
Abstract
Although allergic rhinitis is considered a raising medical problem in many countries it is often undertreated. The reasons for this phenomenon are not completely clear.
The aim of this study is to evaluate factors associated with allergic rhinitis under-/no treatment.
A sample of 518 allergic rhinitis patients recruited by their primary care physicians, as a part of the ARGA study, were invited to fill in a specific questionnaire regarding rhinitis symptoms, treatment, and rhinitis-related work/social disability. Chi-square test and logistic regression were performed to assess risk factors for allergic rhinitis under-/no treatment.
Over one out of four patients had no treatment despite the symptoms and 13.5% were inadequately treated. Participants with asthma (OR 0.47, 95% CI 0.30–0.75) and conjunctivitis (0.44, 95% CI 0.27–0.71) were at lower risk of allergic rhinitis under-/no treatment: in asthmatics this reduction was related mainly to the concomitant asthma treatment (OR 0.19, 95% CI 0.10–0.37).
Asthmatics with under-/not treated rhinitis had the highest prevalence of rhinitis-related quality of life impairment.
Under-/no treatment for allergic rhinitis is still rather frequent despite the relevance of this disease. The simultaneous presence of asthma and an anti-asthmatic therapy are able to influence positively the treatment. Targeted interventions toward a better characterization and a tight follow-up of rhinitis patient without asthma are needed.
Keywords
Introduction
Allergic rhinitis is characterized by a considerable medical and social burden, mainly because of its high prevalence in industrialized countries, the relationship with asthma and the impact on quality of life.1,2 In Italy, a rise in allergic rhinitis prevalence, from 16.8% to 25.8% over the last 20 years, in a particular setting has recently been reported. 3 Furthermore, there is increasing evidence that allergic rhinitis is also a rising medical issue in regions of the world other than Europe and North America. 4 Besides, the economic impact of allergic rhinitis remains substantial: in the USA, the total direct medical cost of allergic rhinitis is approximately $3.4 billion per year; 5 in Sweden the cost of rhinitis in terms of lost productivity is €2.7 billion per year. 6 Such data reinforce the need to implement the guidelines for early diagnosis and effective treatment of allergic rhinitis prepared by scientific societies and expert panels. 7 However, allergic rhinitis is still considered a trivial disease by some physicians, resulting often in underdiagnosis and inadequate treatment. 8 Recently, some authors also pointed out that patients’ compliance to the treatment, properly prescribed by their physicians, is very poor. 9 Under-/no treatment of allergic rhinitis is associated with delayed medical examinations, patient preference for non-prescribing drugs, and the fear of drug-related costs, but the specific characteristics of patients undertreated or not treated for allergic rhinitis are still not completely clear. 7 Having information on which group of patients needs more attention in terms of education, follow-up, and adherence to the therapy could help tailoring practical interventions by general practitioners and specialists toward a better control of allergic rhinitis symptoms. The aim of this study is to elucidate predictors of allergic rhinitis under-/no treatment in participants recruited by their general practitioners, as a part of the ARGA study,10–12 focusing mainly on patients characteristics, type of symptoms, and on the relationship between allergic rhinitis and asthma.
Methods
Study population
This survey is a part of the ARGA study (‘Allergopatie Respiratorie: studio di monitoraggio delle linee guida GINA e ARIA’), 10 funded by the Italian Drug Agency (AIFA) and performed between March 2007 and February 2010. The study was carried out in collaboration with a random sample of 27 general practitioners (GPs) and family pediatricians (FPs) of Perugia Province (Umbria, Italy), an area of 671,820 inhabitants. GPs and FPs were invited to administer a questionnaire to their patients when they came to their offices with symptoms suggesting an allergic rhinitis, enrolled consecutively, during the period January 2008 to December 2009. All 750 patients recruited by GPs and FPs were accepted to participate in the study; in Figure 1 the patient recruitment and selection flow chart are described. Briefly, 662 patients had symptoms suggesting allergic rhinitis by ARIA guidelines; 13 among them, 144 were excluded due to missing information (e.g. sex, age, answers to the key questions). Each of the 518 participants provided written informed consent for the participation in the study, anonymous management of individual and collective data, as well as anonymous publication of the research results. The study protocol, patient information sheet, and consent form were approved by the Ethic Committee of the Region Umbria (CEAS Umbria).

Flow chart of the study population enrolment and selection.
Questionnaire
“Allergic rhinitis” was defined as having watery runny nose with one or more of the following: (1) nasal itching; (2) sneezing; and/or (3) nasal obstruction. 13 Symptoms were classified as perennial if they were present almost all year round or seasonal if they were present in just some seasons. Patients reporting a skin prick test (SPT) positive reaction only to grass pollen and/or tree pollen and/or other seasonal allergens were included in the category “seasonal allergens sensitization”, while a SPT positive reaction only to dust mites and/or cat and/or dog and/or other perennial allergens was defined as “perennial allergens sensitization”. If the patient reported a SPT positive reaction to seasonal and perennial allergens he/she was classified having “both sensitization”. A SPT positive response to food was defined as “food allergens sensitization”. Rhinitis-related quality of life (QoL) impairment, indicating a “disabling rhinitis”, was identified by an affirmative answer to one or more questions on sleep, work, and school or everyday life impairment (Figure 2). Participants were classified as having “asthma” if they reported in the questionnaire asthma-like symptoms (wheezing, shortness of breath, chest tightness) or use of medication for asthma. To avoid a possible overlap with chronic bronchitis and to increase the likelihood of asthma diagnosis, a score system for some key questions (e.g. having cough and phlegm as cough characteristic) was set up. Participants with allergic rhinitis who reported no treatment for this disease were classified as “not treated”, whereas participants with a rhinitis-related QoL impairment, characterized by a poor control, who were treated just with antihistamine and/or vasocostrictor as needed, but needing by ARIA guidelines a more continu-ous treatment, were classified as “undertreated”. Patients not treated or undertreated formed the category “under-/not treated” and in the logistic regression analysis (see below) were those having “under-/no treatment”.

Quality of life impairment of the allergic rhinitis patients treated and under-/not treated, divided by the occurrence of asthma.
Statistical analyses
To assess the distribution of subject characteristics among patients treated, not adequately treated and not treated, the chi-square test was used; a two-tailed test with a 5% level of significance was considered appropriate for the analysis. A similar subgroup analysis was conducted dividing each treatment class in subject with or without asthma, calculating chi-square test for trend. Risk factors for under-/no treatment were evaluated by logistic regression models, adjusting for sex and age. Independent variables were those factors not equally distributed in the different treatment categories by the chi-square test. In one regression model the overall under-/no treatment risk was considered. Since the presence of asthma appears an important factor also able to influence rhinitis treatment, another regression analysis was performed in asthmatics only, adding a treatment for asthma as a possible influencing factor. The goodness of fit of the logistic regression models was confirmed by the Hosmer-Lemeshow test. 14 Statistical analyses were performed with the statistical software package SPSS Statistics 20.0 (IBM SPSS, Chicago, IL, USA).
Results
A total of 136 (26.3%) participants with self-reported symptoms of allergic rhinitis received no pharmacological treatment, 70 (13.5%) patients were undertreated; for reasons of sampling size comparability they were placed together in the category “Under-/no treatment” and compared to those treated (Table 1).
Characteristics of the allergic rhinitis patients treated and under-/not treated.

AR, allergic rhinitis; SPT, skin prick tests.
Almost all the patients (99.6%) had undergone skin prick test for common aero-allergens which had resulted positive (Table 1). The percentage of patients with perennial symptoms and perennial allergens sensitization was higher in those under-/not treated, while the proportion of participants with seasonal allergens sensitization was lower in this latter group (Table 1). Out of 518 patients, more than an half (51.4%) reported a disabling rhinitis causing a sleep/work/life impairment. After stratifying the two categories of rhinitis patients by presence/absence of asthma (Table 2), those with asthma showed higher frequency of perennial symptoms, as well as lower frequency of conjunctivitis.
Characteristics of the allergic rhinitis patients treated and under-/not treated divided by the occurrence of asthma.
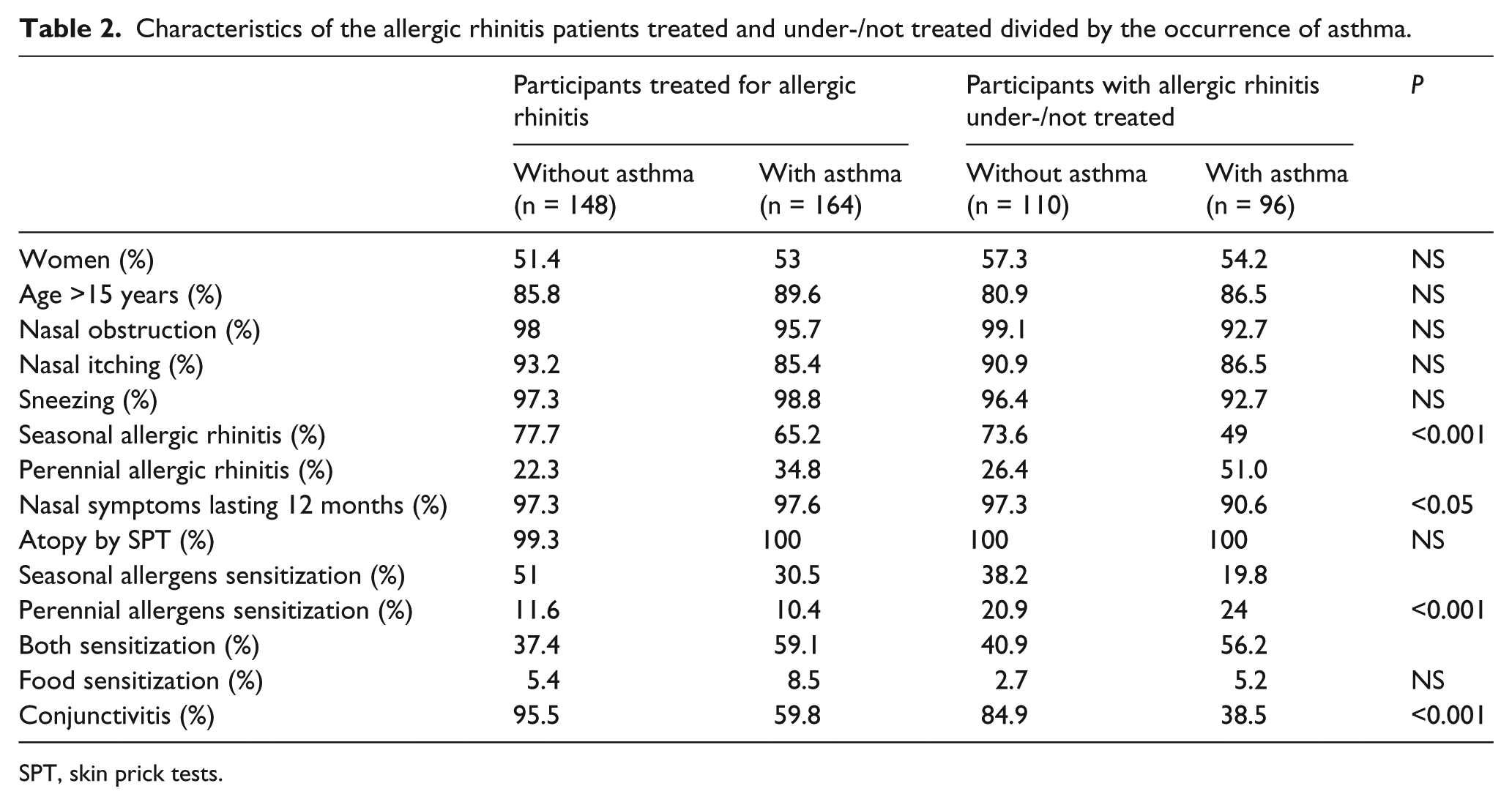
SPT, skin prick tests.
Prevalence of quality of life impairment significantly increased from the group of patients treated without asthma to the group of patients undertreated/not treated with asthma (Figure 1). This trend was also evident for each of the three specific domains.
In the logistic regression model performed in the whole population, adjusting for sex and age, participants with conjunctivitis or asthma had a lower risk of under-/no treatment (Table 3). In another model, limited to asthmatics, the role of conjunctivitis was confirmed and participants in treatment for asthma were at lower risk of rhinitis under-/no treatment, whereas patients with perennial sensitization alone were at higher risk of rhinitis under-/no treatment (Table 4).
Predictors of allergic rhinitis under-/no treatment, adjusted for sex and age.

Predictors of allergic rhinitis under-/no treatment in asthmatics, adjusted for sex and age.

Discussion
Main findings
In this study risk factors for allergic rhinitis under-/no treatment have been evaluated. The presence of asthma and conjunctivitis was associated with a more adequate treatment.
Allergic rhinitis undertreatment has previously been explored but did not focus on individual/disease characteristics. For example, in a large European survey over half of patients with rhinitis had not seen a physician in the last year, preferring either non-prescription medication or nothing, mainly due to the high cost of drugs. 7 Hence, even if allergic rhinitis is widely accepted as clinically relevant and disabling, 15 a not negligible proportion of patients are still considering it as a trivial disease. 8 In our survey, over half of the patients had an impairment of their daily/social life, in particular sleep impairment, confirming previous findings. 5 As regards sleep disturbances, it is to point out that they might have an important effect on mental health, including increased depression, anxiety, and alcohol abuse. 2
In the univariate analysis the prevalence of rhinitis under-/no treated was lower in patients with a sensitization to seasonal allergens, the reason of this finding is to be elucidated. It is possible that patients with seasonal sensitization and symptoms experience intense symptoms related to the peaks of pollen exposure 16 which drive them to seek for medical attention. Indeed, global climate changes have been related to increase in pollen concentration over the last 20 years. 17 On the other hand, in the univariate analysis participants with perennial sensitization and symptoms tend to be under/not treated, especially when asthma coexists. We hypothesize that either patients experienced less serious symptoms throughout the year, not driving them to seek for medical attention, or their doctors tend to concentrate their effort in treating the concomitant asthma symptoms. Furthermore, participants with a perennial allergen sensitization, since symptoms usually are continuous, could underestimate the importance of following a correct treatment. It is known that lack of efficacy, side effects, treatment duration, and costs are associated with a lower compliance to allergic rhinitis treatment. 18 In a recent Spanish survey, just 15% of allergic rhinitis patients sensitized to dust mites reported an improvement after pharmacological treatment. 19 Another possibility would be that patients with perennial allergic rhinitis do not take adequate treatment due to an effective allergen avoidance. A recent update of the Cochrane Review on house dust mites avoidance and allergic rhinitis stated that dust mites impermeable bedding and other preventive measures are not proven to give a substantial benefit to control rhinitis symptoms. 20
The role of asthma in the difference between perennial and seasonal allergic rhinitis needs to be further evaluated. We have shown in another study, with general practitioners from other Italian regions, that GPs tend to be more compliant with ARIA guidelines while treating allergic rhinitis alone than allergic rhinitis + asthma patients 21 . Conversely, in the present study in the Umbria region, the logistic regression analysis, adjusting for sex, age, and rhinitis symptoms/sensitization seasonality, demonstrated that asthma and conjunctivitis are the only two independent factors able to influence the treatment for allergic rhinitis. The results on asthma and conjunctivitis suggest that those with associated co-morbidity might have a more severe disease or be more aware of it; alternatively, they might just be more under control by their physician because of the associated diseases. When limiting the analysis to asthmatics patients, this hypothesis is insofar as asthmatics under therapy are at lower risk of rhinitis under-/no treatment. It is known that in asthmatics a coexistent allergic rhinitis increases the severity of asthma 11 as well as the annual number of GPs visits, 22 thus increasing the likelihood to be properly treated also for allergic rhinitis. Moreover, the presence of ocular symptoms worsens the quality of life of rhinitic patients 23 and this could push the patient to be more compliant with the allergic rhinitis treatment since the pharmacological treatments are often the same. 13 As a matter of fact, the presence of conjunctivitis has been associated with an increased number of allergic rhinitis drug prescriptions. 24
A possible limitation of our study might be the sample size. However, the peculiarity of the study population (a homogeneous group of participants coming from the same small Region, sharing the same healthcare system, recruited by a small team of primary care physicians) and the presence of analogous numbers in similar surveys 25 may overcome such limitations.
Conclusions
In this study of patients with allergic rhinitis recruited by their primary care physicians, more than 25% had no treatment despite the symptoms and 13.5% were treated inadequately. Patients with asthma, especially if treated with anti-asthmatics medications, and conjunctivitis were at lower risk of being under-/not treated. These findings strengthen the need of targeted educational interventions on selected groups of patients and primary care physicians towards a better characterization and a tight follow-up of the disease
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was a part of the ARGA study (‘Allergopatie Respiratorie: studio di monitoraggio delle linee guida GINA e ARIA’) supported by the Italian Drug Agency (AIFA).