
Abstract
Introduction
The role of postoperative scar tissue adhesion and its impact on motor control in infants with congenital heart disease has not been explored in the literature. Elastic therapeutic tapes, such as Kinesio tape, are designed to affect the integumentary system. This case report aims to demonstrate the safety and present the observations following use of Kinesio tape to treat scar tissue in a pediatric patient after open-heart surgery in conjunction with standard rehabilitation.
Method
This retrospective case report presents observations of an infant's sternotomy scar adhesion and gross motor development after six applications of Kinesio tape. The sternotomy and drain tube scars were treated with Kinesio tape fascia applications in addition to standard physical therapy (PT).
Discussion
Several domains showed positive changes. The scar mobility and appearance improved. The patient's motor skills improved, possibly due to skin stretch's role in motor learning. The taping application did not cause discomfort, and there were no adverse reactions.
Conclusion
In this infant, the three-month-old sternotomy scar improved in adherence and appearance after six applications of Kinesio Fingerprint tape; motor skills also increased in the presence of standard PT. There were no adverse reactions noted with the protocol. Kinesio tape may provide a safe adjunct to treat scar tissue adhesion in infants with median sternotomy scars.
Lay Summary
Issue being explored
Sternotomy scars can cause physical and psychological harm. Sensors (receptors) in the skin help with movement and balance responses. The impact of scar stiffness (adhesion) on developing motor control has not been reported in infants. Treating the scar in the remodelling phase with elastic tape may improve the scar's appearance and ability to move, thereby improving development.
Introduction
Congenital heart disease (CHD) is the most common congenital disability, impacting over 1.35 million infants internationally. 1 With surgery, 90% of these newborns survive into adulthood 2 ; however, physical and psychological co-morbidities often affect their quality of life.3–6 Of patients with CHD, 70% are aged <1 year, 7 and over half of these infants present with developmental delays. 8
Median sternotomy scars often have a poor outcome. Hypertrophic or raised scars usually form when incisions are perpendicular to Langer lines or the natural tension lines found in the skin.9–14 This often leads to limited satisfaction due to discoloration, pruritis, 12 chronic pain15,16 and contracture.3,7 Common psychological co-morbidities of sternotomy scars are poor body image and embarrassment.1,9,10 In the case of children, this is concerning to parents as it can cause decreased self-esteem and quality of life.17,18 The problem is so extensive in paediatric patients that research has been directed towards less invasive surgical techniques9,11,14,16–21 and postoperative management.22–25 To date, the most promising strategies have been alternative surgical techniques and silicone gel sheeting; however, only safety, cosmesis and pain have been used as outcome measures. The impact of scar adhesion on motor development has not been explored in this population.
pediatric open-heart surgery accounts for 22,000 7 of the 70 million pediatric scars acquired annually. 3 Assessment of the quality and impact of postoperative scar tissue should be a part of a comprehensive pediatric evaluation as it is estimated that 38%–70% are pathological. 26 Treating surgical scars may be necessary as the skin is so neurological it is termed the diffuse brain. 27 Its ability to deform to stimulate sensory receptors plays a critical role in motor learning. 28 Deficits in the skin impair function 29 ; thus, scar adhesions could impact motor control.
Scars are associated with many physical co-morbidities, including functional deficits.3–6 Sternotomy scars are noted for causing pain and contracture.3,7 While there are many treatments for scar tissue, there is no standard of care established for pediatric populations; thus, inferences must be made from adult research. 3 Kinesio tape (KT), designed to improve skin mobility and provide afferent feedback, shows initial evidence of scar remodelling. It is well established that skin stretch is fundamental to motor learning27–29; however, the specific impact of scar adhesion to movement acquisition in infants has not been explored. This case observes changes in motor skills and scar tissue adhesion in the presence of standard physical therapy (PT) and home programme interventions after the use of KT for scar treatment.
Non-invasive scar treatments
A meta-analysis demonstrates that physical scar treatment significantly reduces many co-morbidities compared to no treatment. 23 Non-invasive therapies include manual techniques (i.e. scar massage)22,30,31 and topical agents (i.e. silicone sheets and onion extract).22–25 KT has preliminary evidence of scar improvement across various pediatric and adult populations.32–34 Low tension applications (<50% tension) impact superficial fascia, improving mobility 24 and 48 h after application.35,36 Kinesio Fingerprint (FP) tape is designed for low-tension applications to create lift. It is 100% cotton, uses an acrylic adhesive and can be worn for three days in children.37,38 Two studies have used Kinesio FP tape immediately after median sternotomy to influence edema and found it decreased pain and improved respiratory perception with no adverse reactions.39,40
Developmental motor scales
The data collected in this retrospective case were chosen specifically for the child's age. The Alberta Infant Motor Scale (AIMS) and the Gross Motor section of the Peabody Developmental Motor Scale second edition (PDMS-2) have strong content validity; the AIMS is more sensitive to at-risk infants aged <9 months. 41 The AIMS is a norm-referenced assessment using observation of 58 skills in four positions (prone, supine, sitting, standing). Each noted skill is given 1 point until the highest skill has been reached. These items are summed and given a rank percentile. 41 Likewise, the PDMS-2 is a norm-referenced test containing six subscales divided into fine and gross motor skills. The gross motor subtests include reflexes, balance, locomotion and object manipulation. 41 Observation of each skill is scored between 0 and 2, depending on the task's description. These subsets are summed and ranked based on age. The three subsets are converted into standard scores and added to produce a gross motor quotient. The Faces Leg Activity Crying Consolability scale (FLACC) is a pain scale in the range of 0–10, with 0 being no pain, validated for use in children aged ≥2 months. 42
Standardised scar assessments
The Patient and Observer Scar Assessment Scale (POSAS) is the most used scar assessment. 43 It has two sections, the patient and the observer scales. The patient scale is not validated for a parent to complete on behalf of their child; it was omitted. The treating therapist completed the observer scale. The POSAS contains six questions regarding the scar's characteristics (colour, pliability and sensation) compared to the patient's typical skin. The clinician rated on a scale of 1–10 then added up the total. 43 The score can be in the range of 6–60 based on the observer's perspective. Lastly, the Adheremeter, a valid and reliable tool, measured scar adhesion. 44 The Adheremeter is a transparent tool with concentric rings to measure skin excursion in millimetres. The skin's mobility is measured in four directions. This process occurs on the scarred skin and typical skin to create a ratio called the adhesion severity index; the closer one is, the more regular the skin. 44
Case report
A three-month-old infant presented to PT with a diagnosis of delayed milestones; he had a history of CHD due to a defect of the pulmonary vein. This required surgical correction 12 h postpartum. He was in a medically induced coma with an open chest cavity for two weeks. Two months later, he was discharged after receiving gastric tube placement due to difficulty with oral feeds. He was three months postoperative and had a well-closed sternotomy scar.
The mother was concerned about the scar appearance, difficulty with tummy time and poor oral intake. She also noted persistent fisting of the right hand. The PT administered the AIMS and the PDMS II. Adhesion severity (AS) for the scar was assessed using an Adheremeter and scar appearance with the Observer portion of the POSAS. He also presented with a Grade I congenital muscular torticollis and Type II deformational plagiocephaly. An early intervention referral was made based on the developmental findings; however, he did not start other services until later.
Consent and review
The mother understood the treatment purpose and method. She signed the written participation agreement and a release of information for publication. The Institutional Review Board of the University of Indianapolis reviewed this retrospective case study, and it received exempt status (01512).
Intervention
The patient was seen once a week for standard PT care, including parent education, neuro-developmental treatment strategies for body awareness, prone position play skills, traditional torticollis management, family training and scar treatment using the KT fascia application. A test patch was applied at the initial evaluation, and application began the following week. The FP tape was cut to cover the sternal and drain tube scars. The standard Kinesio long-short fascia application process created tension between 25% and 50%. 45 The tape started at the xiphoid process and was applied along the sternum to end at the manubrium. The second piece was similarly applied to the drain tube scars (Figure 1). Family training occurred on proper removal after three days of wear. There was one instance where the mother forgot to remove the tape for seven days; it was removed at the PT session.

Kinesio taping application.
Measurements
The FLACC assesses the level of comfort. This was a 3 at the initial evaluation, which did not increase with the tape application. This decreased to 2 after three treatments, with the parent reporting increased prone tolerance. After five sessions and tapings, he scored 0 with improved prone play and less fisting of the right hand, which could be due to increased tummy time.
Standardised testing was assessed after the sixth taping application. Adhesion severity (AS) was evaluated after the first, third, sixth and seventh applications. Overall, the AS improved from 0.008 to 0.233 over six applications; the conservative minimal detectable change is 0.20 44 (Table 1). The POSAS improved 50% (Figure 2). The AIMS and PDMS II were also re-assessed after six applications. The AIMS score improved by 42.5%, while the PDMS II decreased by 10%; however, it is not as sensitive to an infant’s change (Table 2).

Scar progression: pretreatment; after three tapings; after six tapings; and three months later.
Taping applications and adhesion severity.
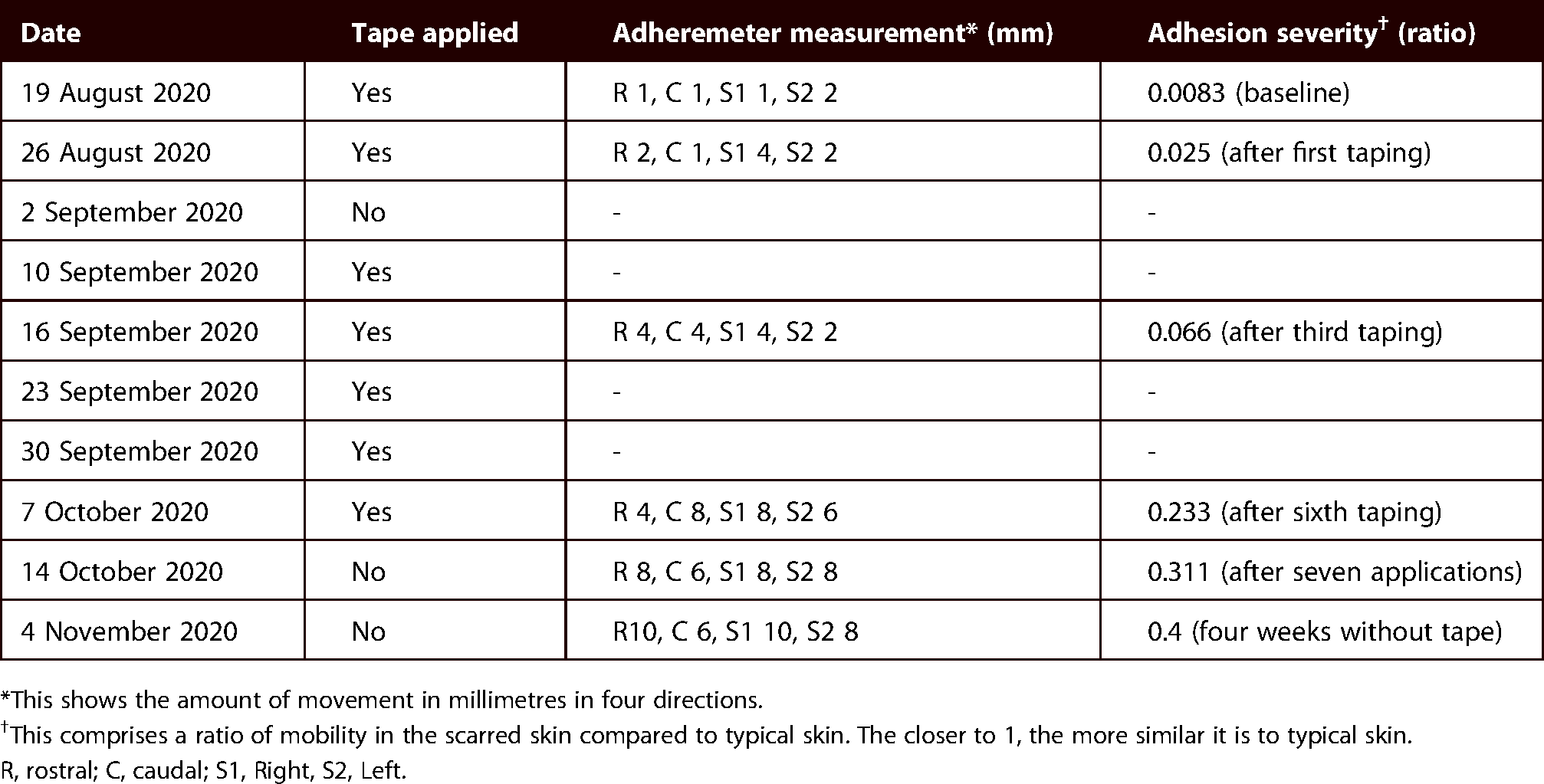
*This shows the amount of movement in millimetres in four directions.
This comprises a ratio of mobility in the scarred skin compared to typical skin. The closer to 1, the more similar it is to typical skin.
R, rostral; C, caudal; S1, Right, S2, Left.
Appearance and motor skill scores.

AIMS, Alberta Infant Motor Scale; PDMS-2, Peabody Developmental Motor Scale second edition; POSAS, Patient and Observer Scar Assessment Scale.
Comprehensive assessments were subsequently conducted after the sixth taping; however, AS was calculated after the final or seventh application. After a four-week washout, the last AS score showed continued improvement, evidenced in a change from 0.233 to 0.311 (Table 1). This was done to see if regression occurred when the tape applications stopped.
Discussion
The incidence of neurodevelopmental impairments in infants with CHD is in the range of 20%–60%.5,6,46,47 Common deficits occur in cognition, social-emotional interaction, attention and sensory-motor function.5,6,46,47 As scar adhesion could impair acquisition of motor skills, pediatric rehabilitation should assess scar tissue after surgical intervention.
Change in affect
The infant's overall distress changed soon after initiating PT, evidenced by a decreased FLACC score. The caregiver reported reduced fussiness, especially with tummy time, and less fisting of the right hand. This could be due to parent education on the safety of tummy time, increased prone tolerance and the distal glide created by the direction of the tape application. 33 Increased mobility could also account for less stress. The FLACC score did not increase with the taping application, implying that it does not create discomfort. CHF is a precaution for using KT; however, surgery had addressed the underlying pathophysiology. There were no adverse side effects to this treatment. On one occasion, the tape was left on between treatments. The PT removed it, and vasodilation was noted, which is common and non-harmful. KT was not applied that week. Ultimately, low tension applications should be used in infants to avoid skin hypersensitivity. Many elastic tape lines carry products created for fragile skin, such as Kinesio Light Touch, Monkey Tape and PerformTex Pediatric Tape, and should be considered.
Study limitations
This is the first case report investigating KT's effects on an infant's sternotomy scar adherence in the presence of standard PT. Although correlation does not equal causation, the AS, AIMS, POSAS and FLACC scores improved with six tapings over seven weeks. The treatment was initiated 12 weeks after surgery and may be more effective if administered earlier in the remodelling phase; however, one study showed positive outcomes with older, more extensive scars. 48 Typically, the earlier the issue is addressed, the better the results. 49 Limitations include the retrospective nature, the same therapist performing the assessments and the potential bias of the evaluations. There was also inconsistent data collection, the competing nature of the combined treatments and the developmental process. No control is provided for comparison. Lastly, it should be noted that there was a lack of standardised positioning for the images taken and a varying amount of light exposure. The results of this study cannot be generalised to broader populations as this is a single case report; however, it is important as it is the first study using KT as an intervention tool for scar tissue after open-heart surgery.
Conclusion
Infants with CHD are at high risk for developmental delay; thus, attention should be given to the postoperative scar tissue and its potential impact on motor learning. While more research is needed to analyse the specific effects, Kinesio tape may provide a safe adjunct to treat scar tissue.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
How to cite this article
G Harvey E. Kinesio taping to address post-sternotomy scars in pediatric patients: A case report. Scars, Burns & Healing, Volume 7, 2022. DOI: 10.1177/20595131211067380.