light) and CO2RE (carbon dioxide) systems from Candela Medical were used, with a range of settings used depending on the assessment of the burn scar. The differences between scores were calculated for the total Patient and Observer Scar Assessment Scale score, pain, itch, colour, stiffness, thickness, irregularity and the overall opinion of the scar. Statistical analysis was completed using a paired, two-tailed student T test.
Results
A total of 31 patients were recruited for this trial with a range of scar locations, surface areas and mechanism of burn injury. The calculated difference in mean showed a significant reduction for the overall Patient and Observer Scar Assessment Scale score (1.93, p < 0.0001), pain (1.39, p = 0.0002), itch (1.84, p = 0.0002), colour (1.97, p < 0.0001), stiffness (2.47, p < 0.0001), thickness (2.1, p < 0.0001), irregularity (1.89, p < 0.0001) and overall opinion (1.58, p = 0.0003).
Conclusion
Current management options for hypertrophic scarring have limited evidence. Laser therapy presents a minimally invasive procedure that can be completed under topical anaesthetic and has shown to be effective following a single treatment of combined carbon dioxide laser and intense pulsed light device therapy.
Lay Summary
Many people will suffer a burn injury throughout their life and up to almost 3 out of 4 people with burn injuries will suffer from hypertrophic scars (a thickened, red and itchy scar). These scars cause distress both due to their appearance and their reduction of function, particularly over a joint or muscle. Laser therapy, in which different wave lengths of light (pulsed light) or gas (carbon dioxide) target the scar, has been found to be effective and have minimal side effects in the management of hypertrophic scars. While individual lasers have been assessed and found to be effective and low risk, the combined use of multiple lasers on the same scar has not been extensively studied. We studied the effectiveness of both light and gas laser therapies on hypertrophic scars. Patients with hypertrophic scars completed a questionnaire that focused on their perspective of their scar (pain, itch, stiffness, thickness, irregularity, overall opinion) prior to the treatment. The patients then underwent laser therapy (with local anaesthetic gel) with either pulsed light and/or carbon dioxide (gas) laser. The type of laser used was decided by the clinician performing the therapy depending on scar location and thickness. Patients then re-completed the subjective survey six weeks following the laser therapy, and the results compared. We learnt that laser therapy (both light, gas and a combination of both) are effective (and low risk) in reducing the subjective burden of the scar for the patient.
Keywords
Introduction
Each year, over 5000 people are hospitalised in Australia due to burns related injuries. 1 Many of these patients develop significant scarring with 32 to 72% of burn victims developing hypertrophic scars, 2 which often result in pain, functional limitations, and significant psychological burdens for patients.3,4 Hypertrophic scars are defined as unchecked proliferation of fibrous tissue where the scar does not extend beyond the original boundaries of the wound. 5 The pathophysiology of hypertrophic scar formation is not well understood, however, it is thought to be due to abnormal collagen deposition during the wound healing process. 6
Normal wound healing is described in three stages: inflammation, proliferation, and remodelling.5,7 The inflammatory stage begins immediately with activation of the coagulation and inflammatory pathways to obtain haemostasis. 7 The inflammatory process recruits macrophages which are thought to coordinate the scar and wound healing process. 7 Proliferation of new tissue occurs between days 2 and 10 post injury and involves migration and proliferation of keratinocytes, myofibroblasts, fibroblasts and angiogenesis. 7 This process is largely driven by a variety of growth factors. 7 Myofibroblasts are contractile cells which allow the edges of wounds to come together, and the interaction of myofibroblasts and fibroblasts creates collagen (mainly type III collagen) which provides the substance of the scar. 7 Finally, the third and final stage of remodelling begins two weeks post injury and can continue for many years. 7 During this phase, many cells undergo apoptosis, and the cellular matrix undergoes remodelling from type III collagen to type I collagen. 7 Current evidence suggests that in hypertrophic scars, the myofibroblasts do not undergo apoptosis following the second stage of wound healing, leading to prolonged collagen formation and contracture of the cells.5,8 Histologically, hypertrophic scars contain increased amounts of type III collagen, compared to type I collagen, indicating an error in the second and third stages of wound healing. 6
Many therapies have been trialled for the treatment of hypertrophic scars, with limited success. Topical silicone gel is a common treatment which may provide some benefit for burn scar management, however there is poor quality evidence in the literature to support this.9,10 Pressure garments are also commonly used to treat hypertrophic burn scars, however there is conflicting evidence in the literature with some studies showing no benefit. 9 There has also been conflicting evidence in combining both silicone gels and pressure garments in the treatment of hypertrophic burn scars. 9 Studies have indicated that intralesional corticosteroid injections are a beneficial treatment option, however these are associated with issues of pain and recurrence. 5 Surgery offers an effective treatment option for hypertrophic scars and can be used to release contractures and improve mobility. 6 However, surgery is an invasive procedure that requires hospital admission and predisposes to new scar formation.6,8
The development of lasers and other resurfacing modalities such as intense pulsed light (IPL) have introduced a minimally invasive and effective treatment for hypertrophic burn scars.8,11–13 Laser therapy has been shown to be more effective than other non-surgical treatment options. 9 From an analysis of 51 studies, Willows et al. 11 concluded that laser therapy was both effective at treating hypertrophic scars, as well as safe and low risk with minimal adverse events. When compared with surgical treatment options, laser therapy is less invasive with a low risk profile, as treatments can be performed in an outpatient setting with topical anaesthetic.11,14 Minor adverse events such as post-inflammatory hypo- or hyper-pigmentation, erythema and infection are reported to occur in approximately 20–30% of patients,11,14 with no severe adverse events reported in the literature.11,15 Laser therapy and other resurfacing modalities have been introduced in multiple international burns centres in Australia with evidence that it reduces length of hospital stay, anaesthetic time and non-laser reconstructive procedures.16,17
There are many types of devices currently used in the treatment of hypertrophic burns scars. Lasers have a variety of therapeutic targets depending on the device and mechanism, including reducing abnormal scar development as well as promoting healthy tissue growth. It is understood that laser therapy can be used to decrease abnormal collagen production in cells, either through damage to abnormal collagen, or through promoting healthy collagen production, depending on the type of laser therapy.8,12 Non-ablative therapy options include pulsed dye lasers (PDL) and intense pulsed light (IPL) systems and are known therapies for port-wine stains, capillary malformations and haemangiomas by targeting the pathological vascularisation of hypertrophic burn scars13,18 IPL devices target chromophores by delivering a narrow spectrum of focused light energy which can be adjusted to achieve its desired effect depending on the wavelength of light energy used.18,19 For example, a low wavelength of 515 nm can treat rosacea, while a higher 755 nm wavelength can stimulate collagen production. 18 IPL is excellent in the treatment of hypervascularity as well as treatment of dyspigmentation. The aim of IPL in hypertrophic scars is to reduce vascular proliferation and pigmentation in the field of rapid collagen growth. 19 It has demonstrated impressive results in the management of hypertrophic burn scars, with a significant improvement in scar characteristics and patient satisfaction following the treatment. 20
In contrast to the IPL devices, carbon dioxide (CO2) lasers are particularly useful in hypertrophic scars where the abnormal dermis can be vaporised, which in turn promotes altered collagen production and remodelling, increasing collagen III deposition, and reducing collagen I.12,18,19 CO2 lasers also have the ability to provide targeted penetration, with minimal damage to surrounding tissues resulting in improved wound healing.18,19 The use of CO2 lasers in hypertrophic burn scar management has been shown to reduce scar thickness, improve symptoms of pain, pruritis and aesthetics of the scar, even in mature scars that were resistant to other management options.17,19,21–25
While there are many studies assessing the use of IPL devices and CO2 lasers individually in the treatment of hypertrophic scars,23,26 there are few studies assessing the combined use of both IPL devices and CO2 lasers. Studies that have assessed the combined use of both devices have found positive impacts on the improvement of scars, compared to the use of individual devices.12,27
Given the effectiveness and low risk nature of laser therapy, a feasibility trial was performed to assess the use of CO2 lasers, IPL devices, and a combination of these in the treatment of hypertrophic burn scars at the Victorian Adult Burns Services (VABS) in Melbourne, Australia.
Methods
All techniques and procedures were approved by the Ethics Committee of the Alfred Hospital, Melbourne, Australia (project number 335/22). Written informed consent was obtained from patients involved in this study for their de-identified data and clinical photography to be used in the publication of this research. Following data collection, patient data was de-identified and anonymised through the removal of identifiers such as hospital ID numbers, name and date of birth.
Patients that were on an existing waitlist for steroid injection for hypertrophic burn scars were approached and assessed for their suitability for this trial. Additional patients with persistent and symptomatic hypertrophic burn scars not improved through conservative therapies (such as silicon creams and pressure garments) for at least three months or minimal response to previous steroid injections were approached for inclusion in this study. Patients were provided with written information explaining the procedure, risks and benefits of the IPL device or CO2 laser treatment and their demographical information was obtained together with written informed consent.
Exclusion criteria included patients with a history of infection with a multi-resistant organism, and history of chronic pain who are unlikely to tolerate the procedure under topical anaesthesia only.
The treatment session was conducted as a day procedure in the operating theatre. Patients attended clinical photography prior to the laser treatment and completed a questionnaire that contained the pre-treatment Patient and Observer Scar Assessment Scale (POSAS). A skin swab was taken from the area to be treated to detect the presence of microorganisms in case the patient were to develop an infection from their treatment. For patients receiving CO2 treatment, topical anaesthetic (BLT cream containing 14% Benzocaine, 7% Lignocaine and 4% Tetracaine) was applied to the target area at least 30 min prior to the CO2 laser treatment. Patients receiving IPL alone treatment did not receive topical anaesthetic. For those patients receiving a combined IPL device and CO2 laser therapy, topical anaesthetic was applied following IPL treatment and prior to CO2 laser therapy. This is due to the small possibility of BLT cream constricting vessels, potentially reducing the efficacy of IPL device treatment. 28 Each treatment area was wiped and cleaned with moist gauze and alcoholic swabs prior to commencing the treatment and therapy. This ensured a clean, sterile field for treatment, as well as removing any topic anaesthetic which may have the potential to interfere with the penetration of the therapy device. Each treatment took approximately 20 to 30 min based on the surface area treated.
The Nordlys and CO2RE systems from Candela Medical were used for this trial. The Nordlys system has a quartet of technologies which include different IPL handpieces with a set filter (400 nm, 530 nm and 555 nm, 600 nm, 645 nm), two non-ablative fractional treatment handpieces (Frax 1550 and Frax 1940) as well as Nd: YAG 1064 nm. In this study, we primarily used the VL555 handpiece to treat the vascular component of the scar, which is the preferred handpiece for darker skin types and allows deeper penetration of vascular and pigmented lesions including, but not limited to, lesions such as telangiectasia, and rosacea.29,30 The CO2RE system is a fully integrated CO2 laser with six different treatment modes, including four fractional ablative treatment modes, five pattern shapes, a traditional resurfacing mode, an excision mode with defined shape, and a freehand mode for minor dermal excisions. This CO2 laser has a spot size of 0.15 mm with a pulse duration that ranges from 0.02–3 ms.19,31 It can reach a depth of 20–750 µm and can deliver <90 mJ of energy per treatment spot.19,31 It delivers an average power of 30 W and a peak power of 60 M to an overall scanned area of 10 × 10 mm.19,31 This laser has four fractional ablative treatment modes: light (20–40 µm), mid (100–200 µm), deep (500–700 µm), fusion (combination of superficial and deep fractional resurfacing). 31 In this study, the fusion programme was the most frequently used setting as it targets collagen remodelling at various levels. The mid programme is useful for light resurfacing with minimal hypertrophic scarring. The fractional density ranged from 3% to 40% and the ring energy between 2 mJ to 94.7 mJ. The core energy ranged from 50 mJ to 130 mJ.
In terms of pre-operative considerations, the characteristics of the scar determine the type of treatment that will be administered. Each patient's scar was assessed by the treating clinician on the day of treatment. The type of device used (IPL only, CO2 only or combined use of both devices), as well as the settings, were determined by the treating clinician depending on the Fitzpatrick skin type of the patient, the anatomical location of the scar, the vascularity and thickness of the scar. The vascularity of the scar was assessed by measuring the capillary refill of the scar, and the size and depth of the vessels. If the patient's natural skin colour is light brown, the VL applicator of the IPL device is preferable. The VL applicator is useful for treatment of “blue or purple” vessels which are located deeper in the epidermis and often slightly larger. 32 It can also be used to treat notable brown pigmentation caused by sun damage. 32 If the patient's natural skin colour is pink, the vessels are often smaller and located closer to the skin surface and would respond better to the PR handpiece. 32 The chilled gel was applied to the region prior to the IPL treatment to protect the epidermis from thermal injury and allow uniform delivery of the light to the surface of the skin. The Nordlys system can generate a default setting based on the clinical parameters entered. While the default setting is often on the lower end of the therapeutic window, it is a safe setting that that allows for spot testing to determine the correct treatment parameters. The expected clinical end point is rapid colour change to a white or blue colour within less than one second for telangiectasia and diffuse redness. For port wine stains, a longer lasting colour change to blue is observed in the treated vessels, with rapid onset of oedema followed by erythema. If there is a lack of reaction after the test spots, it usually indicated that a more effective result can be achieved by increasing the energy slightly. In this setting, we often increase the energy by 1–2 mJ/cm2 and repeated a test spot to ensure effective and correct settings were used.
For the assessment of the CO2 laser, the thickness of the scar determined the depth of treatment required and this was assessed by clinical measurement in our study. While there are newer devices such as optical coherence tomography and confocal microscopy that can offer a more objective assessment, 33 we did not have access to these technologies for our study. For the majority of hypertrophic burns scars, the deep mode and the fusion mode are preferred due to the depth of penetration. The deep mode can penetrate 500–750 micron below the skin's surface providing deep treatment to improve the surgical and traumatic scars. 31 The fusion mode combines the mid and deep setting depositing energy at both 100–200 and 500–750 micron depths improving skin tone and texture as well as the appearance of the scars, all in a single treatment pass. 31 It is particularly useful in addressing some of the superficial contour irregularity from a meshed skin graft. The energy setting for fusion is between 45–128 mJ (mid) and 30–70 mJ (deep). Similar to the IPL device, a test spot is performed using the default setting, and the energy can be increased based on clinical response.
In terms of post procedure management, the treated area was dressed with Bactigras and gauze, and secured with a crepe bandage or Hyperfix. Patients were instructed to keep dressings intact for 24 h and apply Dermeze ointment to the wound until it was fully healed. Following this, patients were encouraged to continue their usual scar management, including silicone gel or sheet and wear compression garments again. The patient received a phone call follow up at one week post treatment and a face-to-face review at six weeks post treatment. At the six-week follow up appointment, patients completed post-laser therapy clinical photography and a post treatment Patient and Observer Scar Assessment Scale (POSAS).
The main outcome measure for this study is the POSAS score. This is a subjective scale that allows patients to assess the quality of their own scars including pain, itch, colour, stiffness, thickness, irregularity and their overall opinion of their scar. 34 Each of these sections is scored from 1–10, with 1 being ‘like normal skin’. In this study, patients were asked to complete the POSAS before their laser treatment and at six weeks post treatment. The score from each section, excluding the overall opinion of the scar, was combined, and averaged to provide an average value for each patient's scar score. The difference between the pre and post laser therapy scar score average was calculated and a paired, two tailed student T test was conducted to identify the significance, with a p value of <0.05 indicating a significant result.
A further outcome measure is the average of each section individually; pain, itch, colour, thickness, stiffness, irregularity. The difference between pre and post laser means was identified and subjected to a paired, two tailed student T test to identify significance. In addition to the POSAS scar scale, patients were asked to score their comfort of the procedure at the six-week follow up appointment, from 1 to 10, with 1 being ‘extremely comfortable’.
The overall POSAS score for each method of laser therapy was a further outcome measure. The overall POSAS score was stratified into CO2 only, IPL only and combined CO2 laser and IPL device treatments. The difference between the POSAS scores was calculated and subjected to a paired, two tailed student T test to identify significance.
Statistical testing was completed in GraphPad Prism and the normality of the data was assessed using the D’Agostino-Pearson normality test.
Results
A total of 33 patients underwent laser therapy. Two of the patients were lost to follow up at six weeks due to moving interstate, therefore only 31 patients were included in the final analysis. Table 1 outlines the patients’ demographics. The majority of the patients had received multiple previous treatments for their original burns, resulting in 48 different previous surgical treatments across 31 patients. Some of the patients also underwent laser therapy on multiple sites, therefore giving a total of 36 different scar locations across 31 patients.
Patient demographics (n = 31).

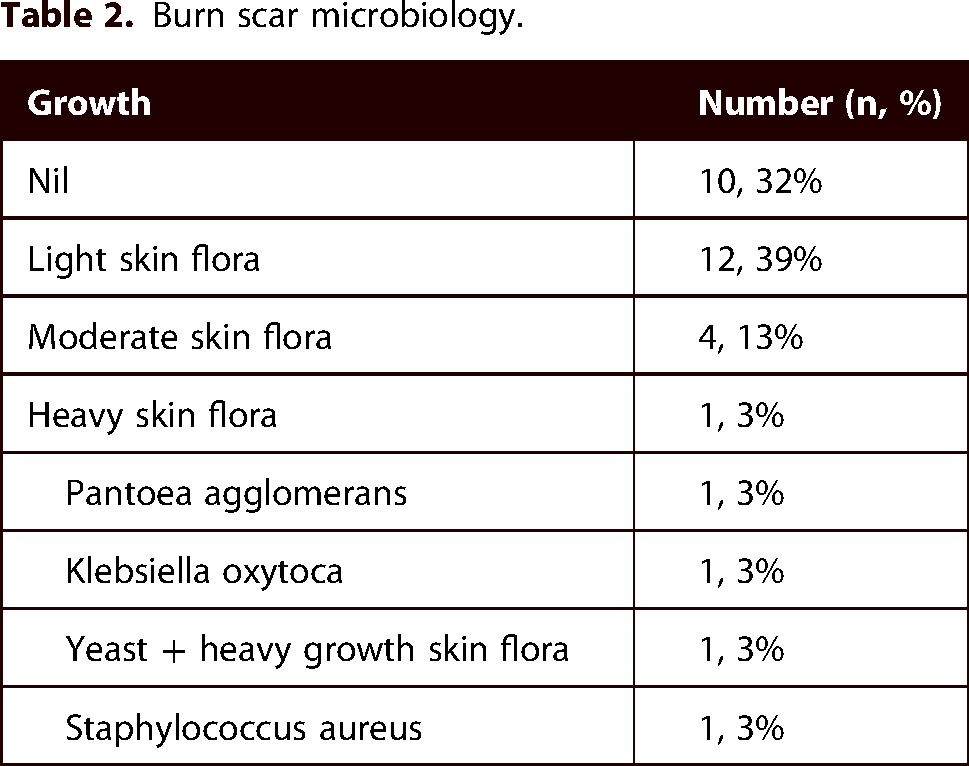
Table 2 identifies the microbiology obtained from the burn scar prior to laser treatment. Ten patients did not grow any microorganisms; however, 17 patients had a variety of normal skin flora. The wound swab of three patients grew a pathological organism; however, these did not result in post treatment infections (Table 3).
Burn scar microbiology.
Details of laser therapy provided.

The details of the laser therapy provided to patients are described in Table 3. Eleven patients received ablative fractional CO2 laser only, while three patients received IPL only. Seventeen patients received a combination of CO2 and IPL during their treatment. Twenty-six (83.6%) patients had topical anaesthetic applied to the treatment area prior to the laser therapy. The majority of patients (90.32%) did not suffer from any adverse events or complications following their treatment; however two patients developed a minor infection requiring one course of oral antibiotics.
The POSAS scar scale results for all patients regardless of treatment device are shown in Table 4. The mean of all the patients’ POSAS score prior to laser therapy was 6.38, while the mean score post laser therapy was 4.46. This indicates a mean difference of 1.93 which was found to be statistically significant (p < 0.0001). The mean difference between pre and post scores are also shown for each individual section, pain (1.39, p = 0.0002), itch (1.84, p = 0.0002), colour (1.97, p < 0.0001), stiffness (2.47, p < 0.0001), thickness (2.1 < 0.0001), irregularity (1.89, p < 0.0001) and overall opinion (1.58, p < 0.0003) all of which were found to be statistically significant (p < 0.05). Eight patients were unable to complete the irregularity score on the POSAS, and therefore the irregularity scar score was calculated with a sample size of 23, rather than 31. The mean score for the comfort of the procedure was 3.98, with 1 being ‘no discomfort’ and 10 being ‘extremely uncomfortable’.
POSAS results pre-laser and six weeks post laser treatment.

*Irregularity was not completed correctly by eight patients. This section therefore has a sample size of 25, rather than the total of 31.
Table 5 identifies the overall POSAS means and the difference in mean when stratified according to the laser therapy received. A statistically significant difference in mean was seen for both the CO2 (2.45, p = 0.0007), and combined IPL and CO2 (1.84, p < 0.001) groups, while the difference in mean in the IPL group alone was not significant (0.56, p = 0.3485).
Overall POSAS results stratified into type of laser treatment.

Figures 1–6 show clinical photographs from before the laser therapy (Figure a) compared with photographs six weeks after the laser therapy (Figure b). Figures 1 and 6 show the result of CO2 only laser therapy, while Figures 2–5 show results from combined CO2 and IPL laser therapy.
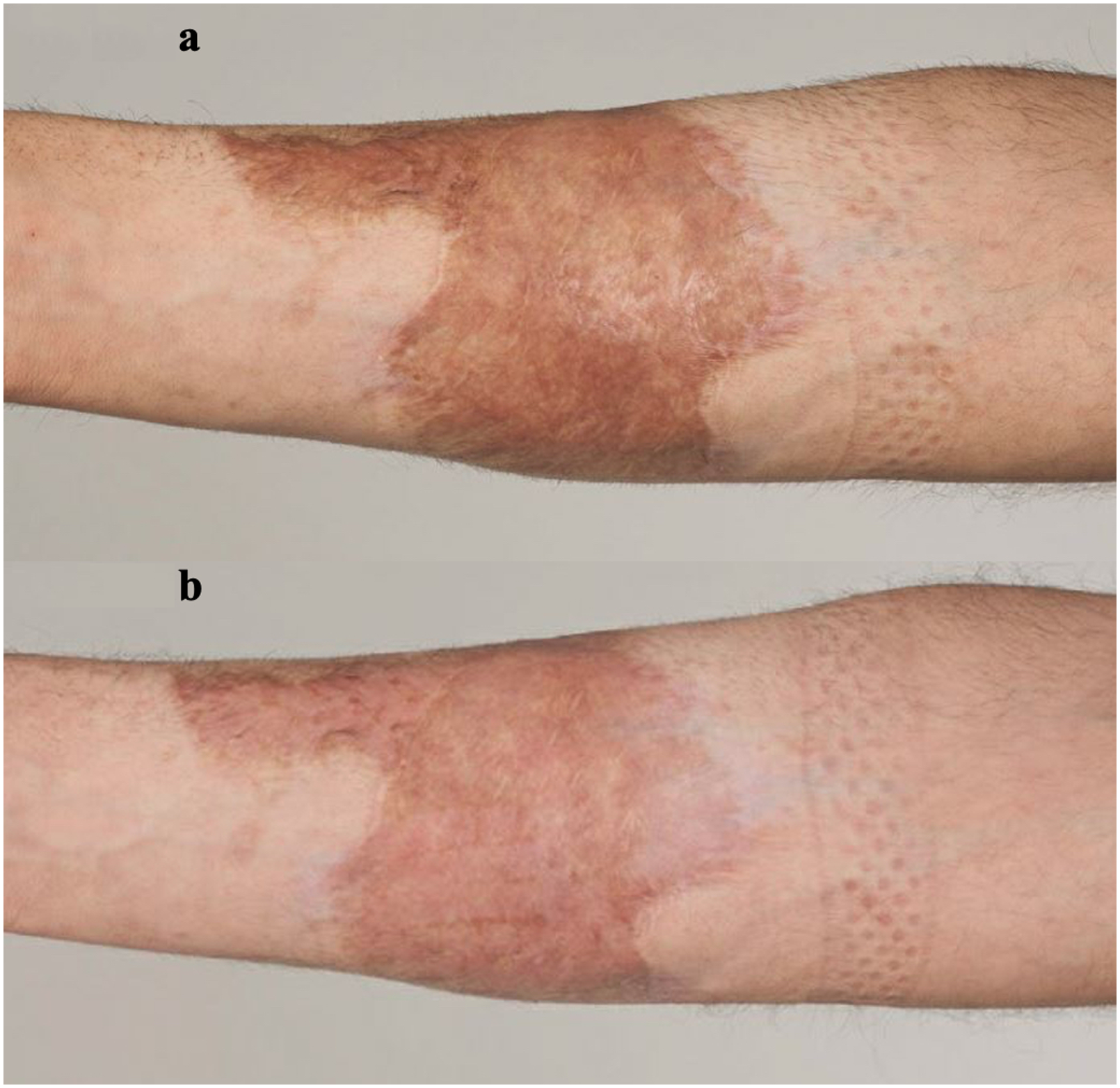
26-year-old male with a 16-month-old scald burn to the right forearm. (a) Shows the scar prior to laser treatment. (b) Indicates the scar six weeks after CO2 only laser therapy. Fusion mode setting was used at 35% fractional density with a ring energy of 87.6 mj and a core energy of 60.0 mj. This was overlaid with a deep mode at 5% fractional density and a core energy of 50.0 mj.

54-year-old female with a five-month-old flame burn to the left hand. (a) Shows the scar prior to laser treatment. (b) Indicates the scar six weeks after combined CO2 and IPL laser therapy. This was the first laser treatment for the patient. The PR 530 handpiece was used for three passes. The first pass had a pulse width of 1.5 mg with 5 J. Second pass had a pulse width of 5.5 ms with 6.7 J. The third pass had a pulse width of 10 ms with 7.6 J. The number of passes and setting was based on the clinical end point after each pass. This was followed by treatment with a CO2 laser with deep mode at 5% fractional density with core energy of 78 mJ, and mid mode with 30% fractional density at 94.7 mJ.

33-year-old male with a 45-month-old flame burn to the chin and neck. (a) Shows the scar prior to laser treatment. (b) Indicates the scar 6 weeks after CO2 and IPL laser therapy. This was the first laser treatment for the patient. We performed three passes of CO2, first in fusion mode with 40% fractional density, ring energy of 80.6 mJ and core energy of 70 mJ. Second pass was with deep mode at 5% fractional density and 79 mJ ring energy. The third pass was with mid the CO2 laser settings with 25% fractional density and ring energy of 94.7 mJ.

39-year-old female with a five-month-old scald burn to the left flank. (a) Shows the scar prior to laser treatment. (b) Indicates the scar six weeks after CO2 and IPL laser therapy. This was the first laser treatment for the patient. The VL555 hand piece at 1.5 ms pulse width and 2.1 J energy was used for the first pass to address the vascularity of the scar. This was followed by deep mode CO2 at 5% fractional density and ring energy of 80 mJ.

28-year-old male with a five-month-old flame burn to the left shoulder and arm. (a) Shows the scar prior to laser treatment. (b) Indicates the scar six weeks after CO2 and IPL laser therapy. This was the first laser treatment for the patient. The CO2 laser settings included a mid and fusion treatment modes. The VL555 hand piece with 1.5 ms pulse width at 2.3 mJ was applied as first pass. This was followed by fusion mode at 40% fractional density and ring energy of 84.6 mJ and core energy of 76 mJ. Second pass included mid mode with 39% fractional density at 94.7 mJ.
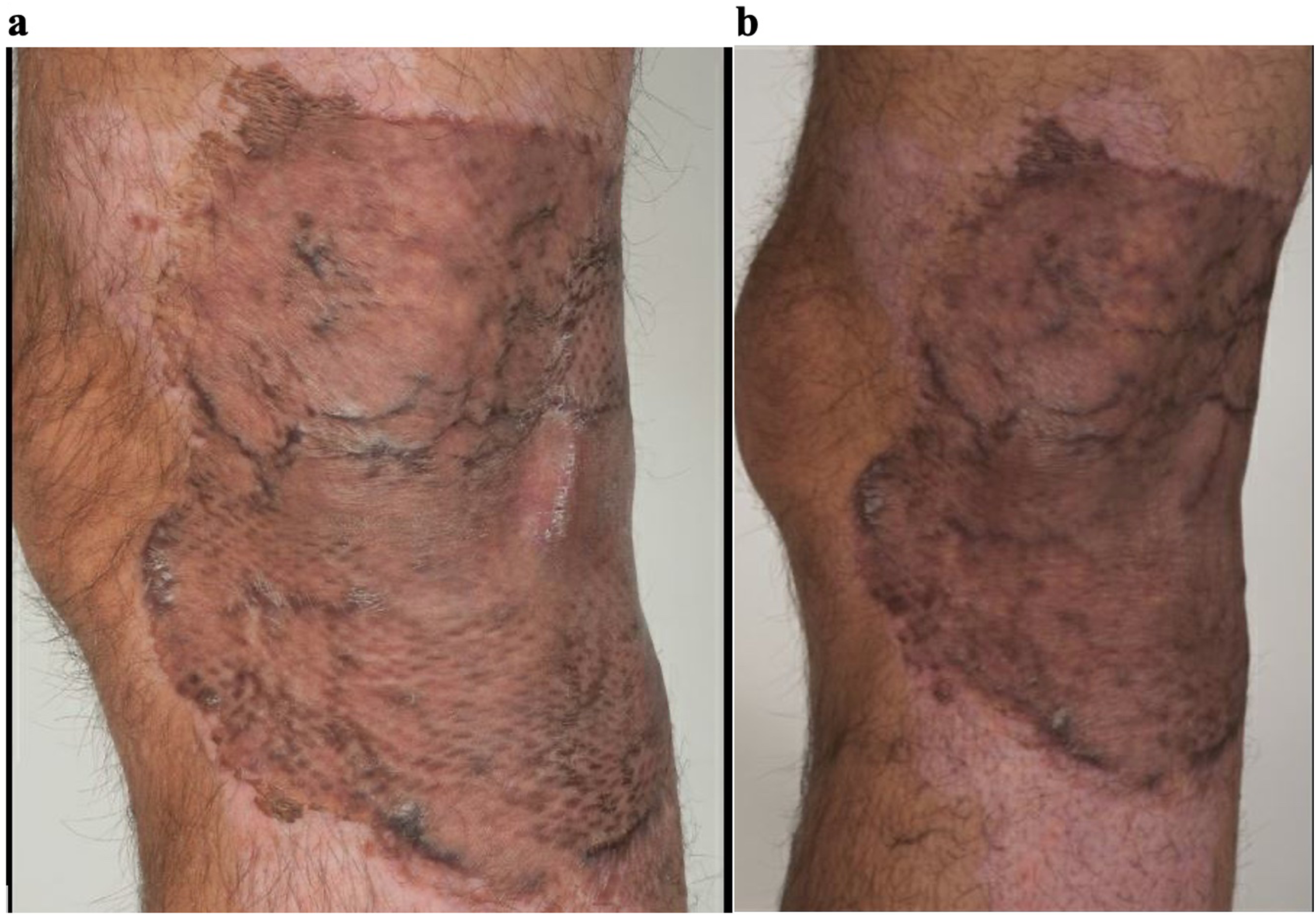
31-year-old male with a five-month-old scald burn to the left popliteal area. (a) Shows the scar prior to laser treatment. (b) Indicates the scar six weeks after CO2 only laser therapy. This was the first laser treatment for the patient. The CO2 deep mode with 3% fractional density and 80 mJ was used.
Discussion
This study aims to assess the use of CO2 laser and IPL device in the treatment of hypertrophic burn scars at a single burns centre. The results from Table 4 indicate that the combined use of CO2 and IPL devices as well as CO2 lasers alone have significantly improved the patient's subjective opinion of their scar. An improvement of 1.93 points on the overall POSAS scar scale is seen, which is statistically significant with a p value of <0.0001 (Table 4). Furthermore, there was a statistically significant improvement in every section of the POSAS score following the laser therapy (Table 4). Many studies in the literature have provided evidence for the effectiveness and benefit of laser therapy and non-ablative resurfacing therapy23,26 and this study further supports the benefit of CO2 laser and IPL devices in patients suffering from hypertrophic burn scars. It is important to note that these results are following a single session of laser therapy only, and patients typically undergo five to six sessions of laser therapy. 26 The statistically significant benefit seen from one session of laser therapy in this study is therefore important to consider, and that additional laser sessions in the progression of this study in the future will most likely produce further benefits.
A limited number of studies have analysed the use of a combination of CO2 lasers and IPL devices in the treatment of hypertrophic scars. 27 This current study has identified that the use of CO2 (2.45, p = 0.0007) laser alone, as well as a combination of CO2 and IPL (1.84, p < 0.001) results in a statistically significant reduction in the overall POSAS score from before and after the laser therapy (Table 5). Interestingly, the use of IPL device alone (0.56, p = 0.3485) did not result in a statistically significant result (Table 5), however it is important to note that the sample size for IPL alone treatment was only three patients (Table 3). While IPL devices have been shown to be beneficial as a sole treatment modality, they are commonly used in combination with other treatment modalities, such as CO2 lasers (as in this present study), intra-lesion steroids and pulsed dye lasers. 19 The role of IPL devices as a sole treatment modality and on hypertrophic burns scars could be explored further with studies that include larger samples sizes in this treatment group in the future.
There are a range of IPL and CO2 systems available for use that target hypertrophic scars. This study used the Nordlys and CO2RE systems from Candela Medical which provides a range of treatment options. The Nordlys IPL device offers a single multi-application platform compared to the traditional single platform device such as a pulse dyed laser. The Nordlys system also offered the Frax 1550 and Frax 1940 as well as Nd: YAG 1064 nm handpieces. 30 While we did not include these handpieces in our study, they can certainly be used for non-ablative fractional treatment for skin surfacing, which can help to improve the texture of skin grafts in burns patients. The Nd: YAG can also be used to treat deeper vascular lesions.30,32 The HR handpiece can also be used to reduce hair follicles in patients who have recurrent burns scar folliculitis.
While the CO2RE system has slightly less depth of penetration compared to some of the other CO2 device that can penetrate as deep as 1600 µm, 19 it was able produce a statistically significant benefit in our case series. It is also a more affordable and more compact machine compared to some of the other similar devices. While the results and benefit of CO2 lasers seen here may be extrapolated to other CO2 model lasers, the exact benefit of each device would need to be individually tested and a comparison between the effectiveness of each device would be beneficial in future studies.
Furthermore, this study analysed the potential link between microbiology and the risk of infection following the laser therapy. Over 85% of patients grew varying degrees of normal flora on the pre-treatment wound swab (Table 2), while a pathological organism was cultured on the wound swab of three patients. Interestingly, these pathological organisms did not result in a clinical infection following laser therapy, as only two patients developed a minor infection following the treatment (Table 3). Staphylococcus aureus is a common organism that infects burn wounds35,36 while Klebsiella oxytoca and yeast species rarely cause infections in immunocompetent patients.37–39 Pantoea agglomerans is a plant pathogen which rarely causes infection in burns patients. 40 Importantly, all of these pathogens may cause an infection in an acute burn injury, however there is limited evidence to identify their role in chronic burn scar infections.
Laser therapy and IPL devices are a low risk, minimally invasive procedures with very limited examples of severe adverse events documented in the literature.11,14 Minor adverse events are reported to occur in 20–30% of patients11,14 which is supported by the findings of this study, in which 6.45% of patients suffered from minor adverse events such as an infection requiring antibiotics (Table 3). All of the patients in this trial found the procedure quite comfortable, rating it an average 3.98 out of 10, with 10 being ‘extremely uncomfortable and painful’ and 1 being ‘extremely comfortable’ (Table 4). This is important as all of the procedures were either performed without anaesthetic (for IPL treatments) or under topical anaesthetic (for CO2 and combined treatments) to reduce the pain and discomfort of the procedure, which ensures that the laser treatments can be performed in the outpatient setting. Furthermore, many patients have expressed interest in receiving further laser therapy sessions, voicing the improvement of their scars as well as the ease, comfort, and speed of the procedure (Online Appendix 1).
Although this study indicates a statistically significant benefit of CO2 lasers and IPL devices on hypertrophic scars, this study is not without limitations. Firstly, the POSAS score traditionally requires two subjective assessments of the scar in question, the patient's assessment as well as an observer's assessment. 34 The use of a clinician or third-party observer as the observer's assessment could be implemented to reduce bias and error in the scar score. Furthermore, eight patients in this study failed to correctly complete one section of the POSAS scar scale (irregularity). These inconsistencies resulted in changes in the calculation of the results and may highlight some errors and biases in the results. The use of a subjective outcome measure presents an inherit recall bias which could be avoided with the use of an objective outcome measure in the assessment of scars before and after laser therapy. 25 Newer technologies and devices such as optical coherence tomography, non-linear technique such as second harmonic generation microscopy, confocal microscopy, as well as colourimeter devices can be used to provide better structural, vascular and pigmentation assessment of the scar. 33 This will allow clinicians to better understand and measure how various treatments alter the scar characteristics. While there is no current gold standard assessment of burn scars,41,42 a more objective assessment of the scar will also help to separate patients into different cohorts based on the scar characteristic, and therefore develop more transferable and reproducible clinical results. Future studies may also consider randomising patients to treatment groups to reduce treatment bias associated with subjective assessment of the scar. Finally, the low sample size reduces the power of this study. Particularly the low sample size of the IPL only group makes the interpretation of findings and stratification of results difficult. Further studies should aim to include a higher number of participants to allow for more accurate assessment and stratification of each individual treatment device.
This study has assessed the use of CO2 lasers and IPL devices on hypertrophic burn scars. It is important to acknowledge that there are many other lasers and devices that are currently being used to manage these conditions including the pulsed dye laser which has the potential to prevent the development of hypertrophic scars from burns wounds. 19 It would be interesting to further compare the results from this study with other treatment options to provide a review of current laser management options.
While laser therapy provides a safe and effective management for hypertrophic burn scars, there are limitations to the introduction of this service to a burns unit. Firstly, clinicians and hospitals require access to a laser which can be expensive and provide logistical issues. 18 Furthermore, staff must be adequately trained and complete safety courses to operate the laser, 18 and regular theatre and clinical allocation is required. Issler-Fisher et al.16,25 have demonstrated the use of CO2 laser potentially reduces the overall costs associated with burn scar reconstruction by reducing the need for surgical scar revisions. Future studies should consider a cost effectiveness analysis of a laser service to better identify the barriers or benefits related to this service. Another point to consider is that support from anaesthetic and pain services will be required for patients with a higher total body surface area of burns that will not be adequately covered by topical anaesthetic. The risk of post operative infection may also be higher in patients who have a larger area of treatment as well.
Despite some of the logistical limitations to laser therapy, it is frequently completed as a day procedure and it will provide a reduced cost of care and resource allocation, when compared to surgical scar management.18,43 The implications of this study on the economic, financial and resources allocation for laser therapy compared with other treatment options for hypertrophic scars should be assessed and considered in future research.
Conclusion
Hypertrophic scarring is common and debilitating for burn victims. Currently there are many treatments available for hypertrophic scarring, however there is limited evidence to support these, or they include invasive and resource consuming surgery. The development of laser therapy has opened new doors in the treatment of hypertrophic burn scar management, with increasing amounts of evidence supporting the improvement of scars. Laser therapy can be performed with topical anaesthetic and yields impressive results. This study has identified a good response following a single treatment of combined CO2 laser and IPL device therapy which will provide a good adjunct to the other scar management services offered by any burns service.
Supplemental Material
sj-docx-1-sbh-10.1177_20595131231202103 - Supplemental material for The use of carbon dioxide and intense pulsed light laser for the treatment of hypertrophic burn scars: A case series
Supplemental material, sj-docx-1-sbh-10.1177_20595131231202103 for The use of carbon dioxide and intense pulsed light laser for the treatment of hypertrophic burn scars: A case series by Sophia Dahm, Geoffrey Lee, Heather Cleland, Hana Menezes and Sally Ng in Scars, Burns & Healing
Footnotes
Acknowledgements
The authors acknowledge Candela Medical and the Candela technicians who aided in the use of the laser therapies, as well as the other clinicals and nursing staff who assisted in patient preparation and follow up.
Authors contributions
SN selected patients, obtained patient informed consent and completed the laser treatment of patients. GL obtained ethics. SD analysed and interpreted the data obtained for this study and completed the article, under the supervision of SN. All authors read and approved the final manuscript.
Availability of data and materials
All data, including raw data used for all figures and analysis, is available upon request to the corresponding author from three months following article publication to researchers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.