
Abstract
We developed and assessed whether a novel neutrophil-to-hemoglobin and lymphocyte (NHL) score would improve the ability to predict clinical outcome compared with neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII) in acute myocardial infarction (AMI). We examined 13,072 AMI patients from the Korean AMI Registry–National Institute of Health database. NHL score was calculated as follows: NHL score (U) = N/(Hb × L), where N, Hb, and L are baseline blood neutrophil, hemoglobin, and lymphocyte count. The primary outcome was the occurrence of major adverse cerebrocardiovascular events (MACCEs) at 2 years. The NLR, SII, and NHL score were independent predictors of 2-year MACCEs. The area under the curve of the NHL score (0.637) for predicting 2-year MACCEs was significantly higher compared with those of SII (0.589) and NLR (0.607). The NHL score significantly improved the reclassification and integrated discrimination compared with NLR (p < 0.0001) and SII (p < 0.0001). A high NHL score (≥ 0.35 U) was an independent predictor of 2-year MACCEs (adjusted hazard ratio, 1.41; 95% confidence interval, 1.29–1.55; p < 0.001). The NHL score could be a novel model for predicting long-term MACCEs in patients with AMI.
Introduction
A robust inflammatory response is an integral component of the response to tissue injury in patients with acute myocardial infarction (AMI).1 The neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII) are inflammation-related indicators that integrate neutrophil, platelet, and lymphocyte counts in the early stage of AMI.2-4 Therefore, the NLR and SII are available for risk prediction in patients with AMI. However, these have not been compared with other prognostic scoring systems of AMI. Moreover, the infarction-related inflammatory state with excess cytokine production may suppress erythropoiesis and impair intestinal iron absorption. Therefore, anemia is not uncommon in patients with AMI and can influence clinical outcome. 5 However, there has been no simple and effective inflammation-related indicator that integrates neutrophil, lymphocyte, and hemoglobin in patients with AMI. Therefore, we developed the neutrophil-to-hemoglobin and lymphocyte (NHL) score incorporating hemoglobin into NLR as a risk prediction model to determine the long-term prognosis of patients with AMI. We aimed to validate the NHL score as a risk prediction model and to assess whether the NHL score would improve the ability to predict clinical outcome compared with the NLR and SII in patients with AMI.
Methods
Study population
The Korean Acute Myocardial Infarction Registry (KAMIR) is a prospective, open, observational, multicenter, online registry of Korean patients with AMI supported by the National Institute of Health (NIH) since November 2011. The main purpose of KAMIR-NIH was to develop novel risk prediction model for AMI in Korea. Sample size calculation was performed based on the previous KAMIR I–III. This study was planned to recruit at least 12,000 AMI patients for 4 years from 20 hospitals. Between November 2011 and December 2015, a total of 13,072 patients from 20 hospitals who were diagnosed with AMI at admission were recruited. The inclusion criteria were all patients who were diagnosed with AMI. AMI was diagnosed based on the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia. 6 Exclusion criteria were patients who were diagnosed with AMI during hospitalization and patients who refused to participate in this study. Other details about the Korean Acute Myocardial Infarction Registry−National Institute of Health have been published previously. 7
Clinical assessment
We analyzed baseline demographic and clinical characteristics including age, sex, cardiovascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, and current smoking), and presenting characteristics at admission. Electrocardiogram was recorded and analyzed in all patients by attending cardiologists. Venous blood samples including neutrophils, lymphocyte, platelets, and hemoglobin were obtained at the time of admission. Biomarkers such as cardiac troponin I (cTnI), CK-MB, and high-sensitivity C-reactive protein (hs-CRP) were also measured at the time of admission.
The NHL score calculation
The NLR was calculated by dividing the neutrophil count by the lymphocyte count. We calculated SII using the equation SII = P × N/L, where P, N, and L are baseline peripheral blood platelet, neutrophil, and lymphocyte counts per liter, respectively. We calculated the NHL score using the equation NHL score (U) = N/(Hb × L), where N, Hb, and L are baseline peripheral blood neutrophil, hemoglobin, and lymphocyte count. The U indicates unit (1/g/dL).
Data analysis
All patient data and procedural details were collected at the time of admission and followed prospectively at each hospital. Data were recorded on a web-based report form with electronic encryption in the National Institute of Health database. This research was supported by the Korea Centers for Disease Control and Prevention (2013-E63005-02). The protocol was approved by the ethics committee of each participating institution, and all patients provided written informed consent to participate in the study. During the follow-up period, clinical outcome data were obtained by reviewing medical records and interviewing patients by telephone. Outcomes were adjudicated by an investigator at each participating hospital, and central adjudication was regularly performed through an audit.
Outcomes
The primary outcome was the occurrence of major adverse cerebrocardiovascular events (MACCEs) at 2 years, defined as the composite of all-cause death; non-fatal MI; repeat revascularization, including repeated percutaneous coronary intervention, and coronary artery bypass grafting; cerebrovascular accident; and rehospitalizations.
Statistical analysis
Data were expressed as mean
The increased discriminative value of the NHL score compared with the NLR or SII was estimated using three measures (Harrell’s C index, net reclassification improvement, and integrated discrimination improvement). Harrell’s C index (c-statistic) is defined as the proportion of usable patient pairs, in which the predictions and outcomes are concordant. 8 We estimated receiver-operating characteristic (ROC) curves and compared the areas under the ROC curves (AUC) of the NHL score, NLR, and SII in corresponding logistic models. 9 The net reclassification improvement and integrated discrimination improvement were calculated by analyzing the differences in individual estimated probability for 2-year MACCEs and mortality of the NHL score compared with the NLR or SII. Because no prior risk categories exist for 2-year MACCEs and mortality, we calculated the category-free net reclassification improvement. 10
Because the patients were not randomly assigned to NHL score, propensity-score (PS) matching was performed to reduce the effect of treatment-selection bias and potential confounding factors in this observational study. For each patient, a PS indicating the likelihood of a high NHL score was calculated using a nonparsimonious multivariable logistic regression model with covariates including baseline and angiographic characteristics, leaving 3661 NHL score < 0.35 U versus 3661 NHL score ≥ 0.35 U. Goodness of fit of the PS was evaluated using the c-statistic and the Hosmer–Lemeshow test. After PS matching, the cumulative incidence rates of 2-year MACCEs between NHL score < 0.35 U and NHL score ≥ 0.35 U were estimated by the Kaplan–Meier curve using the log-rank test. For all analyses, a 2-sided p value < 0.05 was considered statistically significant. Statistical analysis was performed using SAS software (version 9.3, SAS Institute, Cary, NC) and R Statistical Software (version 2.14.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinical characteristics of study subjects.
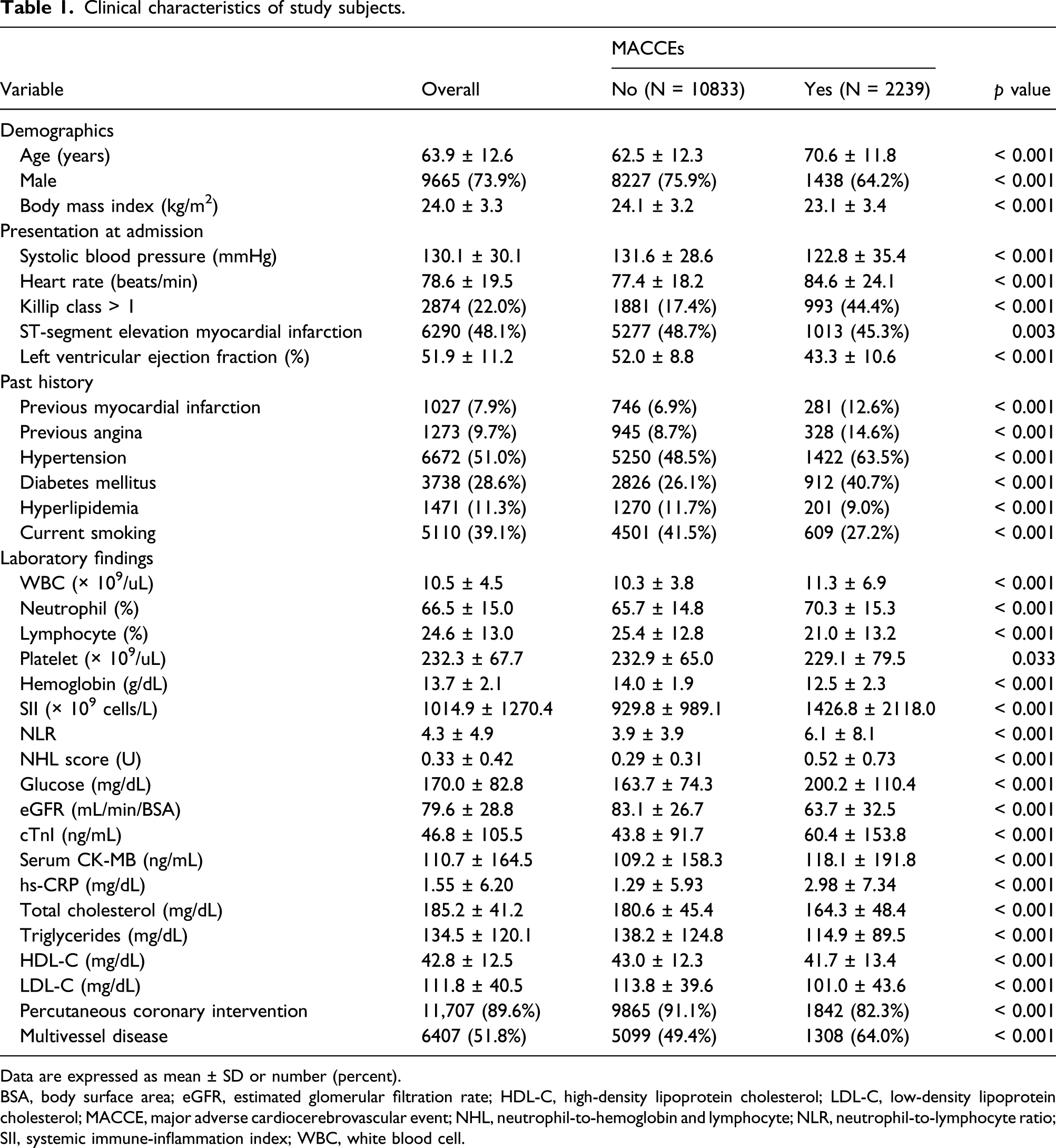
Data are expressed as mean ± SD or number (percent).
BSA, body surface area; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; MACCE, major adverse cardiocerebrovascular event; NHL, neutrophil-to-hemoglobin and lymphocyte; NLR, neutrophil-to-lymphocyte ratio; SII, systemic immune-inflammation index; WBC, white blood cell.
Cox-proportional hazards models for major adverse cardiocerebrovascular events at 2 years.

HR, hazard ratio; CI, confidence interval; NHL, neutrophil-to-hemoglobin and lymphocyte; eGFR, estimated glomerular filtration rate; BSA, body surface area; cTnI, cardiac troponin I; hs-CRP, high-sensitivity C-reactive protein.
In ROC curve analysis, the AUCs of the SII, NLR, and NHL score for predicting 2-year MACCEs were 0.589, 0.607, and 0.637, respectively (Figure 1(a)). The AUC of the NHL score was significantly higher compared with those of the SII (p < 0.0001) and NLR (p < 0.0001), as shown in Table 3. The NHL score significantly improved the reclassification (0.459; p < 0.0001) and integrated discrimination (0.020; p < 0.0001) of patients compared with the SII. The NLR also significantly improved the reclassification (0.227; p < 0.0001) and integrated discrimination (0.004; p < 0.0001) of patients compared with the SII. The NHL score significantly improved the reclassification (0.540; p < 0.0001) and integrated discrimination (0.015; p < 0.0001) of patients compared with the NLR. In terms of 2-year mortality, the AUCs of the SII, NLR, and NHL score for predicting 2-year mortality were 0.619, 0.644, and 0.681 in ROC curve analysis, respectively (Figure 1(b)). The NHL score significantly improved the reclassification (p < 0.0001) and integrated discrimination (p < 0.0001) of patients compared with the SII and NLR, respectively. (a) Receiver-operating characteristics analysis of the SII, NLR, and NHL scores for 2-year major adverse cardiocerebrovascular events and (b) mortality. AUC, area under the curve; CI, confidence interval; NHL, neutrophil-to-hemoglobin and lymphocyte; NLR, neutrophil-to-lymphocyte count ratio; SII, systemic immune-inflammation index. Discrimination of SII, NLRs, and NHL score in predicting 2-year clinical outcomes. The NRI was defined as (Pimproved prediction among patients with major adverse cardiocerebrovascular events or mortality + Pimproved prediction among patients without major adverse cardiocerebrovascular events or mortality) (Pworsened prediction among patients with major adverse cardiocerebrovascular events or mortality + Pworsened prediction among patients without major adverse cardiocerebrovascular events or mortality), where p = proportion of patients. The IDI was defined as (∑imajor adverse cardiocerebrovascular events or mortality (Pnew(i) Pold(i))/n (Patients with major adverse cardiocerebrovascular events or mortality)) (∑jno major adverse cardiocerebrovascular events or mortality (Pnew(j) Pold(j))/n (Patients without major adverse cardiocerebrovascular events or mortality)), where p = predicted probability of major adverse cardiocerebrovascular events or mortality. IDI, integrated discrimination improvement; MACCE, major adverse cardiocerebrovascular event; NHL, neutrophil-to-hemoglobin and lymphocyte ratio; NLR, neutrophil-to-lymphocyte count ratio; NRI, net reclassification improvement; SII, systemic immune-inflammation index.

Clinical characteristics in patients with high or low NHL score.

Data are expressed as mean ± SD or number (percent).
BSA, body surface area; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NHL, neutrophil-to-hemoglobin and lymphocyte; NLR, neutrophil-to-lymphocyte ratio; SII, systemic immune-inflammation index; WBC, white blood cell.

(a) Kaplan–Meier survival curve showing 2-year major adverse cardiocerebrovascular events, (b) death, (c) non-fatal MI, (d) revascularization, (e) CVA, and (f) rehospitalization according to high and low NHL scores. CVA, cerebrovascular accidents; MACCE, major adverse cardiocerebrovascular event; MI, myocardial infarction; NHL, neutrophil-to-hemoglobin and lymphocyte.
Cox-proportional hazards models for major adverse cardiocerebrovascular events at 2 years.

HR, hazard ratio; CI, confidence interval; NHL, neutrophil-to-hemoglobin and lymphocyte; eGFR, estimated glomerular filtration rate; BSA, body surface area; cTnI, cardiac troponin I; hs-CRP, high-sensitivity C-reactive protein.
After PS matching, there were no significant differences in baseline characteristics (Supplementary Table 2). In Kaplan–Meier survival curve analysis, there were significantly higher rates of 2-year MACCEs (23.9% vs 20.1%; log-rank p < 0.001) and mortality (16.1% vs 11.8%; log-rank p < 0.001) in patients with NHL score ≥ 0.35 U (Supplementary Table 3 and Supplementary Figure 3).
Discussion
The main findings of this study are as follows. First, the severity of systemic inflammation is closely associated with prognosis of AMI. Second, the NHL score is a novel inflammatory indicator in AMI. Third, the NHL score is an independent predictor of long-term outcomes in patients with AMI. Fourth, the NHL score has an ability superior to either the SII or NLR in the prediction of long-term outcome in patients with AMI.
There are two noteworthy findings in our study. First, this is the first risk-prediction model to incorporate anemia as one of the inflammatory markers in patients with AMI. In patients with AMI, the prevalence of anemia varies between 10% and 43%, depending on preexisting comorbidities.11-18 A previous large cohort study reported that AMI patients with anemia had more preexisting comorbidities compared with those of normal hemoglobin level. 19 This is consistent with the results of our study. In our study, patients with a high NHL score had greater previous history of hypertension, diabetes mellitus, hyperlipidemia, and current smoking. Accordingly, anemia at baseline should be regarded as a marker of “fragile” patients. Furthermore, anemia in AMI patients should be regarded as “anemia of inflammation” that is a part of the systemic inflammatory response syndrome. 20 Inflammatory response mediated by acute-phase cytokines results in a shorter half-life of red blood cells, antiproliferative action against endothelial progenitor cells, low iron availability for hemopoiesis, reduced erythropoietin production, and minor response of hematopoietic progenitors to stem cell factor and erythropoietin for receptor downregulation. 20 Therefore, the systemic effects of the inflammatory response induced by myocardial necrosis in AMI patients are not just limited to blunted erythroid function but also involve the ability to produce or mobilize endothelial progenitor cells by the bone marrow. 5 This systemic inflammatory response syndrome reduces the vascular healing capacity and contributes to worse clinical outcomes in AMI patients with anemia. 21 This is the reason why we developed the NHL score incorporating anemia into NLR as an inflammatory marker. In our study, the NHL score was an independent predictor of long-term outcomes in patients with AMI after adjusting for other inflammatory markers such as cTnI and hs-CRP.
Second, the NHL score has robust prognostic accuracy compared with the NLR and SII and adds additional prognostic risk stratification in patients with AMI. Many of the hematological indices, as biomarkers related to inflammation, have been studied to establish their prognostic value.22,23 Hematological indices such as white blood cell, neutrophil, lymphocyte, and platelet counts are relatively simple, rapid, and inexpensive. Previous studies have reported that increased neutrophils were associated with poor clinical outcome in patients with AMI.24-31 Neutrophils play a role in the destabilization of atherosclerotic plaque by the formation of neutrophil extracellular traps that contributed to atherothrombosis. 32 Conversely, increased lymphocytes were associated with lower mortality in patients with AMI.33,34 Therefore, the NLR is useful and better than each separate hematological index for predicting clinical outcome. 2 The SII is another inflammatory marker that incorporates platelets into the NLR. The activation of platelets plays a key role in thrombus formation, and its derivative contributes to sustained inflammation. 35 Recently, some studies have reported that higher SII is independently associated with worse clinical outcomes in patients with coronary artery disease, particularly among elderly AMI patients.3,4 In our study, we found that the SII was significantly greater in patients with higher MACCEs at 2 years. This result is consistent with previous studies. However, the NLR and SII have not been compared with other inflammation-related prognostic scoring systems in AMI. In our study, we developed a novel NHL score as an inflammation-related indicator in patients with AMI. The NHL score significantly improved the reclassification and integrated discrimination of patients and has an ability superior to either the SII or NLR in the prediction of long-term outcome in patients with AMI. We believe the NHL score might be the best risk-prediction model among inflammation-related indices in patients with AMI.
Study limitations
This study has certain limitations that should be noted. First, because the Korean Acute Myocardial Infarction Registry−National Institute of Health was an observational study, we could not completely exclude the possibility of residual confounding factors that were not available in our registry. Therefore, our results should only be regarded as hypothesis generating. Second, because some biomarkers were not routinely assessed, we did not compare the NHL score with various inflammatory indicators. However, the limitations of the study should not undermine the strength of this study, namely, that it includes patients encountered in day-to-day clinical practice. Despite these limitations, we believe that the NHL score could provide the clinical insight necessary to determine the future prognosis of patients with AMI.
Conclusion
An improvement in the ability of the NLR and SII to predict long-term MACCEs can be achieved by combining the NLR with anemia to produce the NHL score. The NHL score is a novel valid model of long-term MACCEs in patients with AMI.
Supplemental Material
sj-pdf-1-eji-10.1177_20587392211039095 – Supplemental Material for Prognostic value of novel neutrophil-to-hemoglobin and lymphocyte score in patients with acute myocardial infarction
Supplemental Material, sj-pdf-1-eji-10.1177_20587392211039095 for Prognostic value of novel neutrophil-to-hemoglobin and lymphocyte score in patients with acute myocardial infarction by Hyeon Jeong Kim, Jang Hoon Lee, Se Yong Jang, Myung Hwan Bae, Dong Heon Yang, Hun Sik Park, Yongkeun Cho, Myung H Jeong, Jong-Seon Park, Hyo-Soo Kim, Seung-Ho Hur, In-Whan Seong, Myeong-Chan Cho and Shung Chull Chae in European Journal of Inflammation
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of all the KAMIR-NIH investigators and their staff.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a fund (2013-E63005-02) by Research of Korea Centers for Disease Control and Prevention.
Ethics approval
The study was approved by the by the Institutional Review Board of Kyungpook National University Hospital (KNUH 2011-11-023) and was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
All patients gave written informed consent to participate in this study.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.