
Abstract
This study focused on using “General Practitioners–Specialists” (GP-S) mode to teach the patients with asthma to master inhalation skills. 200 patients with asthma being admitted to the respiratory department of Shanghai Changhai Hospital were included in the study from January to December in 2018. There were 100 cases in the control group and 100 cases in the experimental group. The control groups received routine instruction and the experimental group adopted GP-S mode education, respectively, to learn mastering dry powder inhaler skills. The level of mastery and errors in the use of inhaled medications were recorded after each guidance. After four times’ instruction in two different ways, the patient’s mastery of inhalation skills gradually improved. After the guidance through the GP-S mode, the incidence of inhalation errors after each times instruction was 67%, 28%, and 7%, respectively. The later one was significantly lower than the previous one (67% vs. 28%, χ2 = 30.496, p < 0.001; 28% vs. 7%, χ2 = 15.273, p < 0.001). After twice instructions, the GP-S mode was associated with the lower incidence of inhaler device operating errors versus the regular guidance method (10% vs. 26%, χ2 = 8.672, p = 0.005); the same as the third guidance (2% vs. 11%, χ2 = 6.664, p = 0.018). Similarly, after thrice instructions, the incidence of inhalation method errors in the GP-S mode group was significantly lower than the regular guidance mode group (4% vs. 15%, χ2 = 7.037, p = 0.018), and there was still existing statistical difference of inhalation method errors between the two groups after four times instructions (3% vs. 11%, χ2 = 4.916, p = 0.049). General Practitioners–Specialists mode can effectively improve the patient’s mastery of inhalation skills, which significantly reduced the incidence of errors in the use of inhaled drugs and improved the overall management effectivity of asthma and patients’ compliance.
Introduction
Bronchial asthma is one of the common chronic airway diseases and the focus of community chronic disease management. 1 The disease has a long course and is prone to repeated attacks, which seriously affects the health and quality of patients’ routine lives, resulting in a high psychological and economic burden. 2 The Global Initiative for Asthma(GINA) pointed out that inhaled corticosteroids are currently one of the most effective treatments for bronchial asthma, with better efficacy and less systemic adverse reactions. 2 However, most asthma patients do not obtain GINA-defined asthma control. In China, only 28.7% of asthma patients achieved asthma control, 3 and inhalational techniques largely affected the therapeutic effect of inhalation therapy. 4 As a general hospital with a national-level of general practitioners counseling base, Shanghai Changhai Hospital provided inhalation techniques guidance on asthma patients through a “General Practitioners–Specialists” (GP-S) mode. The aim of the study is explore GP-S mode to teach the patients with asthma to master inhalation skills.
Methods
Sampling
According to 1:1 parallel control design, a = 0.05, power = 90%, bilateral test, combined with the calculation formula and considering the possibility of dropping out of the study in clinical practice, the sample size was set as n = 200 cases. 200 patients with asthma in the respiratory medicine clinic of Shanghai Changhai Hospital from January 2018 to December 2018 were selected.
Inclusion criteria
Inclusion criteria are as follows: (1) meet the diagnostic criteria for bronchial asthma; (2) 18 years of age or older; (3) the severity of the disease is non-severe asthma; (4) the condition is non-acute attack; (5) being received or not received asthma standardized treatment; (6) have a certain level of education and communication abilities and participate in the study voluntarily after informed consent; and 7) patients received the similar type of DPI or pMDI inhaler.
Exclusion criteria
Exclusion criteria are as follows: (1) combined with other serious diseases; (2) existing communication barriers; (3) had received systematic normative education of inhalation techniques; and (4) poor compliance.
Two hundred patients were divided equally into an experimental group and a control group of 100 patients each by simple randomization. The general information of the two groups of patients was collected, including gender, age, duration of disease, and education level.
Study design and data collection
The study is a randomized, single-center, standardized controlled trial. Both groups were given budesonide and formoterol fumarate powder for inhalation (dose 160 μg/4.5 μg/puff), one inhalation a time, twice daily. The control group received the routine guidance method: Three specialists instructed the patient to use the inhaler with a form of “Asthma Class” in the outpatient clinic. The course covered the steps of operating the inhaler device, inhalation skills, and precautions and common mistakes. At least four times instructions, the interval of instruction was 7–14 days, not less than 15 min of each instruction and the intervention was 60 min in total, will be provided during the follow-up period. The teaching contents, course length, and instruction times of the experimental group were same as the control group but adopted the General Practitioners–Specialists (GP-S) mode as the guidance method: Firstly, the inhalation remedy of asthma patients was formulated by specialists. Then three general practitioners directed patients with inhalation skills in the form of “one-on-one” and “face-to-face,” and the guidance model is the same as the specialist group. The exact difference between the educational intervention in the study group and the control group is that the general practitioners in the experimental group not merely instructed and corrected the patient to operate the inhaler device but adjusted the patients’ treatment strategy with the specialist during the follow-up process.
Patients of both the groups’ assessment of the mastery of the inhalation skills took place after each instruction by other specialist or general practitioner; meanwhile, recording the errors that includes device operation errors and inhalation method errors during the therapy of inhaled drugs. Inhaler device operation errors or inhalation method errors would regard as patients did not master inhalation skills.
This study had received approval from Changhai Hospital Research Ethics Committee. Written and verbal consent to participate in the study was obtained from each participant. We confirmed that we had obtained consent to publish the article from all participants.
Data analysis
The association between the both groups in gender, age, duration of disease, and education level was examined by descriptive statistics. A specialist or general practitioner observed and documented the errors during the procession of inhalation therapy and by analyzing the errors found that common errors could be classified into two types: inhaler device operation errors and inhalation method errors. The former errors includes opening the inhaler improperly (without opening the slide bar or the rotating handle) and holding the venting hole by hand; the latter includes forgetting exhaling or exhaling incompletely or not exhaling quickly, putting the nozzle incorrectly (not covering the nozzle between lips and teeth), insufficient inspiratory flow rate or without a deep inhalation, no breath holding or holding time less than 10 s, and exhaling with the device or not exhaling away from the nozzle. Calculate percentages of the inhalation errors occurred in the both groups after each routine mode guidance or the “General Practitioners–Specialists” mode guidance. For measurement, data were expressed as mean and standard deviation (‾x±s), using T-test to compare between two groups, 2 and count data by χ2 All statistical tests were two-sided, and p < 0.05 was set as the level of significance. Statistical analyses were performed using SPSS 21.0 software.
Results
Of the 200 subjects, 100 were in the control group, including 55 men and 45 women with a mean age of 35.73 ± 10.48 years; the average course length of disease was 15.74 ± 21.11 month (range, 0.75–93 months). There were 85 cases with a university education level or above, 11 patients with high school education level, and four patients with junior high school education level. Regarding the experimental group, 53 men and 47 women were included with an average age of (35.65 ± 10.84) years; the average course length of disease was 12.84 ± 18.52 months (range, 0.25–99 months). Among the 100 patients, 84 had a university education level or above, 11 with senior high school education level, and three with junior high school education level. There was no statistical significance of general situation between the two groups (p>0.05) (Figure 1). Consort flowchart.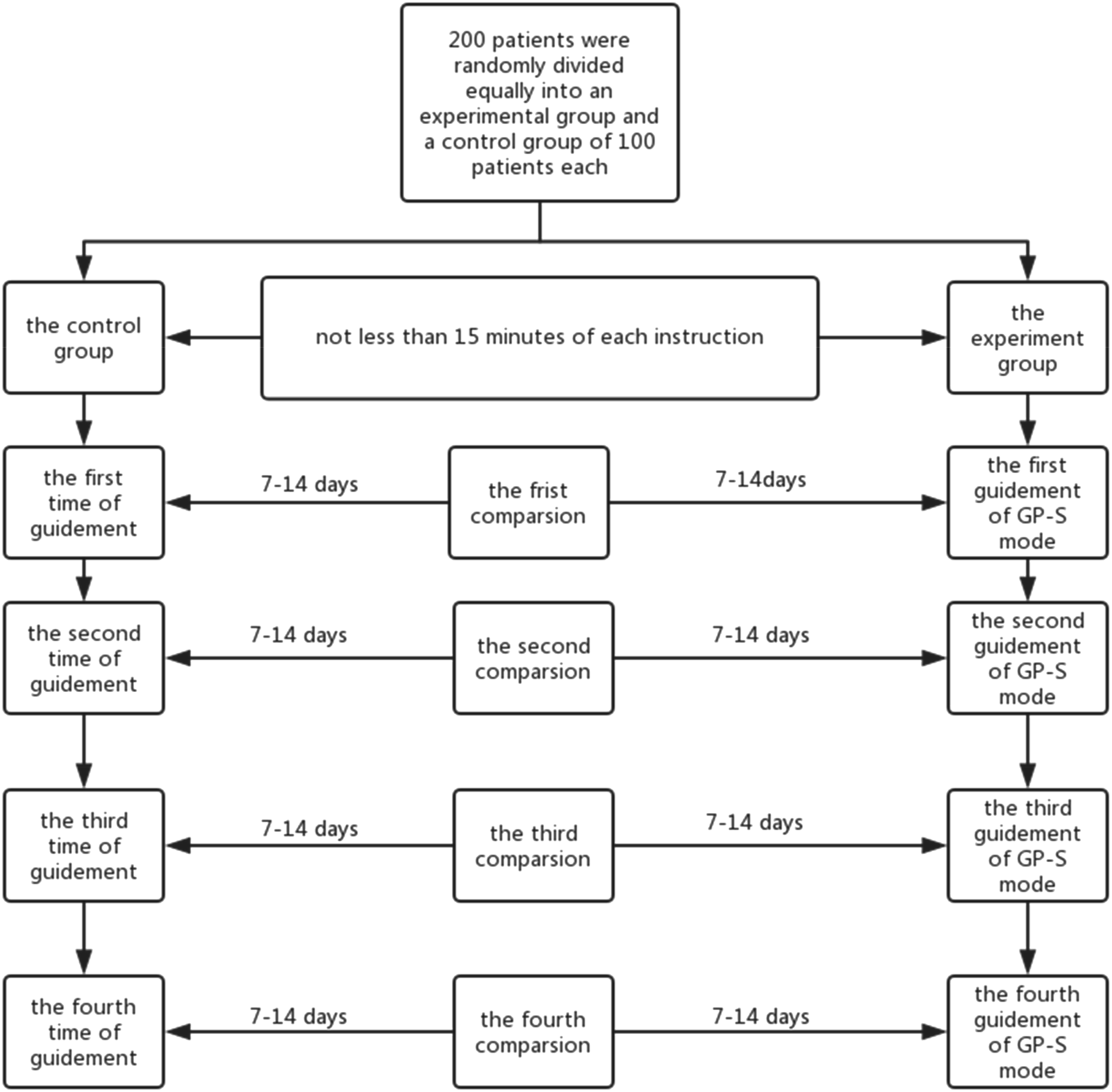
The main of errors during the educational intervention were inhaler device operation errors and inhalation method errors. At the level of detail, the former errors includes opening the inhaler improperly (without opening the slide bar or the rotating handle) and holding the venting hole by hand; the latter includes forgetting exhaling or exhaling incompletely or not exhaling quickly, putting the nozzle incorrectly (not covering the nozzle between lips and teeth), insufficient inspiratory flow rate or without a deep inhalation, no breath holding or holding time less than 10 s, and exhaling with the device or not exhaling away from the nozzle.
The study showed that after the guidance through the GP-S mode, the incidence of inhalation errors after each time instruction was 67%, 28%, and 7%, respectively. The later one was significantly lower than the previous one (67% vs. 28%, χ2 = 30.496, p < 0.001; 28% vs. 7%, χ2 = 15.273, p < 0.001). The incidence of inhalation errors was 6% after the fourth training session, which was not significantly improved compared with the third guidance (7% vs. 6%, χ2 = 0.082, p > 0.05) (Figure 2). Inhalation error rate in patients through the GP-S mode. *p <0.05, ** p <0.01, ***p <0.001, ns = not significant.
The control group used the routine guidance mode, and the incidence of inhalation error after each teaching was 69%, 49% and 27%, respectively, showing a gradual decline (69% vs. 49%, χ2 = 8.268, p = 0.006; 49% vs. 27%, χ2 = 6.452, p = 0.017), while there was no significance of the incidence of inhaling errors between the third and fourth routine guidance (27% vs. 19%, χ
Inhalation error rate in patients through regular guidance mode. *p <0.05, ** p <0.01, ***p <0.001, ns = not significant.
The study indicated that the GP-S instruction mode group was associated with a significantly advantage on the accuracy rate of inhalation skills compared to the routine mode guided group (Figure 4). Specifically, after the first instruction, the percentage of the mastery rate was 33% vs. 31%, χ2 = 0.092, p = 0.88; second instruction (72 vs. 51%, χ2 = 9.313, p = 0.004), third instruction (93 vs. 73%, χ2 = 14.174, p < 0.001), and fourth instruction (94 vs. 81%, χ2 = 7.726, p = 0.009). Inhalation skills accuracy rate in patients of the two guidance modes. *p <0.05, ** p <0.01, ***p <0.001, ns = not significant.
Via comparing the inhalation error rate between the two groups, the study illustrated that after twice instructions, the GP-S mode was associated with the lower incidence of inhaler device operating errors (10% vs. 26%, χ2 = 8.672, p = 0.005) and so was the third guidance (2% vs. 11%, χ2 = 6.664, p = 0.018) (Figure 5). Similarly, after thrice instructions, the incidence of inhalation method errors in the GP-S mode group was significantly lower than the regular guidance mode group (4% vs. 15%, χ2 = 7.037, p = 0.018), and there was still existing statistical difference of inhalation method errors between the two groups after four times instructions (3% vs. 11%, χ2 = 4.916, p = 0.049) (Figure 6). Comparison of inhaler device operation errors between the two groups. *p <0.05, ** p <0.01, ***p <0.001, ns = not significant. Comparison of inhalation method errors between the two groups. *p <0.05, ** p <0.01, ***p <0.001, ns = not significant.

Discussion
Inhalation therapy is currently the prior choice for the treatment of asthma worldwide and the preferred approach of drugs delivery advocated by GINA. 3 However, it had been found clinically that most patients might be unable to correctly grasp the inhalation skills and the operation of inhaler devices, resulting in an undesirably controlling efficacy of asthma. 5 Appropriate guidance needs to be provided to assist the patient in the proper use of the inhaler and to accurately master inhalation techniques throughout the course of inhalation therapy. 6 Some scholars believe that only the inhalation technique instructed by a specialist most patients can master the using of inhaler devices correctly. 7 Hitherto, there is no consensus on the requirement of teaching patients to operate inhaler devices and grasp inhalation methods repeatedly. Studies have shown that after three times education of inhaler technique the correct rate of inhaler devices using can be increased to 91.8%.5,8
Similar results have been demonstrated in the study. The incidence of inhalation errors were gradually reduced after instruction via the regular guidance mode or the GP-S mode. There was no statistically significant difference between four times and thrice educations in the incidence of inhalation errors of both groups. The study also indicates that it is necessary to teach patients repeatedly, at least three times, on operating inhaler devices and inhalation skills. Simultaneously, assess the mastery situation of inhalation techniques and correct the relevant errors timely to ensure the correctness and effectiveness of inhalation therapy for asthma patients.
Further research of the study illustrated that there was a higher correctness rate of inhalation skills in patients who received the GP-S mode after each instruction compared to patients who received the regular guidance mode. Remarkably, only after twice instructions, patients who adopted the GP-S mode the mastery degree of inhalation techniques can be significantly improved. As well, this guidance method could deepen patients’ understanding of the pinpoints of inhalation techniques in an earlier time. All that reflects that the GP-S mode had a better guidance effect and a higher guidance efficiency.
After thrice instructions through the GP-S mode, the error rate of inhaler device operating and inhalation method was only 2% and 4%, respectively, which indicating that this mode can significantly improve the drug inhalation skills for asthma patients and enhance their self-management ability in asthma.
Therefore, the GP-S mode has the clinical meaning in conducting bronchial asthma patients to correct grasping of inhalation skills correctly. On the one hand, the mode could provide patients in both a professional direction and a full-course of following-up. A more professional knowledge of specialists is beneficial to the diagnosis, condition estimation, treatment remedies, and decision of asthma, whereas for some reasons it is difficult to manage the asthma patients in every regard. Adopting the GP-S mode, general practitioners can perform successive instruction on the behavior of patients with chronic diseases, support knowledge of inhalation skills, and improve the control efficacy of asthma. On the other hand, the GP-S mode facilitated to forms a stable and positive physician–patient relationship and strengthened families’ support for patients. Family function could significantly affect the control level of asthma in patients. 9 Studies have shown that harmonious relationship of family members united and positive communication with medical staff are conducive to the curb of asthma symptoms and the reduction of airway inflammation. 10 At the same time, general practitioners were inclined to support asthma patients with scientific, active guidance to improve their self-management ability in the controlling of chronic disease. Playing an important role in family doctors, general practitioners could enter into families to assist patients and their families to establish a cooperative, optimistic psychological state, which contributed to coordinate asthma management and a routine life. The balance relationship helps the patient’s family and patients to integrate into the whole process of asthma management. 11 In addition, the GP-S mode allows the specialist to form a certain general medical concept in daily diagnosis and treatment and pay attention to the full-scale management of the whole asthma course. For general practitioners, the mode is contributed to promote the understanding of specialized diseases, consolidate clinical techniques, access to advances in related disciplines, and improve the clinical diagnosis and treatment capabilities.
The limitations of this study including (1) there may be differences in the understanding of the inhalation technique among the study subjects, which may lead to deviations in the actual operation, and it is necessary to expand the sample for stratified study. (2) Due to the short study time, this study failed to track the influence of the “GP-S” model on long-term inhalation technology mastery in bronchial asthma patients. (3) The applicability and operability of “GP-S” mode need to be further studied in combination with the actual situation of each unit. (4) Excluding patients with poor compliance.
Conclusion
General Practitioners–Specialists mode can effectively improve the patient’s mastery of inhalation skills in DPI or pMDI users, which significantly reduced the incidence of errors in the use of inhaled drugs and improved inhalation skills of asthma.
Footnotes
Acknowledgments
The authors would like to thank all the patients, specialists, and general practitioners who took part in this study. We also thank everyone who contributed to the recruitment of participants.
Author contributions
All authors were contributed to the conception of the project and analyzed the data. Yiping Han is Jiayi Zhao’s academic supervisor. Jiayi Zhao was responsible for data collection and analysis with output from Rong Chai and Rong Zhang. Jiayi Zhao, Jian Fan, and Rong Chai drafted the manuscript, which Yiping Han commented on and edited; the final manuscript was read and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to the protection of participant confidentiality.
Ethical approval
This study had received approval from Shanghai Changhai Hospital Ethics Committee. Written and verbal consent to participate in the study was obtained from each participant. Number of Ethics Committee approval: CHEC2020-097.
Consent for publication
We confirmed that we had obtained consent to publish the article from all participants.