
Abstract
Background:
Rates of self-harm injuries are considered to be increasing. The attitudes of healthcare staff towards patients who self-harm may be negative and a small amount of research specifically investigating burns and plastic surgery healthcare professionals has recently been conducted exploring this issue. This study aimed to determine attitudes towards and adherence to national guidance by healthcare professionals in a UK burns and plastic surgery department with respect to patients who self-harm.
Method:
An audit questionnaire, completed in a designated Burns Unit and plastic surgery department, within a UK hospital with a major trauma centre.
Results:
Data were obtained from 59 healthcare professionals. The majority of responders held positive attitudes towards those who had self-harmed. However, a significant minority held negative attitudes, stating that they found it difficult to be compassionate (10%; n = 6) and believing that patients usually self-harm to get attention (9%; n = 5). One-fifth (n = 12) agreed that, on a departmental level, conservative management (as opposed to surgery) was offered more frequently for self-harm injuries compared with accidental injuries, contrary to national guidance. Awareness of national guidance in relation to self-harm injuries was markedly lacking, in only 12% (n = 7/59) and the frequency of completing relevant training was low (34%, n = 20/59).
Conclusion:
Education among healthcare professionals is important, to ensure adherence to best practice. The findings of this study strongly suggest that many healthcare professionals do not know the current best practice. As a result, these highly vulnerable patients may be receiving sub-optimal care, with consequentially poor outcomes.
Lay Summary
A small but significant number of injuries managed by NHS burns and plastic surgery departments are a result of self-harm. There are national guidelines published by the National Institute of Healthcare and Excellence which are designed to assist healthcare professionals with the care of patients who have self-harmed. The aim of this audit was to explore the attitudes of staff working within a UK burns and plastic surgery department and whether current practice adheres to the national guidance. Staff, including surgeons, nurses and allied health professionals, were surveyed using a questionnaire. Results suggested from a questionnaire found that the majority of healthcare professionals have a positive attitude towards patients who self-harm. However, a significant minority held negative attitudes and conservative management is offered more frequently as opposed to surgery. The majority of staff were unaware of the national guidance and would like further training on the topic of self-harm. Further education on self-harm for healthcare professionals working in burns and plastic surgery departments is required and dissemination of awareness of the national guidance is key.
Introduction
In the UK, self-harm has reported prevalence rates of 4.6–6.6% in the general population 1 and this may be increasing. 2 Patients who self-harm may be subjected to stigmatisation within the healthcare system, as healthcare professionals’ attitudes towards patients who have self-harmed are known be more negative than those with regard to patients with other medical conditions.3,4 Negative professional attitudes may influence patients’ treatment. Punitive care, including judgmental comments and withholding of treatment5,6 have been reported. In plastic surgical and burns departments, clinical decisions concerning operative or conservative management may be influenced by negative attitudes or distorted beliefs about self-harm but published research on this topic is limited. Patients who have self-harmed may evoke strong emotional reactions among healthcare professionals, with perceptions that patients who self-harm are difficult to manage or may be carrying out ‘attention-seeking’ behaviours.7–9
The UK National Institute for Health and Care Excellence (NICE) provides practice guidelines, 5 generic to all types of self-harm. These state that physical treatments for self-harm injuries should be the same as those for injuries not caused by self-harm. It also recommends that treatment for the physical aspects of self-harm injuries should not be dependent upon patients’ willingness to accept psychosocial or psychiatric assessment and treatment. Moreover, in patients who repeatedly self-harm, this guidance suggests that each individual episode should be treated independently and that patients should be fully informed and involved in decision-making. Healthcare professionals who work with patients who self-harm are recommended to receive training and be aware of the relative increased suicidal risk of elderly self-harming patients.
Published evidence on professional attitudes regarding patients who self-harm, management of self-inflicted injuries which are managed medically, surgical decision-making processes and adherence to NICE guidance is very limited. One investigation involved an audit of 63 burns and plastic surgery multidisciplinary staff members, using a brief, eight-item questionnaire. 10 This suggested that psychiatry and psychology services were deemed most appropriate for patients who have self-harmed and that only 22% of staff members considered surgery as being appropriate. However, 71% believed that patients who have self-harmed should be offered surgery as often as required, irrespective of age, length of experience or whether the healthcare professionals were medically qualified. Some healthcare professionals commented that surgery should only be offered to save life and 9% of medically qualified professionals reported that patients should only be offered surgery once. No surgeons believed that patients should be offered surgery twice or three times, possibly suggesting ‘all or nothing’ thinking styles across the surgeon group. The authors also suggested that surgeons, in particular, may feel more uncomfortable and less motivated to help patients who self-harm than do other professional groups.
Rai et al. assessed attitudes, beliefs and surgical decisions in self-harm injuries using a mixed-methods survey of 37 UK burns surgeons with an electronic questionnaire (paper under review). This questionnaire also contained two hypothetical case scenarios. Quantitative and qualitative data suggested that most burns surgeons held compassionate, non-judgmental attitudes. However, 11% held negative views about patients who self-harm; 19% were less likely to offer surgical interventions and 24% believed that surgery should only be offered a limited number of times in this group. Beliefs that surgery reinforces future self-harm, that self-harm is ‘attention-seeking’ and concerns about wound tampering were evident. Burns surgeons with more experience were less judgmental, offered surgical interventions more often and were less likely to hold negative beliefs about patients who self-harm. The authors concluded that education in management of self-harm is required for burns surgeons, particularly during the early period of surgical training.
The aim of this audit was to determine the attitudes of healthcare professionals in a designated UK Burns Unit and Plastic Surgery Department, with respect to self-harm injuries and to consider whether behaviour and treatment planning was concordant with national guidance.
Methods
Design
Data were collected between October and December 2016. The study involved data gathered using a questionnaire that had been developed to measure burns and plastic surgery healthcare professionals’ attitudes and adherence to the NICE guidance. 5 The study was classed as an audit and informed consent was gained before participation.
Participants and setting
Healthcare professionals working within an adult and paediatric burns and plastic surgery department in a large UK NHS Hospital Trust were invited to participate. Participants completed the questionnaire either in paper format or online, via a link distributed by hospital email (‘SurveyMonkey®’).
Measures
A questionnaire was developed by the authors, specifically to address the aim of the study. The questionnaire took approximately 10 min to complete and contained 31 items. Ten items captured demographic and professional information, length of service in the affiliated department and information about: exposure to patients who self-harm; training received; and awareness of the NICE guidance. 5 The remaining 21 items contained Likert-scale responses, prompting participants to state their level of agreement, in order to measure attitudes and adherence to NICE guidance. 5
Data analysis
Descriptive analysis of responses was carried out. In addition, non-parametric (Mann–Whitney U) analysis of differences in responses between participant sub-groups was carried out, using SPSS Premium (IBM Predictive Software, version 23).
Results
Participants’ demographics
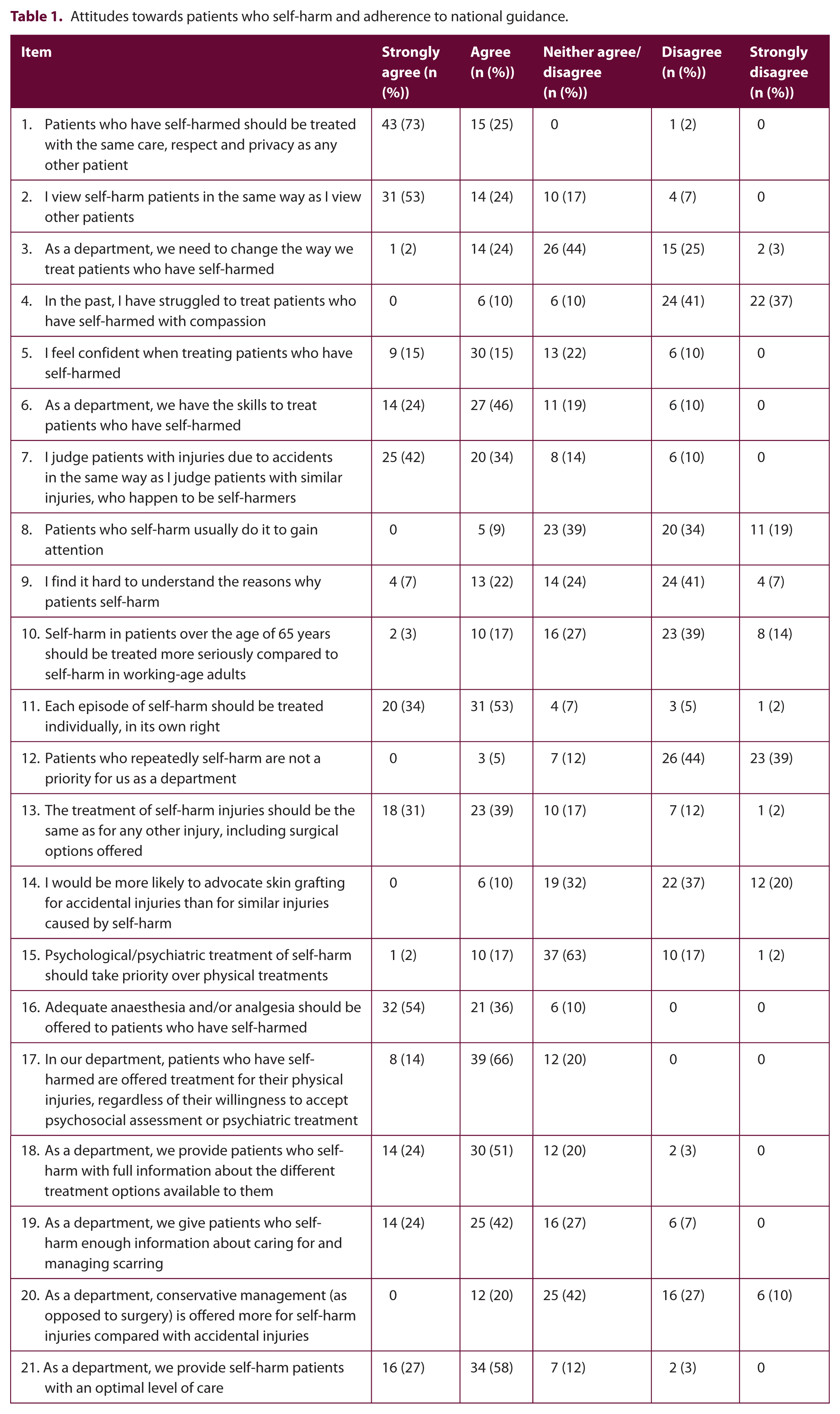
All 59 questionnaires that were accepted were filled satisfactorily. Consolidated data for the entire questionnaire are shown in Table 1.
Attitudes towards patients who self-harm and adherence to national guidance.
Participants showed a female preponderance (71%, n = 42 female; 27%, n = 16 male). One participant did not state their gender. Participants’ age ranges, in order of frequency, were: 30–39 years (32%, n = 19); 18–29 years (29%, n = 17); 40–49 years (25%, n = 15); 50–59 years (9%, n = 5); and 60–69 years (3%, n = 2). One participant did not state their age. Most participants were either doctors (36%, n = 21) or nurses (34%, n = 20). Other occupations included healthcare assistants (10%, n = 6), physiotherapists (9%, n = 5), occupational therapists (5%, n = 3) and one dietician. Two reported being of an ‘Other’ professional background and one participant did not state their profession.
Participants’ plastic surgery and burn care experience varied. One-third (n = 20) had more than ten years of experience; 31% (n = 18) had less than one year of experience; 14% (n = 8) had 2–5 years of experience; 12% (n = 7) had 1–2 years of experience; and 9% (n = 5) had 5–10 years of experience. One participant did not disclose their work experience.
Exposure and training requirements
Over one-third (n = 21) of participants reported contact with patients who have self-harmed a few times per month; approximately one-third (n = 19) reported a few times per year; 17% (n = 10) reported once per month; 12% (n = 7) reported once a week; one participant reported daily contact; and one participant did not state frequency of contact. When asked if they had received any training in relation to self-harm in the past, one-third (n = 20) reported ‘Yes’ but two-thirds (n = 39) reported ‘No’. When asked if they thought they needed any further training in relation to self-harm, approximately three-quarters (n = 45) reported ‘Yes’ and approximately one-quarter (n = 14) reported ‘No’.
Attitudes towards patients who self-harm and adherence to national guidance
Participants were asked if they were aware of the UK NICE guideline ‘Self-harm in over 8s: short-term management and prevention of recurrence’. 5 Twelve percent (n = 7) reported awareness of this guideline. Eighty-one percent (n = 48) were not aware. Seven percent (n = 4) were unsure. When asked if they had read the NICE guideline, 5% (n = 3) reported that they had. Ninety percent (n = 53) reported not having read the guideline and 5% (n = 3) were unsure. Responses generally suggested non-judgmental and compassionate attitudes towards patients who self-harm. However, approximately one-quarter (26%, n = 15) of participants believed that the department needed to change the way it treats patients who have self-harmed. A significant minority admitted: struggling to treat patients with compassion in the past (10%, n = 6); not feeling confident when treating patients (10%, n = 6); and judging patients who self-harm differently (7%, n = 4).
Nine percent (n = 5) believed that patients who self-harm usually do it to gain attention and a further 39% (n = 23) neither agreed nor disagreed with this. Over one-quarter (n = 17) agreed that they found it difficult to understand why patients would self-harm and 14% (n = 8) did not agree that treatment for self-harm injuries should be the same as for accidental injuries, with a further 17% (n = 10) neither agreeing nor disagreeing with this. One-fifth (n = 12) agreed that, on a departmental level, conservative management (as opposed to surgery) was offered more frequently for self-harm injuries compared with accidental injuries. Knowledge that self-harm in patients aged over 65 years should be treated more seriously compared to working-age adults was lacking in a significant number of participants (53%, n = 31 disagreed; 20%, n = 12 agreed).
The results of Mann–Whitney U test analysis suggested that nurses more strongly believed that ‘Patients who have self-harmed should be treated with the same care, respect and privacy as any other patient’ (U = 151, P < 0.05, two-tailed) than did doctors/surgeons. Healthcare professionals with less than one year of burn care and plastic surgery experience, agreed less strongly with the item ‘I feel confident when treating patients who have self-harmed’ than did those with ten or more years of experience (U = 114.5, P < 0.05, two-tailed). No other statistically significant differences between participants’ sub-groups were identified.
Discussion
This investigation of healthcare professionals’ attitudes towards patients who self-harm and the clinical decision-making processes in relation to their treatment identified some reassuring findings, but also several features that should be of concern.
The frequency of awareness of the NICE guidance on management of self-harm 5 was very low. Perhaps, as a result, the frequency of completed specific training was also low. Also, knowledge of the seriousness of self-harm in patients aged over 65 years due to the relatively increased suicidal risk, highlighted in the NICE guideline, 5 was also conspicuously lacking among the majority of healthcare professionals. The authors regard these findings as strongly indicative of a need for better dissemination of best practice guidelines and updates from NICE, since it is necessary to know of a guideline’s existence, before one may gain the training to fulfil the guideline’s requirements. Educational courses also need to take responsibility for dissemination. This need is all the more pressing, given apparent increases in frequency of self-harm. 2 The large proportion of staff members who felt that they required further training in this subject may be a reassuring indicator of the motivation for this training. It may also highlight the challenges that patients who self-harm can pose to healthcare professionals and burns and plastic surgery services. Provision of high-quality courses, with adequate dissemination, advance notice and ease of uptake for staff are therefore of high priority.
While it is encouraging that a large majority of healthcare professionals displayed positive attitudes and compassion for patients who self-harm, in concordance with national guidance, a significant minority of responders reported difficulty in treating these patients with compassion and in understanding why a patient may have self-harmed.
It is particularly concerning that patients who self-harm may be offered conservative management rather than surgery, more often than patients with similar, but accidental injuries. One in ten healthcare professionals explicitly reported that they advocated skin grafts less often to those with self-harm injuries. This is inconsistent with NICE guidelines which state that patients should be offered the same treatment irrespective of the cause. 5 It was not an aim of this study to determine whether professional attitudes had a causal link with modes of treatment. However, one cannot fail to acknowledge with concern, a concordance between frequencies of exceptional attitudes and frequencies of non-standard treatment options.
The findings from this study are largely consistent with previous studies which have suggested that most burns and plastic surgery healthcare professionals hold positive attitudes towards patients who self-harm, but that some find this challenging. 10
Difficulties with understanding, empathising and compassion may be regarded as lesser priorities in specialties whose prime focus is physical reconstruction.8,11,12 Whether intentional or otherwise, if negative perceptions lead to inequitable treatment provision, this may prove disastrous for patients. Individuals may react with disillusionment and avoidance of medical help, due to fear of prejudice and negativity.11–13
Patients, primary and emergency care providers seek specialist help in the hope of receiving expert assessment and treatment, in order to obtain the best outcomes. While specialist units may regard themselves as having expertise in relation to self-harm injuries, it may be that the level of a unit’s expertise would best be expressed in terms of its outcomes, rather than more simplistic measures. 14 The extent to which a unit adheres to current best practice, as set out by NICE guidelines in the UK, could be regarded as a first step in defining the aspects of a unit’s expertise, with regard to management of self-harm injuries.
This study is limited in that it may not represent other burns and plastic surgery units within and outside the UK. In addition, due to the nature of the topic it is possible that some respondents may have answered in a socially desirable way, for example, by selecting the more neutral ‘neither agree/disagree’ option on some items. Respondents may not have wanted to appear negative towards this patient group, even if this was the case.
Through education, healthcare professionals may gain better understanding of what functions self-harming behaviour may serve for individuals. Continued re-education and reinforcement of these ideas would be required. This study raises important issues surrounding the need for: education in self-harm; awareness of national guidance for clinical departments; and action to integrate this knowledge and awareness into efforts to achieve improved outcomes for patients with self-harm burn injuries. This investigation was carried out in an adult burns unit. Further research should focus upon richer analyses of attitudes, possibly through qualitative studies, surgical decision-making and treatment outcomes. These investigations should be extended to include children who have self-harmed in order to understand better the subtleties and complexities of care requirements in these exceptionally vulnerable groups.
Conclusion
The majority of healthcare professionals working in burns and plastic surgery departments hold positive attitudes towards those who have self-harmed. However, a significant minority hold negative or ambivalent attitudes. Patients may be offered surgical treatments less frequently than patients who have sustained injuries accidentally. Awareness of national guidance in acute management of self-harm is lacking. There is a need for education for healthcare professionals working in burns and plastic surgery departments so that national guidance can be appreciated and followed, to ensure that best practice is delivered to all patients in this highly vulnerable group.
Footnotes
Authors’ note
Ciaran O’Boyle is a member of the editorial board of the journal Scars, Burns and Healing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The article processing charge for this paper has been kindly paid by the Katie Piper Foundation.