
Abstract
To determine the impact of two varying doses of dexmedetomidine (DEX) on the onset and duration of neuromuscular blockade of rocuronium (ROC) under the condition of sevoflurane anesthesia. Eighty-one patients, American Society of Anesthesiologists Class I–II, were stochastically allocated to control group (group C) and two DEX groups (group D1 and group D2). In group D1 and group D2, DEX (0.5 and 1.0 µg/kg, respectively) was administrated 10 min before induction of general anesthesia. In group C, equivalent saline was infused by the same way. We monitored heart rate (HR), blood pressure, and train-of-four (TOF) values of all subjects in the period of anesthesia. We recorded times to reach TOF value 0 (T0, from injection of ROC to disappearance of all four twitches) as the onset time and TOF value 25% (T25, ratio of fourth twitch to first twitch,) as clinical duration of neuromuscular blockade. A total of 81 patients were randomized, 75 of whom accepted treatment, including group D1 (n = 25), D2 (n = 25), and C (n = 25). T0 time of three groups was found to be similar. The duration of action for ROC in group D2 was 62.76 ± 6.33 min, which was much longer than that in group D1 and group C, which were 42.64 ± 3.92 and 42.56 ± 4.04 min (p < 0.05), respectively. At T2 (after DEX administration) and T4 time point (10 min after trachea intubation), compared with group C, the changes of heart rate (HR) and blood pressure in DEX groups (group D1 and group D2) show greatly differences. Otherwise, there were no obvious differences among different groups at the other monitoring point-in-time. DEX infusion in general anesthesia has no obvious effect on the onset of ROC, but it is capable of prolonging its clinical effect time, which can provide reference for rational application of DEX and ROC in general anesthesia.
Introduction
Rocuronium (ROC), an non-depolarizing muscle relaxant, has a brief onset of action. Its onset is shorter than that of other non-depolarizing muscle relaxants in clinically relevant doses, ranging from 60 to 90s, and an optimal intubating condition can be achieved. 1
Dexmedetomidine (DEX) is a α2-adrenoceptor agonist with higher specificity and selectivity. DEX can activate postsynaptic α2-adrenoceptor, which could inhibit the release of norepinephrine, thus inactivating the sympathetic nervous system, playing an important role in anxiolysis, sedation, and analgesia. In addition, DEX has a significant effect in reducing heart rate (HR) and blood pressure. 2
A large amount of studies have reported the clinical duration of single muscle relaxant. In fact, it is impossible to use muscle relaxant alone in general anesthesia, which onset and duration of action must be affected by other drugs. However, DEX, as a new sedative and analgesic drug, is widely used in clinic, but its effect on ROC is still uncertain and needs further research. Animal experiments in some studies indicate that the high concentrations of DEX can enhance the neuromuscular blockade of ROC, but have no therapeutic effect. 3 The work aims to evaluate the influence of two varying dosages DEX on the onset time and duration of neuromuscular blockade of ROC under the condition of sevoflurane anesthesia, thereby providing more evidence and guide technical for clinical.
Materials and methods
This work was a randomized, multicenter, parallel-group, safety-assessor-blinded, active-controlled Phase IIIa trial, called Spectrum research. Moreover, obtaining approval from Independent Ethics Committee at each center, the protocol fully complied with the newest version of the International Conference on Harmonization Guidelines, the Declaration of Helsinki, Good Clinical Practice and law issued today. Registration number and name of trial registry are ChiCTR-IOD-17013079 and China Clinical Trial Registry, respectively. In addition, the full trial protocol can be downloaded in the website of http://www.chictr.org.cn. The study implemented in the Department of Anesthesiology, Shanghai Jiaotong University Affiliated Sixth People’s Hospital and the duration of the study was started from October 2016 to September 2017.
The preliminary trial was conducted with the dexmedetomidine group (DEX 1.0 µg/kg) and the control group (the same dose of normal saline). The onset and duration of action of the subject’s muscle relaxant drug rocuronium were used as the observed outcome indicators. According to literatures and preliminary test results, the duration of action of the control group was 42.64 ± 4.02 min, and the duration of action of the treatment group was 56.53 ± 5.32 min, set bilateral as α = 0.05, and the power was 90%, using MedSci sample size calculation software ( MedSci Sample Size tools, MSST), the two independent sample could be compared.
The preliminary experiment only made a comparison between the 1.0 µg/kg DEX group and the control group. Due to the obvious difference, the 0.5 µg/kg DEX group was added in actual study, which is planned to explore the effect of DEX’s dose on muscle relaxants. Therefore, three different groups were designed based on the preliminary trial, which are the D1 group (DEX 0.5 µg/kg), the D2 group (DEX 1.0 µg/kg) and the control group C, respectively. With reference to the number of cases in actual clinical work that meet the criteria for inclusion in the experiment, 25 cases in each group is much larger than the sample size calculation results obtained from the two sets of pre-experimental data.
After obtaining the support of the Ethics Committee and consent form of the subjects, seventy-five patients were enrolled to our double-blinded randomized clinical trial. Inclusion standard includes American Society of Anesthesiologists (ASA) physical status I-II, ages from 20 to 65 years, BMI ranges from 18 to 23 kg/m², undergoing elective surgery (posterior lumbar interbody fusion, PLIF). Exclusion criteria includes clinical history of heart, lung, kidney, liver, or neuromuscular disease, alcoholism or drug use, anemia, abnormal serum electrolyte, or more. No history of drug therapy neuromuscular blockers was found in the patients.
After reaching the operation theater, we cannulated an 18-G catheter into patients’ hand vein, monitored electrocardiogram (ECG), noninvasive arterial blood pressure (NIBP), as well as arterial oxygen saturation (SpO2) and measured their values.
After measuring the baseline, 81 sufferers were stochastically allocated to 3 groups via permuted block randomization, which were group D1 (n = 27), D2 (n = 27), and C (n = 27), respectively. However, in the group D1 (DEX 0.5) and group D2 (DEX 1.0), DEX, 0.5 and 1.0 µg/kg, was infused in 10 min before induction of general anesthesia, respectively. Meanwhile, in group C (Control), equivalent normal saline (NS) was infused by the same way. During the study, consent forms were provided by all subjects. The approval number of Shanghai Jiaotong University Affiliated Sixth People’s Hospital Ethics Committee is 2015-KY-007(K)-(1).
After completing administration of incipient dosages of DEX or NS, we induced anesthesia applying 1.5–2.0 mg/kg propofol, 3 µg/kg fentanyl. Later, we intubated trachea subsequent to administration of ROC 0.6 mg/kg when the train-of-four (TOF) value reached 0. However, 3% sevoflurane was continued to use for anesthesia. We adjusted ventilation to keep end-tidal CO2 (EtCO2) 35–40 mmHg. Blood pressure, HR, SpO2, and EtCO2 values of all subjects in the period of anesthesia were monitored. During the intraoperative infusion, the infusion dose of propofol was changed, and fentanyl dose was also changed according to the operative needs and hemodynamic changes (20% increase or decrease in systolic blood pressure or HR in contrast to baseline), while sevoflurane dose remained stable in the period of anesthesia.
We surveyed neuromuscular block via TOF acceleromyography (TOF Watch S; Organon Ireland) applicable to the ulnar nerve. We cleaned the area above the ulnar nerve for supplying sufficient electrode contact. When propofol was injected, the nerve stimulator was switched on and started monitoring. The stimulation was set as TOF pattern. The surface electrode was set as a pulses of 0.2 ms duration, delivered as a frequency 2 Hz, at intervals of 12 s.
The hemodynamic changes were recorded at these five time points, before DEX administration (T1), after DEX administration (T2), before trachea intubation (T3), 10 min after trachea intubation (T4), and 30 min after trachea intubation (T5). We recorded the time from injection of ROC to reach of TOF value 0 (disappearance of all four twitches, T0) as the onset time and the time from T0 to return of TOF value 25% (ratio of fourth twitch to first twitch, T25) as clinical duration of neuromuscular blockade.
We recorded adverse reaction, including bradycardia (<50 bpm), hypotension [mean arterial pressure (MAP) <60 mmHg], anaphylaxis, respiratory arrest (respiratory rate <8/min), and delayed recovery. If bradycardia happened, atropine (0.5 mg) was administrated via i.v.; in case of persistence existence of bradycardia, we would gave the same dosage. It was planned that ephedrine (5 mg) was administered via i.v. for treating hypotension, and the equivalent dosage can be utilized repeatedly if necessary.
Statistical analyses were accomplished with SSPS 19.0 software. Onset time and duration of action in the three groups were compared using one-way ANOVA. However, the parametric variables were analyzed by the analysis of variance ANOVA and post-hoc test. The p-values less than 0.05 were considered as statistically significant. To compare the results throughout the study, we used Generalized Linear Mixed model (GLMM) to further illuminate the data. We assessed sample size adopting sample size calculator software with 95% CI, p = 0.05 and power of 80% and difference between the two groups of 30% in main consequence in line with preliminary investigation.
Results
General data comparison of patients in each group
As the consort diagram shows in Figure 1, 81 patients enrolled in the trial, but 6 cases were excluded from the survey on account of some other reasons. Hence, efficient data analysis was collected from 75 patients. The features of the subjects (age, gender, height, weight, and body mass index) were presented in Table 1, which indicated that no obvious differences among the three groups (p > 0.05). Otherwise, T0 and T25 times of three groups are summarized in Figure 2. Duration of onset (T0) was 71.92 ± 7.89 s in the group D2, 71.44 ± 8.75 s in the group D1 and 75.84 ± 9.39 s in the group C. Duration of onset harbored no evident difference among three groups (p > 0.05) (Figure 2). However, the clinical duration of neuromuscular blockade (T25) in group D2 (62.76 ± 6.33 min) was obviously longer than that in group D1 (42.64 ± 3.92 min) and group C (42.56 ± 4.04 min), which displayed significantly difference among them (p < 0.05) (Figure 2).
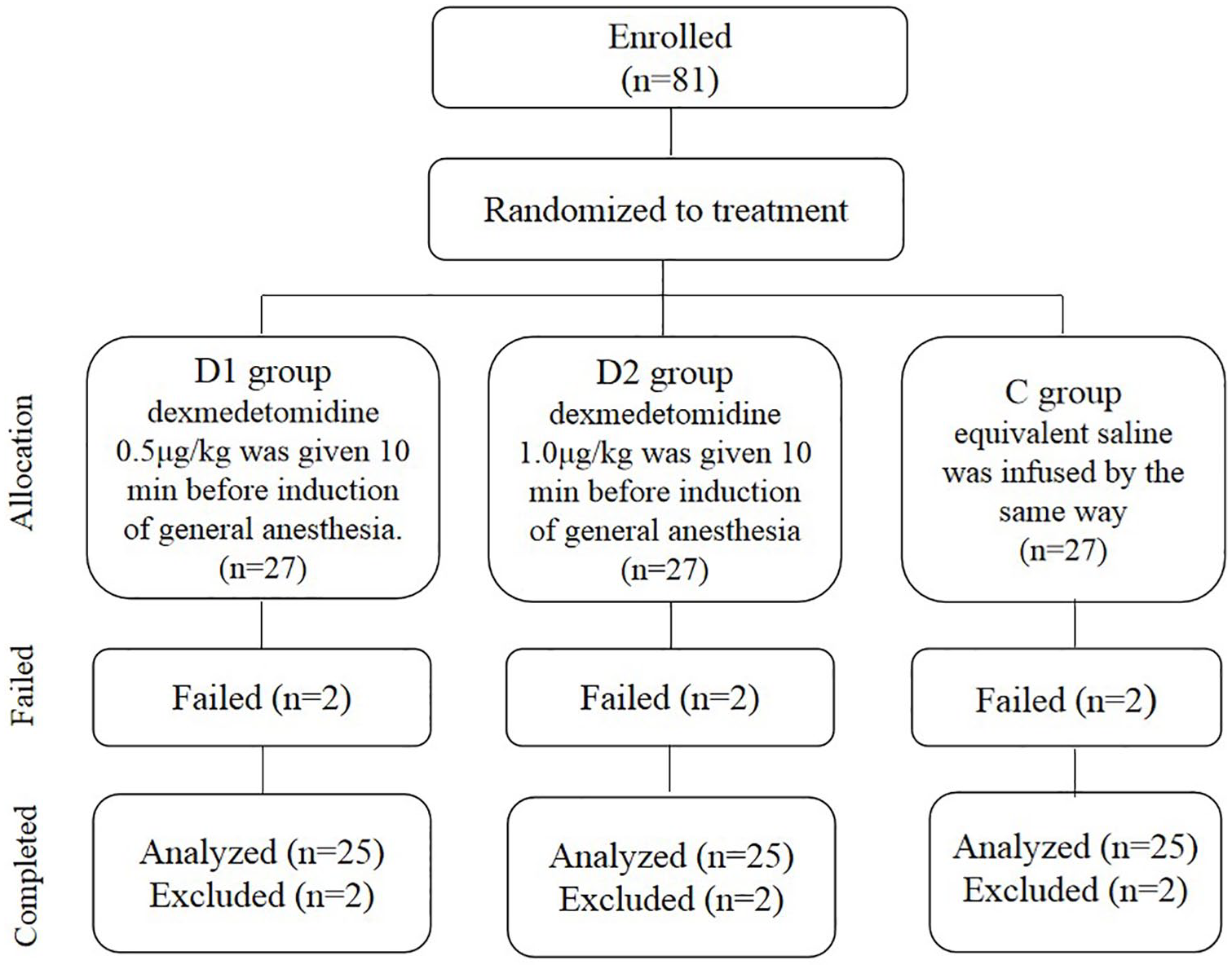
Consort diagram showing the flow of participants.
Patient characteristics.
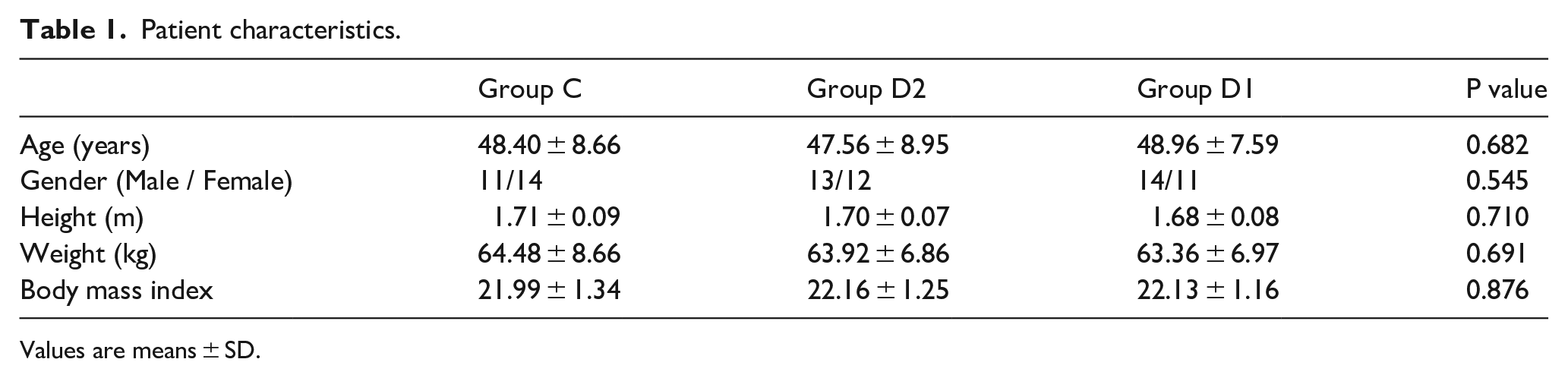
Values are means ± SD.

T0 and T25 times of three groups.
The Effect of DEX in non-depolarizing neuromuscular relaxant rocuronium
The changes of hemodynamics for MAP and HR were noteworthily different between DEX groups and control group after DEX administration (T2) and 10 min after trachea intubation (T4). However, at the other monitoring time points, such as before DEX administration (T1), before trachea intubation (T3) and 30 min after trachea intubation (T5), were no significantly differences among the three groups (p > 0.05) (Figures 3 and 4). The mixed regression model results indicated that each group had a decreasing trend in MAP. However, group D2 showed the lowest MAP during the process (p’s < 0.001) (Figure 3). Even considering the basic effect of HR among three groups, the HR in DEX groups were strikingly lower than control group (p < 0.001) (Figure 4). No side effects were in each group.

Mean arterial pressure of three groups at monitoring time points.

Mean heart rare of three groups at monitoring time points.
Discussion
DEX can prolong its duration of action of ROC in a dose-related manner
The work attempted to probe into the efficacy of two varying dosages of DEX on the onset time, as well as duration of neuromuscular blockade of ROC under the condition of sevoflurane anesthesia. In this study, T0 in three groups was found to be similar. Group D2 possessed longer duration of action for ROC than group D1 and group C. The difference was statistically significant. This result suggests that DEX does not have an impact on the onset time of ROC, but significantly prolongs its duration of action by the means of dose-dependence.
The effect of DEX in prolonging the duration of action in muscle relaxation of Vecuronium
The onset time of ROC is mainly affected by circulation or non-circulation factors, among which the circulation factors can affect the diffusion and distribution time of ROC from the injection area to other areas. However, the non-circulation factors are manifested in the interaction mechanism of neuromuscular diseases or the application of drugs. That’s why the study of Munoz etc. showed that the onset time of ROC could be shortened by adding small dose of ephedrine. 4 Studies have shown that after intravenous injection of DEX 1–2 μg/kg, blood pressure will temporarily increase and HR will temporarily decrease in healthy adults, and then blood pressure and heart rate return to normal, resulting in central anti-sympathetic effect and increased vagal activity. 5 Ozcan et al. 6 has shown that, compared with fentanyl and remifentanil, DEX can significantly prolong the duration of action in muscle relaxation of Vecuronium.
The discussion of DEX’s advantages and effects
DEX is regarded as a safe and effective adjuvant, or in single use therapeutic agent in clinical anesthesia, which has a broad clinical application promising in the further. 7 This study found that the first dose of DEX before induction had no effect on the onset time of ROC. It may be that after induction of ROC, the onset time of ROC decreases to a stage where blood pressure slowly falls from a short period of rise. 8 Although the heart rate decreases, the change of cardiac output is not obvious at this time. It has no direct effect on the speed of rocuronium reaching the neuromuscular junction and the volume of muscle perfusion. 9 Thus, the onset time was similar to that of the control group, which could provide theoretical evidences for clinical utility.
By inhibiting the secretion of norepinephrine and the activity of sympathetic nerve, DEX can reduce the sympathetic tension, strengthen the cardiac reflex of vagus nerve and baroreceptor reflex, reduce the secretion of catecholamine, reduce the operation center rate and blood pressure of patients, and reduce the blood supply of liver and kidney organs.10,11 However, rocuronium mainly depends on liver and kidney metabolism and excretion, so the decrease of liver and kidney blood flow may change the pharmacokinetics of rocuronium, prolong its half-life, and increase the muscle relaxation effect. 8 Therefore, the effect time of rocuronium in group D2 was significantly longer than that in the control group. Otherwise, DEX, as a preoperative drug, which is suitable for patients susceptible to pre- and perioperative pressure. Nevertheless, the use of DEX as a local anesthetic has not been widely used in clinics yet. 12 All above results showed that it is safe to inject DEX before induction of general anesthesia, and DEX is a dose-dependent in prolonging its clinical duration of action.
Another reason may be that although DEX has no neuromuscular blocking properties at the neuromuscular junction, research concluded that clonidine, another alpha-2 adrenergic receptor agonist, can abate the release of norepinephrine from sympathetic nerve endings and prevent the release of acetylcholine from the presynaptic membrane of the central nervous system, thereby enhancing the role of non-depolarizing muscle relaxants . 13 DEX, as a more selective alpha 2 adrenergic receptor agonist, may have similar effects, thus prolonging the clinical duration of rocuronium. 14 Therefore, we speculated that DEX’s high selectivity for alpha 2 receptors may be the prolongation mechanism for duration of neuromuscular blockade of ROC under the condition of sevoflurane anesthesia.
Due to the administration of DEX, the changes of HR and blood pressure in the two DEX groups were significantly different from those in control group C at T2 (after DEX administration) and T4 time point (10 min after trachea intubation). No significant differences were existed between three groups at the other monitoring time points. It may suggest that DEX can effectively improve the quality of tracheal intubation and maintain the stability of vital signs. DEX can inhibit the secretion of noradrenaline, decrease the plasma concentration of catecholamine, produce sedative and sympathetic inhibition effects, and reduce the stress response of patients to a certain extent. 15 Propofol and fentanyl can stimulate vagus nerve and dilate blood vessels, which leads to the decrease of blood pressure, while DEX can constrict blood vessels, thus to a certain extent counteracting the decrease of blood pressure in general anesthesia and maintaining the stability of hemodynamics.9,16 This is of great benefit to the life safety of patients during perioperative period.
The limitations in this study
However, there are still some limitations in this study. First, the duration of action for ROC was notedly extended in group D2, in which DEX 1.0 µg/kg was given 10 min prior to induction of general anesthesia. Secondly, one of the major limitations of this study was the small sample size. Randomized and controlled studies with a larger sample size will be conducted in the future. 17 However, there was no obvious effect in group D1, in which DEX 0.5 µg/kg was given in the same way. These results indicate that there is a dose-dependent effect, which needs further study. In addition, if we can further monitor the recovery time of muscle relaxation to 75%, it may help to determine the most appropriate time for extubation after operation, and also provide more clinical reference for the addition of muscle relaxants during long-term operation. In terms of hemodynamics, if we can monitor cardiac output or liver and kidney blood flow with the help of ultrasound, it may be more helpful to maintain the stability of perioperative circulation, and we can have a deeper understanding of the impact of DEX on the circulatory system.
Conclusion
In conclusion, DEX infusion in general anesthesia has no striking influence on the onset of ROC, but it can prolong its clinical effect time, which can provide reference for rational application of DEX and ROC in general anesthesia.
Footnotes
Other information
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The present study was approved by Shanghai Jiaotong University Affiliated Sixth People’s Hospital Ethics Committee [Shanghai, China; approval no. 2015-KY-007 (K)-(1)]. Written informed consent was provided by all patients.
Ethical approval
The present study was approved by Shanghai Jiaotong University Affiliated Sixth People’s Hospital Ethics Committee [Shanghai, China; approval no. 2015-KY-007 (K)-(1)]. Written informed consent was provided by all patients.
Informed consent
Verbal informed consent was obtained from legally authorized representatives before the study.
Trial registration
Registration number and name of trial registry are ChiCTR-IOD 17013079 and China Clinical Trial Registry, respectively.