
Abstract
Acute respiratory infections (ARIs), especially pneumonia, remain the leading cause of childhood mortality and the most common reason for adult hospitalization in low- and middle-income countries, despite advances in preventative and management strategies. This study was conducted to assess factors associated with poor clinical outcome of suspected pneumonia cases among hospitalized patients at the three public health hospitals in Southwest district of Ethiopia. A cross-sectional study was conducted from May to July, 2020. Those patients admitted with suspected pneumonia were followed up during their hospital stay, and data on outcomes were captured by study nurses. Socio-demographics, clinical features, and follow-up data were gathered, and analyzed using SPSS versions 20.0. The differences in patients’ outcome in relation to their clinical features and epidemiologically linked exposures were described and compared using chi-square tests at 95% confident intervals. In this study, 742 patients with suspected pneumonia were analyzed. Of these, 473 (62.8%) of them were male, and 264 (35.6%) were of age 1–4 years. About 533 (71.8%) patients with suspected pneumonia were presented with irregular respiratory signs/symptoms (more than one symptoms) and 132 (17.9%) had underline illnesses. About 633 (85.4%) of patients were improved after treatment, and 109 (14.7%) of them ended with poor clinical outcome after completion of their treatment. Age of the patients and presence of comorbid conditions such as HIV/AIDS infections and bronchial asthma were identified as the risk factors for poor outcome of patients with suspected pneumonia. The clinical outcome of patients with suspected pneumonia at the three hospitals in Southwest district of Ethiopia was not satisfactory. Our findings highlight that in order to reduce poor clinical outcome related to suspected pneumonia, the efforts should be focused on some factors like management and prevention of chronic comorbidities. Increasing clinicians’ awareness on early management of suspected pneumonia cases is also essential in reducing the burden of the disease.
Introduction
Respiratory tract infections are the leading cause of death, especially in the developing world, accounting for approximately three million deaths annually. 1 Especially, pneumonia remains the leading cause of childhood mortality and the most common reason for adult hospitalization in low- and middle-income countries, despite advances in preventative and management strategies. 2 Data from hospital-based studies indicate a 187% increase in hospital admissions due to child pneumonia between 2000 and 2015. 2 Microorganisms like viruses, bacteria, and fungi diseases contribute to the global burden of the disease; still, the novel and emerging viral agents may be responsible as causes of acute respiratory infections that can be outbreaks, epidemics, or pandemics. 3
Although, bacterial conjugate vaccines may have an impact on pneumonia burden, widespread implementation of currently effective preventative and management strategies for pneumonia remains challenging in many low- and middle-income countries. The most common causes of severe bacterial pneumonia are Streptococcus pneumoniae (pneumococcus) and Haemophilus influenzae type b (Hib) contributing to 18% of cases of pneumonia and 33% of deaths. 4 Although bacterial conjugate vaccines may have an impact on the disease burden, widespread implementation of currently effective preventative and management strategies remains challenging in many low- and middle-income countries. For instances, between 2000 and 2015, global hospital admissions for child pneumonia increased by 2.9 times with a more rapid increase observed in the WHO Southeast Asia region than the African region. 5 In 2015, 49% of global pneumonia deaths occurred in India, Nigeria, Pakistan, the Democratic Republic of the Congo, and Ethiopia collectively. 5
The risk factors for pneumonia are multifactorial and include poor socioeconomic status, overcrowding, indoor air pollution and or passive smoke exposure, lack of breastfeeding, severe acute malnutrition, lack of immunization, prematurity, and HIV infection or exposure, and comorbidities such as hypertension, diabetes, and liver diseases could increase the risk of spread and transmission of respiratory tract infections.5–8
In developing countries with about 700 million people, mainly women and children in poor rural areas inhale harmful smoke from burning wood and other fuels, predisposing them to the risk of acute respiratory infections, especially pneumonia. 7 In sub-Saharan Africa, in particular, pneumonia incidence was dominated by effect of human immunodeficiency virus (HIV): up to three-quarters of all hospitalized pneumonia patients are HIV positive. 8 Tuberculosis (TB) also accounts for up to one-quarter of acute pneumonia in high TB incidence settings in Southeast Asia and sub-Saharan Africa.
With the emergency of new coronavirus strain (COVID-19), various non-specific symptoms, including asymptomatic to severe pneumonia, fever, breathing difficulty, lung infections, and death, are the main health problems worldwide.9–11 Starting March 2020, the WHO detected community transmission in some African countries (including Ethiopia) and the risk of spreading is due in large part to deep challenges in practicing social distancing and frequent hand washing in settings of high population density and lack of running water, as well as the non-specific symptoms of COVID-19 that make it difficult to differentiate from endemic illnesses such as bacterial pneumonia, malaria, and influenza.12,13 In addition, close to 40% of children less than 5 years of age in Africa are undernourished, 14 with the highest prevalence of certain underlying conditions, like tuberculosis and HIV/AIDS, with lower ratios of hospital beds and health professionals to its population than other regions, which makes the situation very worst. On the implementations of preventive measures, WHO has implemented several public health measures including rapid identification, diagnosis and management of the cases, identification and follow-up of contacts, infection prevention and control in healthcare settings, implementation of health measures for travelers, awareness rising in the population, and risk communication. 15 We immediately expand surveillance to detect COVID-19 transmission chains by testing all patients with atypical pneumonias, conducting screening in some patients with upper respiratory illnesses and/or recent COVID-19 exposure, and adding testing for the COVID-19 virus to existing surveillance systems is essentials.13,16 However, in countries without advanced laboratory tests, especially in resource-limited countries, knowing the etiologic agent of pneumonia is very difficult. 8
In addition, health authorities should be fulfilling the required information relating epidemiology and clinical features of pneumonia, whether or not it is caused by 2019-nCoV, to design prevention and control strategies in reducing this mortality burden. However, there is currently limited information available related to the epidemiology and clinical characteristics of pneumonia in general. Therefore, the current study was designed to assess the clinical outcomes and risk factors of patients with pneumonia at the three hospitals in Southwest districts of Ethiopia. This sensitizes local institutions and policy makers as it prioritizes the situation in designing strategies for prevention and control, and for updating national as well as local management of patients with pneumonia.
Methodology
Study area and period
A study was conducted from May to July 2020 at three hospitals (Mizan-Tepi University Teaching Hospital, Bonga General Hospital, and Tepi Primary Hospital). These hospitals were found in the Southwest districts of Ethiopia, in Mizan-Aman, Bonga, and Tepi town which are located at 561, 468, and 575 Kms, respectively, from Addis Ababa, capital city of Ethiopia. Currently, these hospitals are providing services for an average of approximately 16,000 inpatient, 95,184 outpatient attendants, 28,508 emergency cases, and 10,080 deliveries in a year coming to the hospitals from the catchment population of 10 million people. An average of nearly 1808 patients with respiratory infection cases per year were admitted at these three hospitals.
Study design and subjects
A cross-sectional study involving the review of patient’s medical records was conducted. Patient’s medical records covering the period of 1 March–30 June 2020 were reviewed. The enrolled patients were followed up and the charts were reviewed daily until the patients were discharged from the hospital. Within the study period, total of 742 complete medical record charts of patients suspected of pneumonia at the three hospitals were reviewed and full demographic and clinical information was extracted during study period. Those patients’ medical records with incomplete information (i.e., without age, sex, and without outcome status) were excluded.
Data collection
At each site, surveillance nurses reviewed registers and emergency logs to identify patients admitted with suspected pneumonia. Suspected pneumonia was defined as evidence of acute infection and ≥1 sign/symptom of respiratory disease. Signs or symptoms of respiratory disease included tachypnea, cough, sputum production, pleuritic chest pain, difficulty breathing, shortness of breath, and sore throat; in addition, for children <2 years old, signs included chest in-drawing, nasal flaring, noisy breathing, and difficulty eating, drinking, or breastfeeding. The trained data collectors (nurses) were enrolled to follow-up patients with suspected pneumonia and to extract the required information from medical chart. Information related to hematologic test results, sign/symptoms of the disease, antibiotics used, and patient’s outcomes were collected. The data abstraction tools were prepared after reviewing different literatures done on related objectives. To increase the quality of data, each patient’s information was independently reviewed by the two data collectors.
Data analysis
The collected data were checked manually for its completeness before data entry. Then, the data were entered daily into Epi-Data version 3.1 and then exported to Statistical Package for Social Science (SPSS) for Window version 20 for analysis. First, frequency distributions and descriptive statistics such as the number, proportion, ward distribution, clinical features, and laboratory test results were identified and calculated. Second, the differences in patients’ outcome in relation to their clinical features and epidemiologically linked exposures were described and compared using chi-square tests at 95% confident intervals.
Operational definitions of the variables
Suspected pneumonia cases are those patients with inflammation of respiratory tracts and with ≥1 sign/symptom of respiratory disease which include cough, fever, difficulty in breathing, fast breathing, and chest in-drawing and/or wheezing.
17
2. Good outcome: If patients with suspected pneumonia are improved after completing the treatment without any complications.
3. Poor outcome: If patients with suspected pneumonia were not improved after completing the treatment, died in hospital or were discharged home in a moribund condition, referred to other health institutions with complications, or refused against medical treatment were classified as poor clinical outcomes.
Results
Demographics of patients with suspected pneumonia
Summary characteristics of pneumonia-suspected cases at the three hospitals in Southwest districts of Ethiopia, 2020.

Clinical features of pneumonia-suspected cases at the three hospitals in Southwest districts of Ethiopia, 2020.

Clinical presentation and outcomes of suspected pneumonia cases
A total of 424 (57.1%) patients with history of dry cough, 304 (41.0%) with fever ≥38°C, 154 (20.8%) with tachypnea/dyspnea (short or fast/laboured breathing), and 115 (15.5%) with X-ray imaging features of pneumonia are presented. Most patients (322 (43.2%)) were treated with crystalline penicillin followed by ceftriaxone (37.5%). From all patients with suspected pneumonia, 633 (85.3%) of them had good clinical outcome after completion of their treatment. On the other hand, 109 (14.7%) patients ended up with poor clinical outcome after completion of their treatment. Of these, 31 (5.5%) of them died or was discharged home in a moribund condition after completion of their treatment, 67 (9.0%) were referred to other health institutions, and 11 (1.5%) refused against medical treatment (Table 2).
Documented laboratory results of suspected pneumonia cases
Documented laboratory test results of pneumonia-suspected cases at the three hospitals in Southwest districts of Ethiopia, 2020.

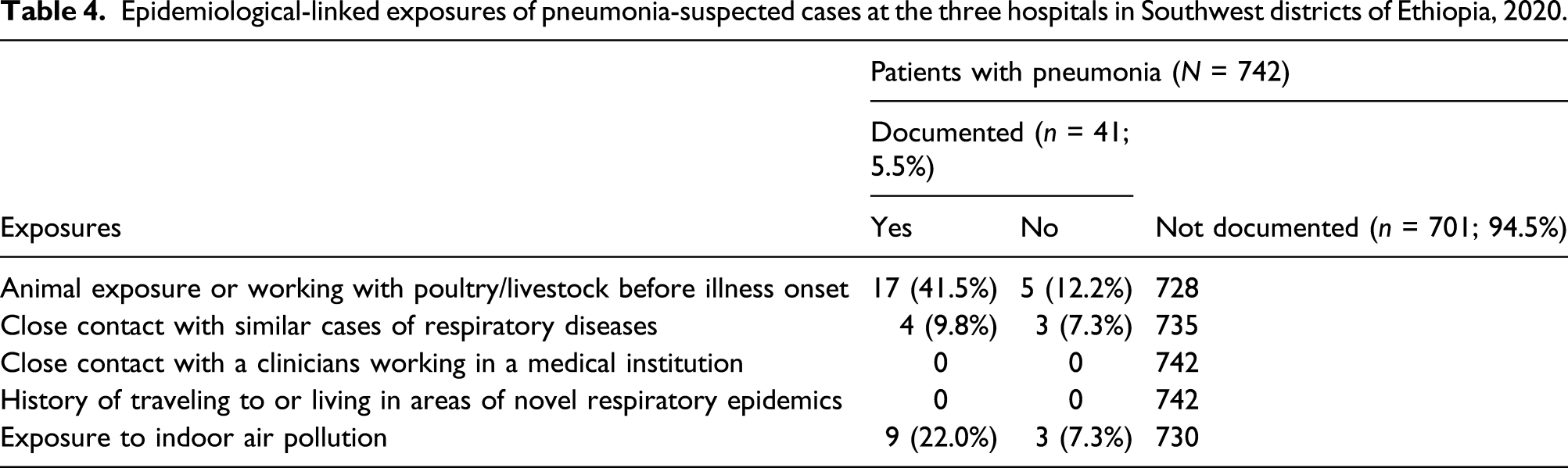
Exposures of suspected pneumonia cases
Epidemiological-linked exposures of pneumonia-suspected cases at the three hospitals in Southwest districts of Ethiopia, 2020.
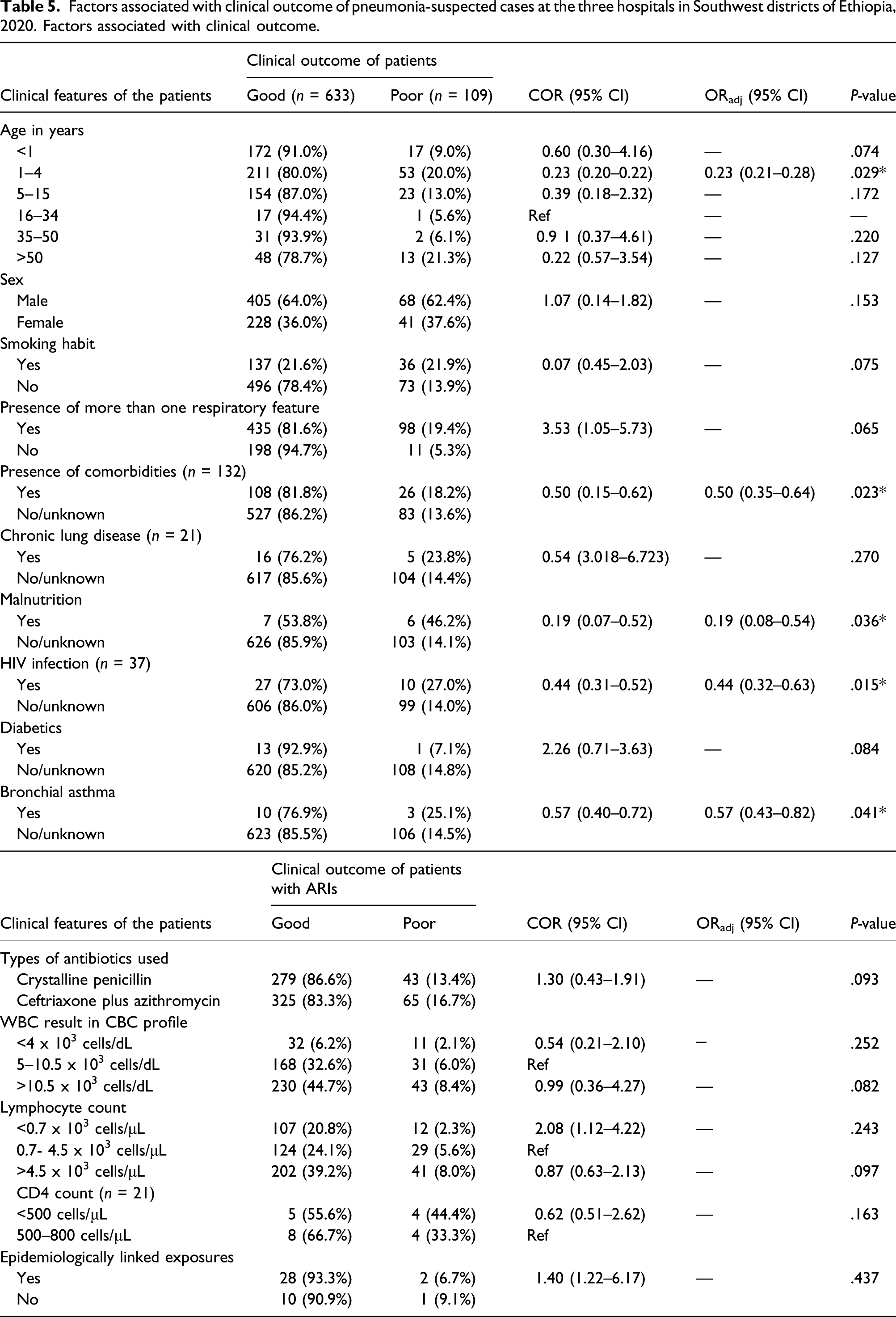
Factors associated with poor clinical outcomes
Factors associated with clinical outcome of pneumonia-suspected cases at the three hospitals in Southwest districts of Ethiopia, 2020. Factors associated with clinical outcome.
Discussion
This study was conducted to assess clinical features, outcomes, and risk factors of patients with pneumonia at the three hospitals in Southwest district of Ethiopia. Accordingly, about 85.3% of patients with suspected pneumonia had good clinical outcome after completions of their treatment. On the other hand, 14.7% of patients ended up with poor clinical outcome after completion of their treatment. That is, 5.5% of them ended up with death after completion of their treatment, 9.0% were referred to other health institutions, and 1.5% refused against medical treatment. This result is comparable with other study finding, in which unfavorable outcomes of patients with pneumonia exceeded 15% in many cases.6,18,19 However, the proportion of good clinical outcome in this study is higher than a finding in Morocco, in which (72.8%) children were classified as having a good prognosis and 187 (27.2%) as having a poor prognosis. 20 The proportion of poor clinical outcome in this study is higher than a finding in India, in which cases of fatality rates related to pneumonia was 1.1%–1.43%,21,22 and in Guatemala, 23 in which 4% of patients <2 years old and 12% of adult patients dying during hospitalization or discharged in a moribund state.
A study across seven low- and middle-income countries showed that a total of death related to severe or very severe pneumonia within 7 days of discharge was 120 (6.7%), with higher finding in Mali (13.4%) and Zambia (26.0%). 24 The study finding in Malawi also showed that pneumonia-related death was 10%. 25 This difference in the proportions of good and poor clinical outcomes of patients with pneumonia may be due to the differences in the progress toward improving care and reducing pneumonia mortality among countries and health facilities and it may differ from time to time. In our situation, there was no continuously functional chest radiography in each hospital due to electric power interruptions and lack of trained human power. That is why most patients are treated with their clinical sign and symptoms.
With regard to age distributions, significant numbers of patients with suspected pneumonia were found to be in the age group of 1–4 years in this study. Our finding is similar with a global and regional meta-analysis finding, in which the incidence, severity, and deaths of childhood pneumonia was highest in Africa and Southeast Asia, 1 of which the five countries India, Nigeria, Pakistan, the Democratic Republic of the Congo, and Ethiopia accounting for 49% of global pneumonia deaths in children younger than 5 years collectively. 2 Thus, strengthening of healthcare delivery system for early detection and treatment and as well as minimization of preventable risk factors can avert a large proportion of death due to pneumonia.
In this study, age of the patients and presence of comorbidities (HIV infections and bronchial asthma) were identified as the independent determinant factors for poor clinical outcome of patients with pneumonia. Those patients with age groups of 1–4 years were 77.0% more likely to end up with poor outcome than patients with reference age groups. The finding of age as a determinant factor for poor clinical outcome of patients with pneumonia in this study is in line with other study findings in different countries.26–32 This may be due to lower immunity in the cases of lower age groups as compared to other age of patients.
In addition, those patients with comorbidity conditions such as HIV and bronchial asthma were 56.0% and 43.0% more likely to end up with poor outcome than patients without history of HIV infection and bronchial asthma, respectively. This result is supported by other study findings, in which pneumonia are the most common cause of infectious disease–related death worldwide associated with age, HIV infection, bronchial asthma, and smoking.26–32 Thus, understanding of these risk factors will help to develop strategies to reduce the burden of mortality from respiratory infections. Thus, to prevent the burden of pneumonia, the efforts should be focused not only on the preventions of suspected pneumonia but also on the other contributing comorbidity factors, such as TB, HIV, and non-communicable diseases.
In this study, although significant numbers of respiratory infectious disease were identified in the medical record, only 41 (5.5%) patients with suspected pneumonia were documented with their epidemiologically linked exposures as predisposing factors. In addition, most (533 (41.8%)) incomplete patient medical records were found in this study. This may be due to poor patients’ history taking and documentation activities of clinicians. Here, beyond improving social determinants that affect lower respiratory tract infections, a combination of public health and clinical strategies is required to control the burden of pneumonia. Thus, this finding suggests that clinicians should practice actively asking of all patients with pneumonia about specific exposure history and developing well patients’ history-taking habits as their parts of routine activities.
This study may have significant contribution to our knowledge in the area of clinical features and outcomes of patients with pneumonia for clinical workers, policy makers, and for other researchers. However, as limitations, we used time period instead of calculating sample size. In addition, this is a hospital-based study, which may miss those who did not visit the hospital for medical care despite they were with suspected pneumonia, so the finding may not be a true reflection of what is in the community. A longitudinal study would better illustrate the effects of the clinical outcomes and potential risk factors than this cross-sectional study.
Conclusion
In conclusion, a clinical outcome of patients with suspected pneumonia was not satisfactory. The determinant factors for poor outcomes were age of the patients and presence of comorbidities, such as HIV/AIDS and bronchial asthma. Therefore, to improve outcome of patients with pneumonia, early detection and management as well as reducing other comorbidities, such as TB, HIV, and other non-communicable diseases, are essential. In addition, improving the functions of clinical care and diagnostic centers as well as expanding short course training of health workers on early detections of sign and symptoms and on proper management of patients with suspected pneumonia will reduce the morbidity and mortality burden.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Mizan- Tepi University Ethical Review committee (Approval Number/ID: Rf/240/2020). District health offices were wrote permission letter to the hospitals where the actual study was done. Head of each hospital were informed about the study and asked to provide permission to conduct the study.
Informed consent
Written informed consent was obtained from the study participants before the study.