
Abstract
Globally, surgical site infections are one of the common infections which lead to a large amount of mortality and morbidity in postsurgical care. The risk for surgical site infection is multidimensional which includes mainly; patient, surgery, and hospital-related factors. This study is aimed to determine the burden of SSIs along with contributed risk factors. A prospective observational cross-sectional study was conducted in one of the largest public-sector hospitals in Pakistan. A total of 412 patients were recruited in the study with full consent and monitored for 30 days after surgery with direct and indirect surveillance. Overall, in seven different surgical procedures the incidence (29.8%) rate of SSI was observed; in appendectomy (n = 17, 4.1%), exploratory laparotomy (n = 51, 12.6%), laparoscopic cholecystectomy (n = 12, 2.90%), mesh repair (n = 17, 4.01%), thyroidectomy (5, 1.2%), transurethral resection of the prostate (n = 11, 2.6%), and transurethral resection of the bladder (10, 2.4%). The average SSI rate in every single procedure was about 18 (4.27%) per surgical procedure out of 123 (29.85%) SSI cases. Types of SSI identified were superficial, deep incisional and organ/space (n = 76, 18.4%, n = 23, 5.5%, and n = 24, 5.7%). Incidence of SSIs during admission, at readmission, and post-surveillance cases were (n = 50, 12.1%, n = 25, 6.0% and n = 48, 11.6%). Associated risk factors found contributed to the incidence of SSI (p < 0.05). Pre-operative (n = 348, 84.5%) and 6 (1.5%) surgical patients did not received the post-operative antibiotics. The P. aeruginosa (n = 15, 12.1%) and S. aureus (13, 10.5%). Cefoperazone and sulbactam were the most prescribed antibiotics. Associated risk factors and treatment outcomes of surgical patients have a direct association with the incidence of SSI. Hospital-based antimicrobial stewardship, implementation of surgical guidelines, patient care, and education are needed to develop at wards level in hospitals.
Introduction
Globally, surgical infections contributed to a large burden of disease. LMICs (lower-middle-income countries) have many challenges in managing. 1 Likely, one of the great challenges is the increasing rate of antimicrobial resistance (AMR), probably linked to the misuse of antibiotics adds to challenge. Expansion of surveillance, prevention of infection, and antimicrobial stewardship programs are preliminary steps forward and have a role in the prevention of surgical infections. 1 Surgical site infections (SSIs) are common infections developed after surgery. Centers for Disease Control and Prevention (CDC) defined Surgical Site Infections (SSIs) as “infections that occur after surgery at the site of incision, organ, or space.” 2 The ECDC (European Centre for Disease Prevention and Control) postulates the same that SSI must happen within thirty days after surgery without implant. 3 Current findings by the WHO (World Health Organization) reported that SSI remains the second most common type of HAIs (Hospital-Acquired Infections) in the United States and Europe that is linked with increased length of stay at hospitals. 4 Additionally, in the US alone during the period from 2006 to 2009, nearly 1.9% of surgical operations were affected by SSIs. 5
The rate of SSI is higher in the developing world than that in developed countries. The post-discharge surveillance of SSI in elective clean and clean-contaminated surgical procedures was carried out during 2019 and 15% incidence was reported in LMICs. 6 The prevalence of HAIs was lower in 2015 than in 2011 after continuation to make improvements in the prevention of such infections, as per strategies increased by CDC. 5 HAIs may affect approximately 5% to 20% of patients during hospitalization. It is estimated that in Europe, about 7.5 million patients (acute hospitals 3.5, 4.2 million in the tertiary care facilities) develop HAIs every year. Nearly 147,000 patients in European hospitals die annually from HAIs, directly or indirectly, with SSIs at the forefront. 7 A 2002 Canadian study reported a 4.25% incidence rate of wound infection after cardiac surgery approximately 29,000 patients.8,9 The incidence of SSIs is four times higher in LMIC. 10 The SSIs accounted for approximately 31% of all HAIs and up to 20% of post-surgical readmissions. 10
Recently, a study reported from Pakistan showed that in older patients, 4 out of 9 developed SSIs, and those who underwent emergency surgeries were the most affected. 11 Pakistan is the seventh most populated country in the world with a population of 212.2 million. Pakistan established its first National Infection Guidelines in 2006. 12 WHO has developed evidence-based guidelines and recommendations for the prevention of SSI.13,14 Implementation of these guidelines and further modification is a challenge in Pakistan. 15 Most of the health care setups have no institutional guidelines or SOPs to follow. 16 No detailed data is available on SSIs from Pakistan and few pilot studies are documented which are totally against WHO criteria in a region. Inappropriate choice, the timing of administration, and the combination of SAP observed in Pakistan. 17
Factors associated with an increased risk of SSI include; emergency procedures and longer duration of surgery. 18 Numerous risk factors are involved in SSI with a complex relationship as; surgery, patients, microbial, and environment-related factors. 18 The incidence rate of SSIs mainly depends upon the health care facility, surgical procedure, and level of care. Patients of SSIs are closely linked with increased length of stay, delayed wound healing, pain, discomfort, long-lasting disability, and even death. 19 Single-incision Laparoscopic Surgery (SILS) is technically feasible and safe for patients undergoing colorectal surgery with no unusual complications. 20
Clinicians should limit the use of quinolones and remain aware of the possibility of resistance developing by colistin. 21 Surgeons’ perspective has shown that the associated risk factors and treatment outcomes of surgical patients may have a direct association with the incidence of SSIs. 22 Antibiotic prophylaxis is one of the major domains to prevent and reduce the rate of surgical site infections. Mainly antimicrobial stewardship (AMS) programs are also focused on an audit of surgical prophylaxis. 23 The current study is aimed to examine the incidence rate of surgical site infection along with risk factors responsible.
Methods
Study design and setting
A cross-sectional study was carried out in the general surgical wards. The current study was conducted in 92-bed general surgery wards of PIMS (Pakistan Institute of Medical Sciences), a 592-bed tertiary care teaching hospital associated with Shaheed Zulfiqar Ali Bhutto Medical University (SZABMU). PIMS hospital is one of the largest hospitals in the country, located in the capital, Islamabad.
The United States CDC (Center for disease control and Prevention) surveillance methods were used. 24 Trained assistants (two nurses and two pharmacists) collected indirect surveillance data from patient medical records through validated data collection forms. Research study assistants also investigated all surgical sites during wound dressing and changing 24 to 48 h after the surgical procedure (direct surveillance). Swabs of suspected SSIs were taken and sent for analysis by assistants, along with post-discharge surveillance. For the post-discharge surveillance, patients were asked to come back for follow up after 30 days. If this did not happen consented patients were contacted through mobile phone numbers and if SSIs were suspected, patients were then asked to visit the same hospital to possibly confirm the diagnosis. The National Health Safety Network CDC criteria were used for the SSI diagnosis. 24 Patient’s medical records, antibiotics prescriptions were collected and presented in the shape of drug utilization.
Sample size, study participants, and patients characteristics
The sample size was determined through Ra-osoftTM calculator with the confidence interval 95%, a margin of error 5%, and the assumption of 80% an adherence rate. This created a sample size requirement of 385. Attrition rate assumed at about 20% and the existence of outliers, a sample of 412 respondents was needed to be included in the present study.
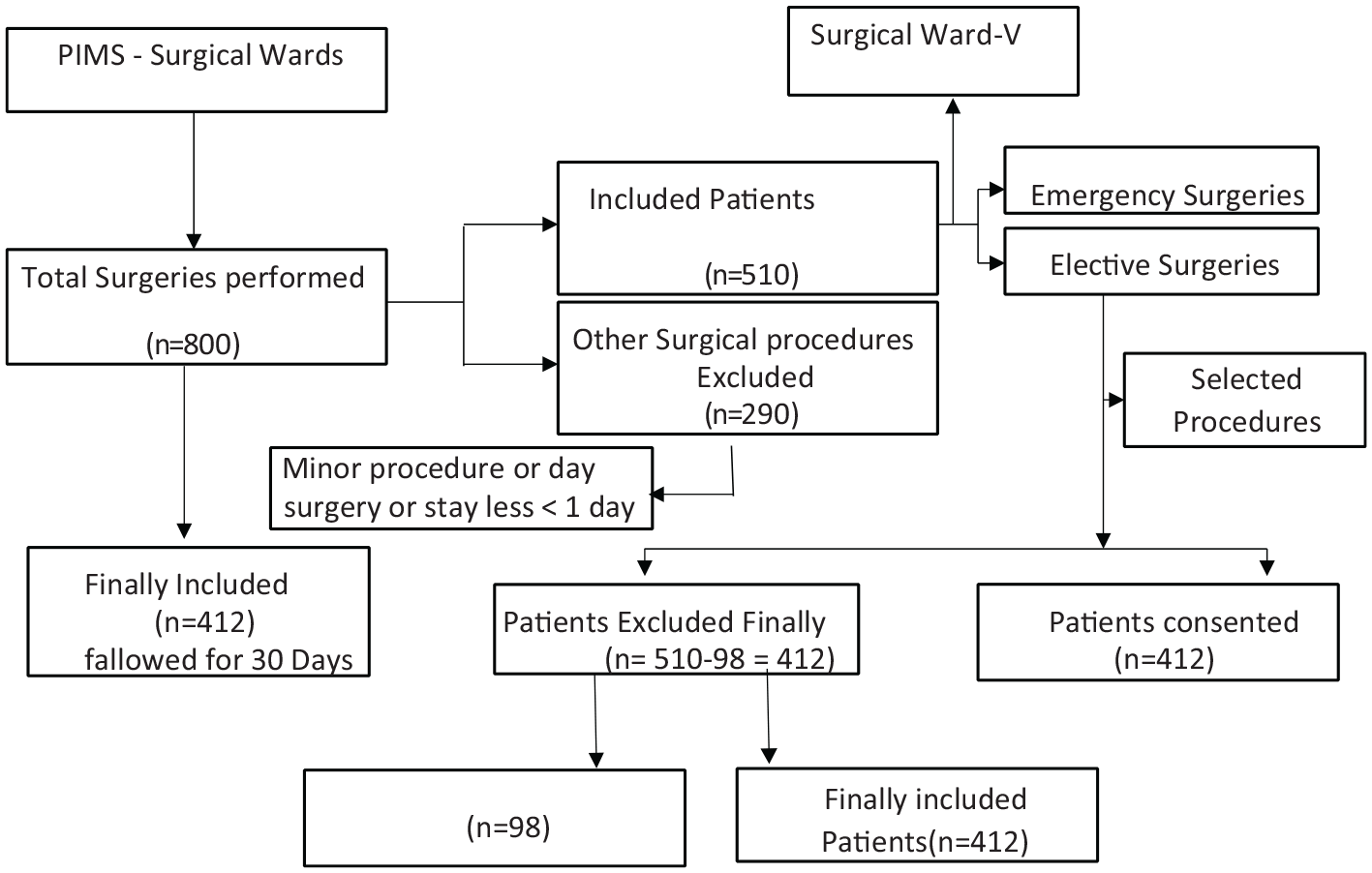
All patients admitted between November 2016 and August 2017 were prospectively included in the survey. All non-surgical patients were excluded from the study. A total of 800 patients were admitted to the given surgical wards. Among (n = 800) patients, 510 patients were admitted for selected surgeries (Elective and Emergency) and the remaining excluded (n = 290) were observed as minor or for day surgery. A total of 510 patients, 98 participants (n = 50) didn’t give consent after the surgery, and (n = 48) failed to answer the questions during surveillance and or did not attend the call during follow-up were excluded (Schematic/Flow Chart 1). Finally, 412 (80.7%) patients were recruited in the study after full consent.
Sampling techniques and laboratory method
Collected swabs samples were plated on the medium of blood and MacConkey agar. For the identification of pathogenic bacteria, standard and conventional methods were used. 25 Antibiotics susceptibility testing was done through the Kirby-Bauer disc-diffusion method on Mueller-Hinton agar plates. The Disc strength was according to the recommendation of CLSI (Clinical Laboratory Standard Institute). CLSI interpretation criteria were used for the susceptibility and resistance. Gram-negative bacteria intermediate susceptible isolates were considered resistant in the calculations. Staphylococcus aureus isolates, the screening of methicillin resistance was done by cefoxitin. According to the CLSI guidelines, a disc screen test and 6 g/ml oxacillin in Mueller-Hinton agar added with NaCl (4% w/v; 0.68 mol/l). 25
Data collection
A literature survey was done with (MeSH) keywords before the questionnaire development and different questionnaires were reviewed concerning incidence, factors responsible for the SSIs, along with antibiotics rationality. Finally, a comprehensive data collection form was developed that included (a) general identification and patient information, (b) demographics and socio-demographics (gender, age, education, financial status, residence, occupation, and marital status) (c) patient diagnosis-related, (d) surgery-related, (e) pre and post-operative antibiotics, (f) hospital facilities related factors, (g) KUNIN and MUST criteria. The data collection form was first validated from the research committee of the pharmacy department and two experts from the other academic institutes validated the data collection forms through the face and content validity (Supplemental File S1). The hospital review research committee alongside the ethical review board also approved the final validity of the data collection forms and approve the data collection commencement (Schematic/Flow Chart 1).
Ethical approval
Ethical approval was obtained from the Quaid-i-Azam University Bio-Ethical Committee with assigned protocol number BEC-FBS-QAU-103, the PIMS Hospital Ethical Review Board reference number 1-1/2105/ERB/ SZABMU also ap-proved the study.
Statistical analysis
The Data were analyzed through IBM SPSS Statistics version 22 (IBM, Armonk, NY, USA). Percentages and frequencies were determined for categorical and binary variables. Descriptive analysis and SSI cumulative incidence rates were calculated through different statistical techniques. The associations between variables were explored through the Pearson ϰ 2 test. A regression model was used for the association of SSIs with other factors. Simple linear regression was used to recognize the factors affecting and leading to the incidence of SSI. Multiple linear regression analysis was conducted to variables have the statistical significance of the univariate analysis to separate the factors (independent). For each predictor related to patients, surgery, and guidelines beta (standard error and p-value) were reported. Information about the percentage of variance explained included to provide by the model through pseudo R 2 value. Less than 0.05 (p-value) was considered to be statistically significant. 26
Results
Patients demographics
A total of 800 patients were registered for different surgical procedures, out of a total of 510 patients went through general surgeries, and finally, 412 patients were recruited on a purely informed consent basis (Schematic/Flow Chart 1). Overall, n = 232 (56.3%) male and n = 180 (43.7%) were females. Education level, no formal education 40%, or only have primary education 16.2%. Participants belong to rural areas (n = 250, 60.7%). Patients reported with age group between 28 to 37 years (n = 97, 23.5%) mostly went through the surgical procedure. Patients demographics and their relationship with SSI found significant in gender and education level (Table 1). Most of the participants were males and the results showed near to significant relation (p = 0.08) with SSI. Education level was found significantly associated with SSIs (p = 0.02). SSIs were most commonly reported in housewives (n = 45, 30%), and (n = 174, 42.2%) patients belonging to middle-class background. The socioeconomics values were adjusted into USD as reported previously; In approximately USD: VL = very low (>$60.0), and upper class = (>$500). 27 (Table 1).
Demographics of the participants and association with the incidence of SSI.
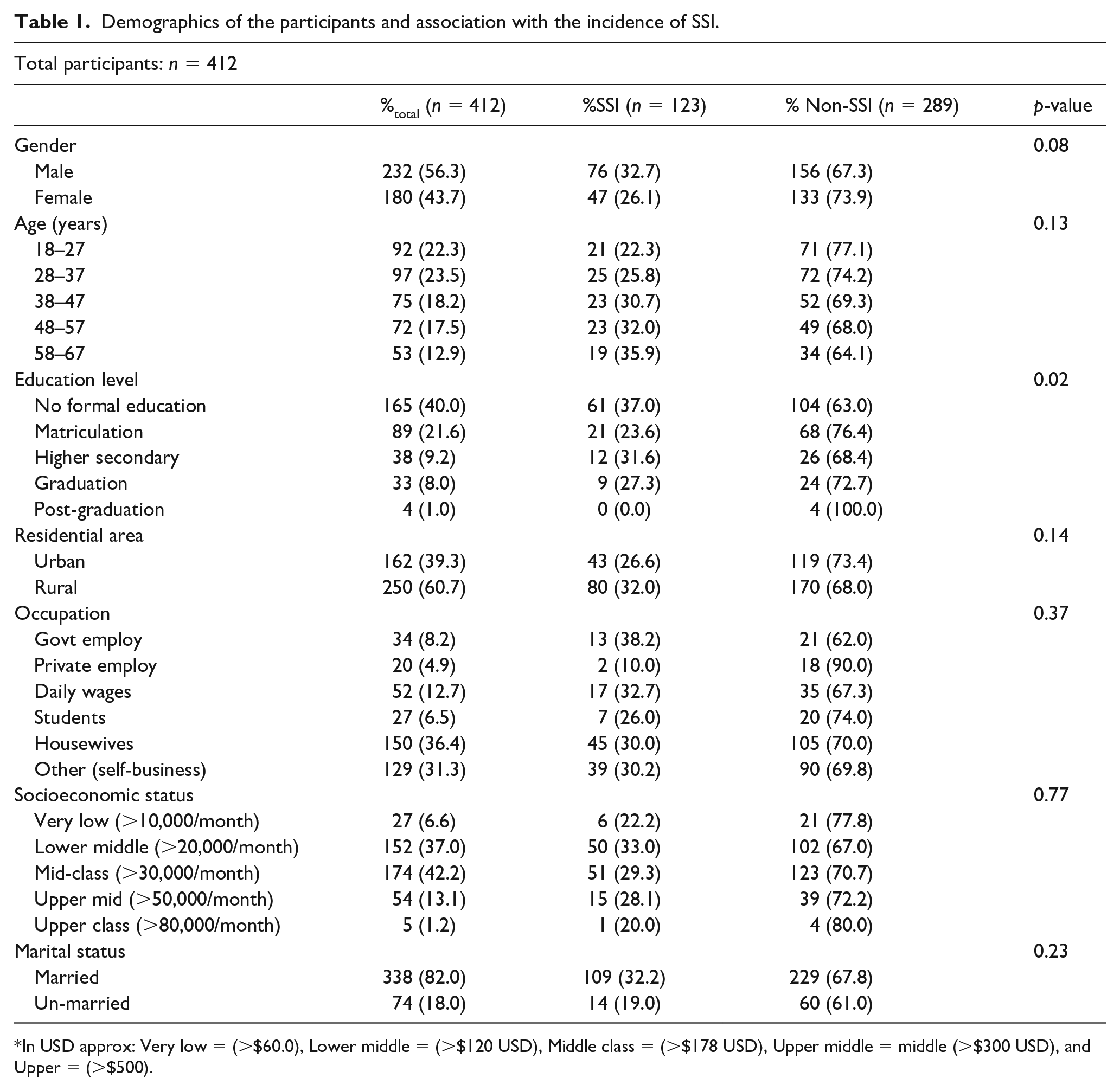
In USD approx: Very low = (>$60.0), Lower middle = (>$120 USD), Middle class = (>$178 USD), Upper middle = middle (>$300 USD), and Upper = (>$500).
Burden: Incidence of SSIs
Overall, out of 412 patients, 123 (29.85%) have developed SSIs and observed in seven different surgical procedures include; appendectomy (n = 17, 4.1%), exploratory laparotomy (n = 51, 12.3%), laparoscopic cholecystectomy (n = 12, 2.9%), mesh repair (n = 17, 4.1%), thyroidectomy (5, 1.2%), TURP-transurethral resection of the prostate (n = 11, 2.6%), and TURB-transurethral resection of the bladder (10, 2.4%). The average SSI rate in every single procedure was about 18 (4.27%) out of 123 (29.85). Types of SSI identified were superficial, deep incisional and organ/space (n = 76, 18.4%, n = 23, 5.5%, and n = 24, 5.7%). Incidence of SSIs during admission, at readmission, and post-surveillance cases were (n = 50, 12.1%, n = 25, 6.0% and n = 48, 11.6%). (Table 2). Most SSI cases (40.6%) were detected during the hospital stay after surgery. The culture sensitivity test was performed only for 64.2% of cases during the stay at the hospital. Nearly 52% of SSI cases, the causative pathogen was identified. Only 6.50% of a patient suffering from SSI underwent a second surgery. Overall 79% SSIs cases were reported in ASA score-I, 28.4% cases in score-II, and 7.3% cases were in score-III.
Incidence of surgical site infections.

Associated risk factors
Patients related factors
Various patients related factors associated with SSIs were identified and are shown in Table 3. Elevated ranges of blood pressure and albumin level were significantly (95% CI: p = 0.05, p = 0.02) associated with SSIs. Patients who had past surgical histories showed a significant (p = 0.02) relation with SSIs. About (n = 47, 37.2%) patients suffered from SSI had a surgical history. Table 3 also shows the addiction to smoking and other tobacco products. The results confirmed a strong significant association of smoking and other tobacco products use with the incidence of SSIs (p = 0.01, p = 0.05) respectively. The influencing factors related to patients like patients’ medical and past surgical history affect the incidence of SSI (Supplemental File S2).
Patients related factors association with surgical site infections.
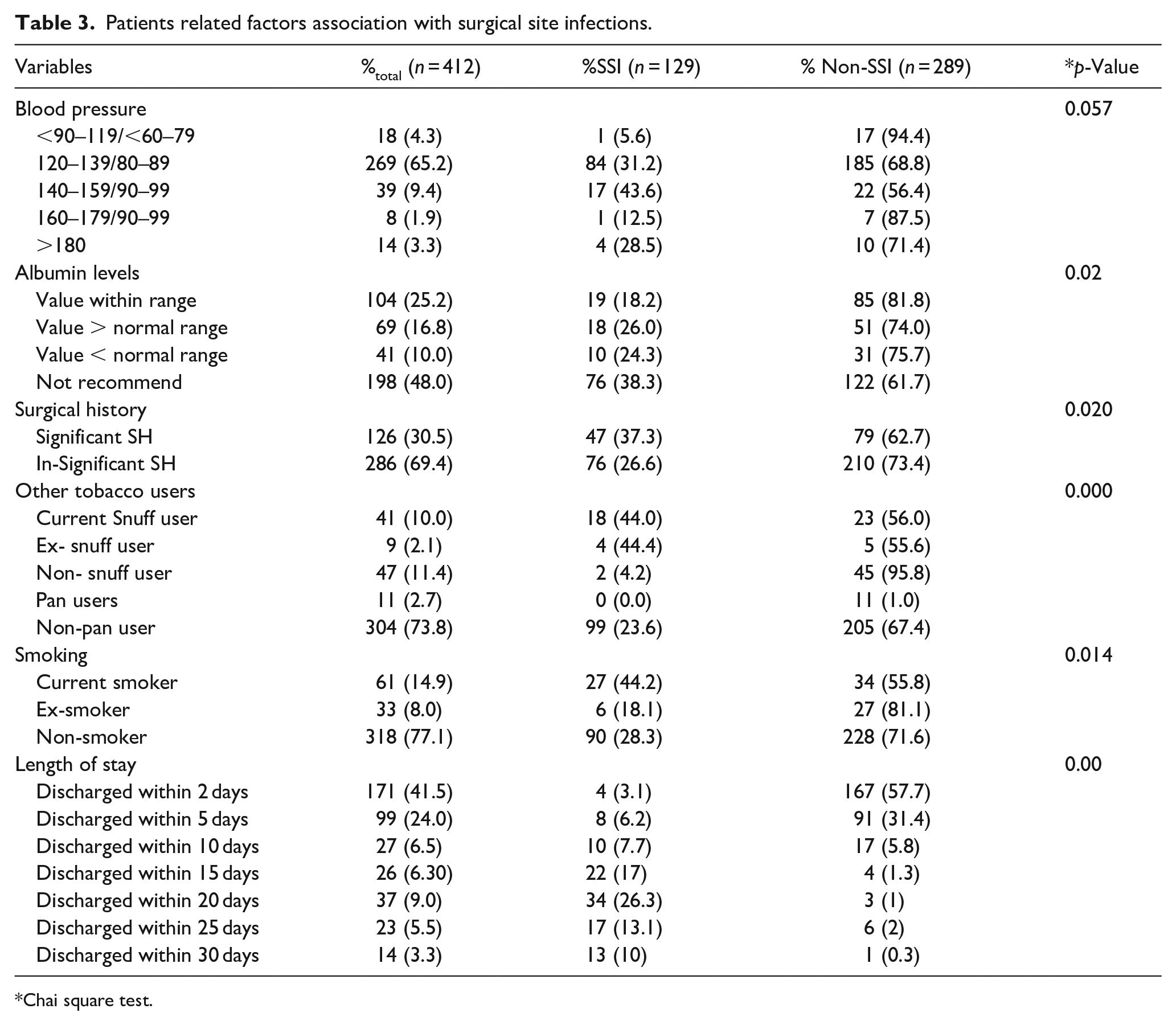
Chai square test.
Surgery-related factors
Surgical procedures were linked with the incidence of SSIs (p = 0.01). Exploratory laparotomy (XLAP) was the most commonly reported surgical procedure with cases of SSIs (n = 125, 30.3%). Laparoscopic cholecystectomy (CHOL) was in second place (14.1%). Pathological lab tests before and after surgery and surgical trauma after surgery (p = 0.01, p = 0.00) were significantly associated with SSI. Surgery-related factors and association with SSI were remained significant (Table 4). Significance relation (p = 0.00) was assessed between duration (from greater than 30 min to 3 h) of surgery and SSI incidence (Supplemental File S3).
Association of surgery related factors with surgical site infections.

UB: urinary bladder related surgeries; PT: prostate related surgeries.
Hospital related factors
Length of stay at hospital (LOS)
Prolonged hospitalization is directly associated (p > .05) with the incidence of surgical site infection. The post-operative LOS of patients at hospital and number of patients suffered from SSI <5 days (n = 4), >5 days (n = 8), >10 days (n = 10), >15 days (n = 22), >20 days (n = 34), >25 days (n = 17), 30 days (n = 13), and the patients with critical threat to life (n = 15). These patients were followed during their hospitalization.
Hospital facilities for the individual patient
The hospital facilities provided to every single patient was observed in terms of poor, fair, good, and very good category. Various hospital facilities related factors found a significant association with the incidence of SSI. Ventilation, hygienic condition, bed dressing, diet plan, availability of waste bins, and biosafety signs (p = 0.00, p = 0.001, p = 0.04, p = 0.043, and p = 0.27) have a strong association with incidence of SSI. The surgical site dressing was found to have an insignificant association (p = 0.5). The majority of the patients had developed SSI with poor facilities and care during the stay at the hospital.
Guidelines used and incidence of SSIs
Different guidelines were used which are still ignored at surgical wards and hospitals. The CDC guidelines were used for the classification of surgical wounds and observed significant results (p < 0.05), which means CDC guidelines are still ignored and unfollowed for appropriate wound classification shown. The prescribed antibiotics rationality was checked through KUNIN criteria and irrationality was observed in the prescription as the KUNIN criteria were associated significantly with SSIs (p < 0.05). The MUST (malnutrition universal screening tool) was used for surgical patients and significant association with SSIs was found (p < 0. 05). ASA (American Society of anesthesiologists) score was used for the physical status of the patient and mostly the patients were physically fit and the ASA association with SSIs was insignificant (p > 0.05). (Supplemental File S4).
After adjusting contributory factors of SSI incidence, the univariate analysis consists; patient-related factors (BP, albumin level, surgical history, and length of stay), surgery-related factors (nature of the surgery, surgical procedures, length of surgical procedures), and related guidelines (KUNIN, MUST, CDC). Antibiotics prophylaxis included pre- and post-operative along with the total duration of antibiotics. The model fit statistics summary (R 2 =0.615) and the significant association was found (p > 0.05). (Table 5).
Model summary.

Model summary: R 2 = 0.615 p = <0.05, P-value less than 0.05 is considered significant.
Antibiotics prescribed
Antibiotics were prescribed to the patients before (pre-operative), intra-operative (before 60 min of operation) and post-operative (after the completion of surgical procedures). Pre-operative antibiotics prescribed included cefoperazone and amikacin (n = 30, 7.3%), Ceftriaxone (15, 3.6%), amoxicillin (n = 4, 1%), piperacillin and tazobactam (n = 2, 0.5%), Cefotaxime (n = 9, 2.2%), and vancomycin (n = 4, 1%). Patients (n = 348, 84.5%) did not receive pre-operative antibiotics. Intra-operative antibiotics included; cefoperazone and amikacin (n = 83, 20.2%), Ceftriaxone (32, 7.8%), amoxicillin (n = 16, 3.9%), piperacillin and tazobactam (n = 7, 1.7%), Cefotaxime (n = 17, 4.1%), and vancomycin (n = 8, 1.9%). Patients (n = 249, 60.4%) did not receive antibiotics 60 min before operations After surgery, patients received antibiotics; cefoperazone and amikacin (n = 191, 46.4%), Ceftriaxone (80, 19.4%), amoxicillin (n = 42, 10.2%) piperacillin and tazobactam (n = 29, 7.6%), Cefotaxime (n = 52, 12.6%), and vancomycin (n = 12, 2.9%). Only 6 (1.5%) patients did not get post-operative antibiotics.
Overall, more than 83% did not receive antibiotics prophylaxis before the surgical procedure. Cefoperazone and sulbactam were the most prescribed antibiotics pre and post-operatively. The combination of cefoperazone and sulbactam along with amikacin was also used in pre and post-surgical patients. Prescribed antibiotics before and after the surgical procedures have differences (Table 6). No specific rational guidelines were in practice and the prescribed antibiotics were measured with the KUNIN criteria. Most patients received irrational and inappropriate therapy before and after surgery.
Antibiotics prescribed for surgical patients.

Causative agents
The culture sensitivity test was performed in only 79 infected patients (65 positive and 14 with negatives results) out of 123. Various causative agents were reported in positive cases and that was responsible for the development of SSIs. The most common pathogens involved in SSI were Pseudomonas aeruginosa (12.1%), Staphylococcus aureus (10.5%), and K. pneumonia (8.1%) and E. coli (4%). Table 7 shows the microorganisms responsible for the incidence of surgical site infections.
Causative agents.

Discussion
The present study is the first of its kind to report the SSI rate in seven different surgical (emergency and elective) procedures in the largest tertiary care hospital in the capital of Pakistan. Multifactorial risk factors were associated with the incidence of SSI. Different strategies need to curb the incidence of SSI in Pakistani hospitals. The present results may relate to other LMICs. The overall incidence rate was found 29.85% in seven different general surgical (elective and emergency) procedures. The average rate of SSI (n = 123, 29.8%) was 4.3% of the total cases. The study published in 2011 from Pakistan reported 82 patients developed SSI and 13% experience in emergency general surgical procedures. 28 The current study showed 129 patients developed SSI (58 elective and 65 emergencies) in general surgical wards. The SSIs rate in India ranges from 5% to 12.7% in major cities. An Iranian study reported 17.4% and another from Egypt reported 17%. A Study in Pakistan showed a 12.7% SSIs rate in emergency cases and 4.6% SSIs rate in elective surgical cases but the sample size was limited. 29 In another study, a 5.78% to 17.5% SSIs incidence rate was reported. 30 In the Sindh province of Pakistan, at SSIs rate was up to 7.7% in Karachi and 13% in Hyderabad. 31 The SSI incidence rate in the thyroidectomy was reported by 10.9% in Nawabsha city. 32 Due to post-surgical complications, the mortality rate was up to 10.6% in Karachi. The Khyber Pakhtunkhwa province hospitals reported SSIs rate from 5.78% to 9.2%. 33 Punjab province reported an SSI rate of 5.78% to 17.5% but it was mostly in single surgical procedures. 34 The total length of stay at the hospital has a significant influence on the incidence of SSIs. Pre-operative stay is linked with SSIs reported in previous studies. A single dose of ceftriaxone reported with the high rate of SSIs, but 24 h regimen (9.6% vs 6.7%) has opposite results reported with the low incidence rate of SSIs. 35
Associated risk factors have the potential to increase the chance of SSI. Current research shows the risk factors have potential toward the incidence of SSI. Patients, surgery, and hospitals related factors were checked against the incidence of SSI and found significant results (p < 0.05). Due to different risk factors the rate of SSIs higher than previous studies as Bibi et al. was the first who reported the SSI incidence rate with many limitations. These high rates, especially in the emergency surgeries, could be; due to lack of infrastructure, human resources, contaminated water, poor sanitation, overcrowding, and often a general disinterest in basic infection control by health care staff. 15 A study reported from Malaysia, during 1-January 2016 and 31-December 2017 stated, associated risk factors were responsible for deep SSI. 36 Based on a large population analysis, previously reported risk factors for SSI were confirmed in this study following surgery; including preoperative and postoperative albumin, level and decreased postoperative hemoglobin, and the same factors are identified in the current study. It was also noted regarding ASA scores that 79% of patients fall in the score I and 28.4% in Score II. Malnutrition risk assessment for surgical patients is not in practice. Pre and post antimicrobial prophylaxis patterns are not on a standard to rationality like set criteria of KUNIN. Implementation of these guidelines may reduce the incidence rate of SSI. The above-mentioned guidelines are still ignored in the given hospital, most patient wounds classification was allotted on a general empiric basis.
The Lancet Commission on Global Surgery projected that about 5 billion people lack access to safe and reasonable surgical care. 37 Worldwide burden of SSIs, the several gaps in evidence-based guidelines, and essential for a global approach, for the prevention of SSIs WHO decided to prioritize the development of evidence-based commendations. 13 Total 13 recommendations on preoperative preventive measures were presented and these guidelines take into account the benefits and harm balance, the evidence quality, patient values and preferences, cost, and resource use implications.13,14 Later on WHO presented 16 recommendations for SSIs prevention. 14 Appropriate surgical antibiotics prophylaxis (SAP) may reduce the risk of SSI but proper guidelines are needed to follow for the individual procedure. Recently, Khan et al., study reported the poor adherence to the pre-operative antibiotics guidelines and in another study by Khan et al., stated that the most common antibiotics cefuroxime and ceftriaxone were used inappropriately. 38 Our study also reported that no adherence to SAP was found during pre- and post-surgical prophylaxis. We also recommend educational interventions along with the implementation of AMS programs.39,40 The above authors also reported that approximately 89% of the patients who underwent surgical operations received antibiotics. 41 The same results were found in our study as only six patients didn’t receive antibiotics after surgery. The selection of a therapeutic agent, the timing, and the use of broad-spectrum antimicrobial were the common problems in the given setting.23,38,41
Besides the strength the given study has many limitations; firstly, the study has been taken in one tertiary care hospital so the findings may not generalizable to the whole country. The total period of the study and the sample size is not that much larger. The given study was conducted in general surgical wards only.
Global strategies and solutions are required as surgical infections constitute a worldwide problem. This consists of improving tools and techniques for source control, surveillance programs, and as well as antibiotic-stewardship, infection control, and practices of prevention to control AMR. 37 The combined efforts will lead to a decrease in the incidence of SSI.
Conclusion
To the best of the author’s knowledge, the current surveillance study is the first of its kind in Pakistan. The current research tried to show the reasons behind the occurrence of SSI events and gave an overall scenario of the SSIs. Associated risk factors and treatment outcomes have a direct association with the incidence of SSI. This is an alarming situation in Pakistan and still, no proper SSI reporting system with central databases exists. Evidence-based guidelines implementation at the hospital is the need of an hour. The hospital-based antimicrobial stewardship programs are need of the hour to curb SSIs. Moreover, further studies at the national level are required.
Supplemental Material
S1-Data_collection_form.miR – Supplemental material for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan
Supplemental material, S1-Data_collection_form.miR for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan by Faiz Ullah Khan, Yu Fang, Zakir Khan, Farman Ullah Khan, Zafar Iqbal Malik, Naveed Ahmed, Amir Hayat Khan and Asim.ur. Rehman in European Journal of Inflammation
Supplemental Material
S2-Patient-Related_Factors_MR – Supplemental material for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan
Supplemental material, S2-Patient-Related_Factors_MR for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan by Faiz Ullah Khan, Yu Fang, Zakir Khan, Farman Ullah Khan, Zafar Iqbal Malik, Naveed Ahmed, Amir Hayat Khan and Asim.ur. Rehman in European Journal of Inflammation
Supplemental Material
S3-Surgery-Related_Factors_miR – Supplemental material for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan
Supplemental material, S3-Surgery-Related_Factors_miR for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan by Faiz Ullah Khan, Yu Fang, Zakir Khan, Farman Ullah Khan, Zafar Iqbal Malik, Naveed Ahmed, Amir Hayat Khan and Asim.ur. Rehman in European Journal of Inflammation
Supplemental Material
S4-Related_Guidelines_miR – Supplemental material for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan
Supplemental material, S4-Related_Guidelines_miR for Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan by Faiz Ullah Khan, Yu Fang, Zakir Khan, Farman Ullah Khan, Zafar Iqbal Malik, Naveed Ahmed, Amir Hayat Khan and Asim.ur. Rehman in European Journal of Inflammation
Footnotes
Acknowledgements
We (authors) highly appreciate the support of the given hospital, university, and all who helped us for the present research.
Authors contribution
Conceptualization, A.R. Data curation, F.U.K. Formal analysis, Z.K., F.U.K. Methodology, N.A., A.R. Project administration Z.I.M., A.R. Supervision, A.R. Writing validation, A.H.K. Review and editing, Y.F. The final manuscript read and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the; Quaid-i-Azam University Bio-Ethical Committee has provided the ethical approval before the execution of the study and have assigned protocol number BEC-FBS-QAU-103, and PIMS (Pakistan Institute of Medical Sciences) Hospital Ethical Review Board granted ethical approval with reference number 1-1/2105/ERB/ SZABMU.
Informed consent
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.