
Abstract
Objectives
The purpose of this study was to describe the severity of the radiographic findings of COVID-19 over time and to assess their correlation with the duration of symptoms prior to admission, CT scores, and disease severity.
Methods
A retrospective analysis of patients with COVID-19 confirmed by reverse transcription polymerase chain reaction (RT-PCR) and CXR who were admitted at the university hospital was performed between March 25 and 30 April 2020. Baseline and serial CXRs were reviewed, along with onset and disease time courses. Correlations between CXR scores and CT scores, durations of symptoms and disease severity were evaluated; and also between regression times and disease severity.
Results
Of 208 total patients, there were 33 mild (15.9%), 103 moderate (49.5%), and 72 severe-critical (34.6%) cases. The most frequent symptoms were fever, cough, fatigue, and dyspnea. Dyspnea was more frequent in patients with severe and critical disease (p < 0.001). The duration of symptoms experienced prior to admission was longer in patients with severe and critical disease than in moderate cases (p < 0.05). Abnormalities on CXR were present on admission in 83.2% patients, with reticulations being the most common finding. CXR scores correlated with duration of symptoms prior to admission and CT scores (p < 0.05 and p < 0.001, respectively). The median radiographic score of the severe-critical-type group was significantly higher than the moderate type (p < 0.001) and regression time correlated with disease severity (p < 0.001).
Conclusion
Our study showed that despite the limitations, CXR remains a very important tool for diagnosing and managing patients with COVID-19.
Introduction
Coronavirus disease 2019 (COVID-19), caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in Wuhan, China in December 2019. 1 Recently, there has been an increasing number of publications assessing the validity of chest computed tomography (CT) and chest X-ray (CXR) for COVID-19 patients. Most published studies have confirmed the superiority of CT over CXR for detection of COVID-19.2–6 However, in some hospitals, including our own, clinicians rely on radiographs, both for diagnosis and for clinical management of these patients. Although CXR shows low sensitivity in detecting positive COVID-19 cases in the early phase of the disease, initial CXR is useful in the diagnosis of moderate and severe disease. 4 Some studies have also shown its utility for predicting clinical outcomes of COVID-19 patients. 7 Although CT is a more sensitive modality than CXR for detection of COVID-19, several other factors, such as local resources, image interpretation expertise, and different attributes of CXR and CT influence the final decision on which imaging modality should be used for management of COVID-19 patients. 8
This study aimed to describe the severity of the CXR findings in COVID-19 patients and to assess correlations between these findings with the duration of symptoms experienced prior to admission, CT scores, and disease severity.
Methods
Patients
This is retrospective, single center study conducted on 208 patients admitted for the SARS-CoV-2 infections to the tertiary hospital for treatment from 25th March to 30th April 2020. COVID-19 infection was confirmed by reverse transcription polymerase chain reaction (RT-PCR) analysis of nasopharyngeal swabs and throat swabs. Patients admitted to our hospital with a clinical symptoms consistent with COVID-19 and RT-PCR positive with mild symptoms were included in the study. At the beginning of endemic, asymptomatic close contacts of a positive case were also tested. In this phase, the Ministry of health of Republic of Serbia issued hospitalization for all tested positive patients regardless of disease severity. Discharge of these patients was after two consecutive RT-PCR negative tests. Epidemiological and clinical data, such as symptoms experienced and past medical history, were obtained, in most cases, through the electronic patient database and, in a few cases, directly from the patient. Clinical data were doubly-entered by two physicians and the final data were obtained by consensus when there was a discrepancy. The following epidemiological and clinical data were collected: age, sex, clinical symptoms (fever, cough, myalgia, fatigue, dyspnea, headache, diarrhea, and loss of appetite, smell, and taste), presence of comorbidities (diabetes, hypertension, cardiovascular disease, chronic obstructive pulmonary disease, malignancy), and survival status. Patients were divided into three age groups: 20–44, 45–59, and ≥60 years. Durations from the onset of symptoms to the time of admission, CXR, and CT examinations and outcome (recovery or death) were determined for all patients. The severity of the disease was classified as one of four categories according to the Guidelines for the Diagnosis and Treatment of New Coronavirus Pneumonia. 9 Patient selection for this study was consecutive and no exclusion criteria were applied.
Image acquisition and analysis
All patients had CXRs upon admission, with follow-up CXRs available for all but 31 patients (who had normal CXRs at admission and did not experience any disease progression). CXRs at admission and follow-up were acquired in the posteroanterior (PA) or anteroposterior (AP) projection depending on each patient’s condition. CXRs of patients in the intensive care unit were acquired in the AP projection using portable X-ray units. Most of the CXRs at presentation were performed in the PA projection. Radiographic features including reticulations, consolidation, ground glass opacities (GGO), and pulmonary nodules were diagnosed according to the Fleischner Society glossary of terms. 10 The presence of pleural effusion was also noted. The distribution of the lung pathological findings was categorized as: (a) right, left, or bilateral lung involvement, (b) perihilar predominance or peripheral predominance, (c) upper zone, lower zone (defined as upper/lower halves) or no zonal predominance. To quantify the extent of infection, a severity score was calculated using a method reported in the literature. 4 A score of 0–4 was assigned to each lung depending on the extent of involvement of pathological findings (0 = no involvement; 1 = <25%; 2 = 25–50%; 3 = 50–75%; 4 = >75% involvement). The scores for each lung were summated to generate the final severity score for each patient.
Chest CT scans were performed using multi-detector CT scanners (Siemens Somatom Definition AS+, Erlangen, Germany). CT images were collected during a single breath-hold without intravenous contrast infusion. Overall scan time was 2 s, and slice thickness for reconstruction was 1 mm. For each of the patients, the major CT features were described, including the pattern and distribution of the lesions and the number of involved lobes. The patterns on the CT images were evaluated and a semi-quantitative scoring system was used to estimate the area of involvement for each lung lobe based on a method published previously. 11 There were five lung lobes assessed per patient; the range of possible scores was from 0 to 20. All available CXR and CT images of the patients were obtained and reviewed by one thoracic radiologist (25 years of experience) and a general radiologist (5 years of experience). Patients with follow-up CXRs or CT images were compared to determine if there was progression, stability, or improvement of the affected portions of the lungs. Correlations among CXR and CT scores and durations of symptoms, disease severity, and regression times were evaluated. The outcomes were recovery and death.
Statistical analysis
Statistical analysis was performed with IBM Statistical Package for the Social Sciences (SPSS) software (Build 1.0.0.1347; IBM, New York, USA). The baseline characteristics of the subjects that were continuous variables were compared using Student’s t-tests. Categorical variables were compared using the chi-square test. Spearman’s correlation analyses were performed to assess correlations between variables. Mann–Whitney U test was used for independent group comparisons when parametric test assumptions could not be met. Statistical significance was defined as p < 0.05 for all tests.
Results
Demographic characteristics of patients.

Clinical data
Relationship between diseases severity and symptoms.

Mann–Whitney U test determines relation between disease severity and duration of symptoms prior to admission, baseline CXR scores and time of regression.

The time of evolution of symptoms in the group of patients who died was 8.2 days which is significantly shorter in comparison to 19.4 days of survivors (p < 0.05).
Distribution of disease severity by age.

Comorbidities were more common in severe and critical cases with domination of cardiovascular diseases and hypertension (Table 1). Coexisting medical conditions were recorded in 78% of patients with the worst outcome and in 49% of survivors.
Radiological data
Abnormalities on CXRs were present on admission in 173 patients (83.2%). Forty-nine (28.3%) of those patients had abnormal CXR without respiratory symptoms but with other symptoms (fever, fatigue, and myalgia). The most common findings on CXR were reticulations, followed by GGOs and combinations of consolidations, GGOs, and reticulations (Figure 1). Chest X-ray (CXR) features of patients with COVID-19 based on disease severity. (GGO: ground glass opacities).
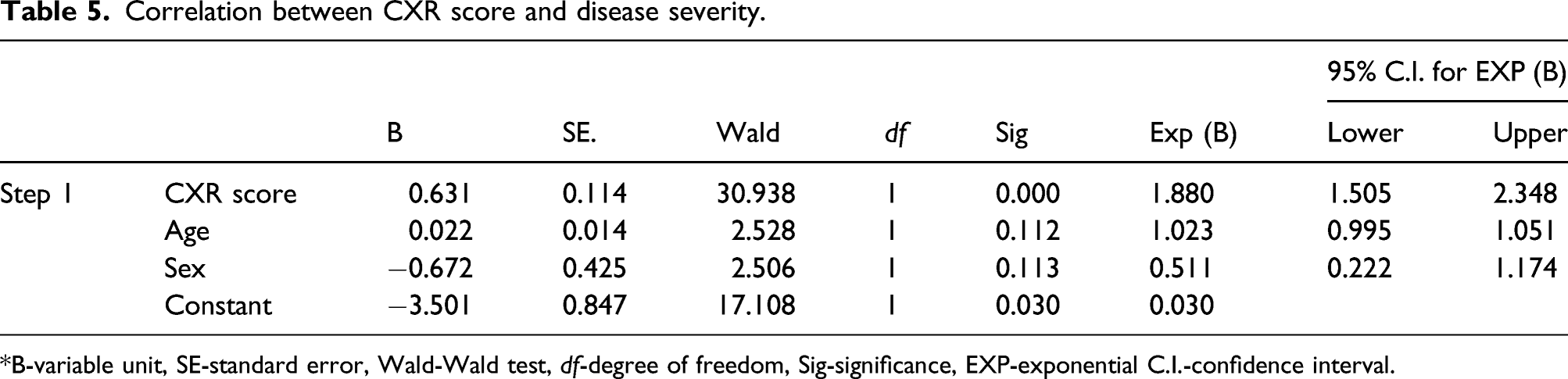
Most patients had bilateral pathological findings, with peripheral localizations predominantly in the lower lung fields (Figures 2(a)–(c)). In patients with moderate disease severity, the average radiographic score was 2.3. The CXR scores were significantly higher in patients with severe and critical diseases, averaging 4.1 and 4.5, respectively (p < 0.001). A one point increase in the CXR score was associated with nearly double the likelihood of a severe or critical disease (odds ratio (OR): 1.88; 95% confidence interval (CI) 1.50–2.35) (Table 5). (a) Chest radiographs of COVID-19-positive patients at the time of admission. Reticular opacities in the lower lung fields (arrows), with a total score=2. (b) Hazy opacities in the right upper lung field (arrows), with a total score=2. (c) Patchy opacities in peripheral lung zones (arrows), with a total score=5. Correlation between CXR score and disease severity. *B-variable unit, SE-standard error, Wald-Wald test, df-degree of freedom, Sig-significance, EXP-exponential C.I.-confidence interval.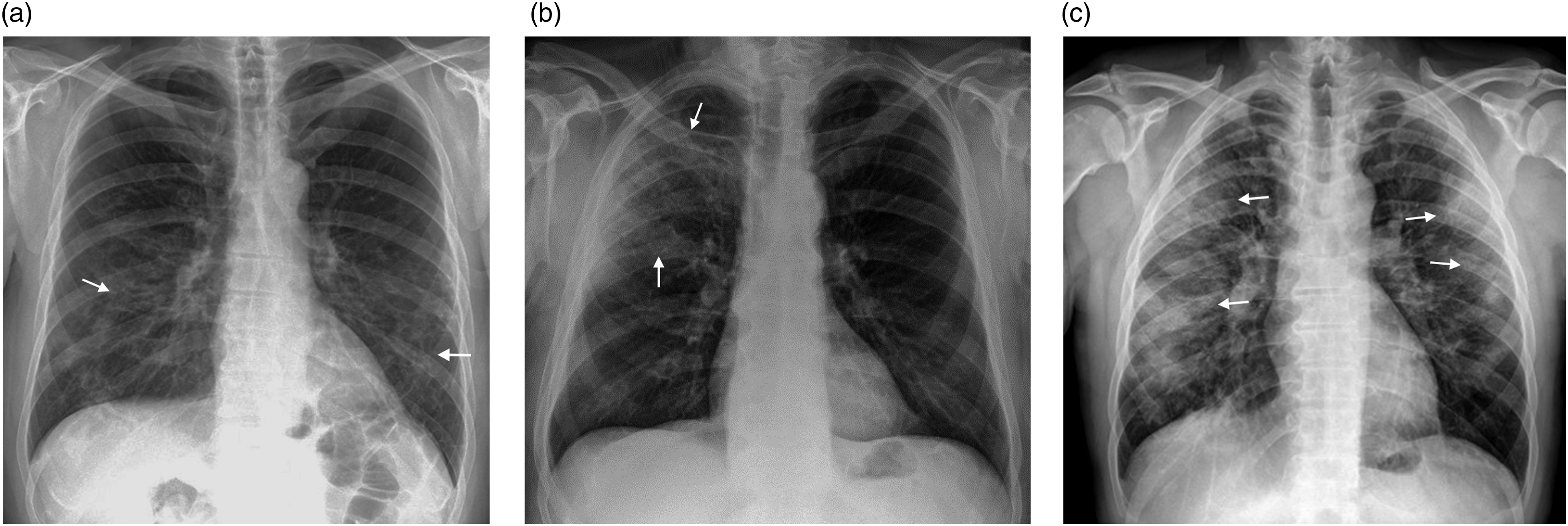
Survived patients had lower CXR score than those with worst outcome (3.04 vs 4.5). CXR scores correlated with the duration of symptoms experienced prior to admission (p < 0.05). Eighty-four patients underwent chest CT 1 to 6 weeks from symptom onset. CT was performed in eight patients with normal CXR who experienced appearance of respiratory symptoms and the decrease in blood oxygen saturation. In other 76 patients, clinical deterioration or poor response to treatment was indication for chest CT. A summary of CT findings over the 6-week period is shown in Figure 3. Computed tomography (CT) features observed in COVID-19 patients across the 6-week assessment period.
The most common CT findings 1 week from onset of the disease were peripheral GGOs, as well as GGOs with segmental consolidations, with the total CT score being 7.8±4.5 (Figure 4(a)). In the second week, the predominant findings were extensive GGOs, as well as a mixture of GGOs and consolidations and reticulations, including “crazy-paving” patterns in 25% of cases, with the total CT score being 7.6±4.2. The most frequent findings at the third-week follow-up were reticulations and GGOs with linear fibrous changes, followed by consolidations and GGOs. “Crazy-paving” patterns were detected in 23.8% of cases, with the total CT score being 10±6.2 (Figure 4(b)). At the 4-week follow-up and later, reticulations and GGOs were the predominant finding, and subpleural bands with long curved lines posteriorly were evident in one third of patients who underwent CT scans at that time; the CT score was 15.9±3.2. Inverse halo signs were detected in five patients (Figure 4(c)). In most patients, the observed CT patterns were typical of those with COVID-19 infections. In the 72 patients who underwent CT scans, the CXR scores correlated significantly with CT scores (p < 0.001). In eight other patients with radiographic abnormalities, CT patterns did not correspond to the CXR findings. (a) Chest CT performed 6 days from the onset of symptoms. Irregular GGOs are shown in the peripheral parts of both lungs (arrows). (b) Chest CT performed 13 days from the onset of symptoms. Mixed GGOs are observed, with consolidations in both lungs (arrows). Interlobular septal thickening (crazy-paving pattern) is seen (yellow box)*. (c) Chest CT performed 4 weeks from the onset of symptoms. Small consolidations, slight GGOs, “inverse halo” signs, and fibrous strips are present (arrows).
In four patients with normal chest radiography, CT scans revealed GGOs associated with a low CT score (Figures 5(a) and (b)); The time of regression ranged from 3 to 58 days (19.5±8.4) and correlated with disease severity (p < 0.001). The first sign of regression on radiography appeared 6 days from disease onset in three patients. Clinically and radiographic significant regression was observed in 75% of cases, with an average time of 19.8 days from the onset of the disease. Seventeen patients were not included in the recovery group (three patients were still hospitalized at the cut-off day and 14 patients died). (a) Chest radiographs of a COVID-19-positive patient. Normal finding. (b) CT scan of the same patient. Scattered small ground glass opacities in the peripheral parts of both lungs (arrows).
Discussion
Clinical characteristics
In this study, we analyzed the association of radiological findings’ extension with duration of symptoms experienced prior to admission, disease severity and outcome in patients hospitalized in our clinical center. The association of clinical symptoms’ evolution with disease severity and outcome was also analyzed. Patient demographics in terms of age and sex were similar to those of other published studies.4,12,13 The most common symptom was fever, followed by cough, fatigue, myalgia, and dyspnea. Other symptoms such as diarrhea and loss of smell and taste were present in a small number of patients. Clinical symptoms also matched other reported data.14–18 The only symptom more frequent in patients with severe and critical disease was dyspnea. It was expected, as all of them had extensive pneumonia. 19
Results of this study show longer time of symptoms evolution in patients with severe and critical disease than in moderate and mild disease which is consistent with data reported in previous studies with a similar sample size.17,18 This can be explained by smaller sample in our study and the fact that analysis included patients with mild disease. On the other hand, in our sample, the time of evolution of symptoms was shorter in the group of patients who died in comparison to the survivors which is in line with previously reported data.19–21 Molinaro et al. in their study suggested that less aggressive disease can be the reason for a prolonged presentation in survivors. 19 Comorbidities were more frequent in patients with worst outcome than in survived but the sample is small for valuable conclusion.20,21 One of limitations of this study is possible information bias because hospitalization data were obtained, in most cases, through the electronic patient database which can lead to the underestimation of prevalence of comorbidities.
Only 15.8% of hospitalized patients had mild disease severity, most of whom had symptoms of upper respiratory tract infection without lung involvement.22,23 Nearly one half of our patients had moderate disease severity at the time of admission, and one third of all cases were of severe or critical disease. 6 Patients over 60 years of age suffered from severe and critical disease more frequently than younger patients.19–25
Radiological characteristics
Chest X-rays performed at the time of admission showed pathological findings in the majority of cases and were helpful in the detection of SARS-CoV-2 infections. Abnormal CXR in group of 49 patients without respiratory symptoms at admission additionally confirms that radiography can help clinicians to identify SARS-CoV-2 pneumonia and initiate the treatment on time. CXR scores were used for quantification of lung involvement in COVID-19 positive patients and as prognostic scores for disease severity.4,26 CXR scores in our patients correlated with the duration of symptoms experienced prior to admission. We found significant statistical correlation between CXR scores and disease severity which showed that one point increase in the CXR score was associated with nearly double the likelihood of more severe disease. The course of the disease was monitored clinically, radiographic images were acquired for all patients and CT scans were performed in about 40% of cases, usually those displaying clinical deterioration or poor response to treatment. CT was most often performed in the second and third weeks from the onset of the disease. Imaging manifestations corresponded with the clinical stage in most cases indicating that radiological evolution of COVID-19 pneumonia is consistent with the clinical course of the disease.
Mild disease severity was associated with normal CXR findings in nearly all cases. Our case series, as well as previous experiences, shows that a normal CXR does not rule out disease pathology in the lungs; therefore, clinical monitoring of patients with oximetry is extremely important. 4 The appearance of respiratory symptoms and a decrease in blood oxygen saturation in patients with normal radiography were indications for CT in a small number of our patients. Half of them had pathological findings on CT scans, mostly in the form of discrete GGOs. This finding is in line with the results of previously published studies. 4 Patients with moderate disease severity, in most cases, had bilateral reticular or GGOs; these were most pronounced in the lower lobes with a low radiographic score. The dominant patterns observed on CT scans in these patients were GGOs. In severe and critical cases, the most frequently observed radiographic and CT findings were consolidation and GGOs, which were most extensively localized in the lower lobes; these patients had a significantly higher CT score than those with moderate disease severity.26,27 These findings often led to respiratory failure, which required artificial ventilation in 17 of our patients, similar to findings reported in other studies.28,29 Consolidations in combination with linear opacities and inverse halo opacities were present in the late stage of the disease, confirming that the CT findings correlated with underlying pathophysiology of disease process as it organizes.16,29,30 Considering the patterns and distribution of the opacities, CXR findings correlated significantly with CT findings, but CT was more sensitive for determining disease extent, 4 and semi-quantitative CT scoring could reflect the severity of different stages of this disease. The total CT scores were lowest at the first and second weeks, indicating that, early on, cases were clinically predominantly moderate. The highest scores, which occurred at the later stage of disease progression pointed to severe and critical disease that lasted for a long time, consistent with other studies.22,31,32 Clinically and radiographic significant regression was determined in 3/4 cases at the time of discharge form the hospital. Most patients with incomplete regression had discrete linear opacities, and, in one quarter of such cases, rough scarring remained after extensive consolidations and reticulations. Results of our study show that patients with a lower radiographic and CT scores, those with a shorter time from the onset of the disease to admission, and younger patients recovered faster.15,16 Studies with larger sample size have shown that older patients with comorbidities, shorter time between symptom onset and hospitalization, and with rapid worsening of symptoms are more likely to have the worst outcomes.18–21
Study limitations
The primary limitation of this study was its retrospective nature, which can lead to observer bias. Second, some of the radiographic findings were subtle, which may limit reproducibility in suboptimal viewing conditions or when assessments are performed by non-specialists. Third, there was a lack of a non-COVID-19 control group, and CT scans were available for less than half of patients, thus limiting evaluation of the sensitivity and specificity of CXR. Our study was performed on patients hospitalized in tertiary hospital center which disables the generalization of the results to other cohorts of patients. Our conclusions need to be further verified by large samples and multi-center data.
Conclusion
In conclusion, in our study CXR score has demonstrated to be useful method for quantifying the extent of SARS-CoV-2 pneumonia and as a prognostic factor for disease severity and outcome. The results of this study showed that CXR has the potential to help clinicians in identification and estimation of disease severity in COVID-19 positive patients despite its lower sensitivity compared to chest CT.
Footnotes
Author Contributions
RS and NC designed the study; RS, NC and DM analyzed and organized the results; RS and BM wrote the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia grant number 200110.
Informed consent
Written informed consent was obtained from all subjects before the study.