
Abstract
Hepatitis C is a dangerous liver disease transmitted by Hepatitis C virus (HCV). HCV constitutes an important health issue in Pakistan. In Pakistani setting HCV is found frequently and is recognized as an alarming health problem. In this cross sectional study we reviewed published data regarding the seroprevalence of hepatitis C in general community, blood donors and pregnant females and risk factors linked with its occurrence in Pakistan. Data retrieved from163 studies published from 2001 to 2022 was utilized and weighted mean was calculated. Data of 1,875,232 individuals was collected and arranged into three groups, depending upon the population type such as (1) general population, (2) pregnant women, (3) blood donors. General population (765,426) and blood donors (973,260) formed the most of population. Mean Hepatitis C virus prevalence in general public and blood donors was 16.47% and 8.2% respectively. In pregnant females (136,546) the mean frequency was 9.3%. This study exhibits that the frequency of Hepatitis C in general population, pregnant females and blood donors groups was 11.32%. The data suggested that risks factors for transmitting HCV infection in Pakistan include unsterilized needle use, blood transfusions, shaving by barbers, lack of trained staff, needle stick injuries, injection drug users, household contacts/spousal transmission, unsterilized dental and surgical Instruments, improper disposal of hospital waste, poor infra-structure and others. The frequency of HCV infection is distressing in Pakistan. Health education and awareness programs are needed for decreasing Hepatitis C infection in Pakistan. The data necessitate the implementation of preventive and remedial approaches to decrease the disease load and mortality in Pakistan.
Introduction
Hepatitis C virus (HCV) is widespread globally and a considerable load is exerted by this microorganisms in health care systems. 1 HCV is a common causal factor of chronic hepatic disorders, belongs to Flaviviridae family. Death rate due to this virus is high, approximately 350,000 persons die annually. 2 Over 58 million persons are chronically infected with HCV around the globe3,4 around 1.5 million persons worldwide are recently infected with Hepatitis C. 5 The frequency of Hepatitis in general community was assessed at 1.0%. 6
Infected blood products, unsafe sexual relations, infected barber instruments, tattooing and body fluids are mainly attributed to the transmission of HCV. 7 HCV is the main causative factor associated with hepatocellular carcinomas (HCC). HCC is a prevalent tumor and a major cause of cancer associated deaths across the globe.7,8 When these diseases are escorted by inflammation, damaging of hepatocytes activate the reproduction and fibrosis, that eventually can cause HCC and liver cirrhosis. 9
Seroprevalence is the percentage of persons in a community which shows antibodies against a specific pathogen in their blood. Seroprevalence shows the number of persons infected with the specific pathogen (HCV), while viremic prevalence is the proportion of persons suffering from chronic hepatitis C among infected persons. 10 HCV is very indigenous in many areas of Pakistan. The precise frequency of hepatitis C is not known uptil now. Different literature showed that 4.8% community is suffering from hepatitis C.2,11 Epidemiological understanding is important in the development of economical medication against hepatitis C. 12
In various regions of Pakistan, various research works has been carried out in past, but a compile sero-epidemiological data describing HCV prevalence is lacking. The current study revealed a picture of frequency of hepatitis C infection in Pakistan and drew a comparision attainable with published data regarding hepatitis C among different cities of Pakistan. The current review was carried out to analyze the frequency, causal factors, routes of transmission and distribution of hepatitis C genotypes in different areas of Pakistan.
Literature review
Literature was taken from google scholar, science direct and pubmd. Data regarding prevalence and casual factors in Pakistani community was taken. Incomplete researches were not included. We chose 163 numerous research papers from various search gates. Research reported between 2001–2022 was incorporated in the present review
Analysis
Frequency of hepatitis C in general community.

Frequency of hepatitis C in pregnant females.

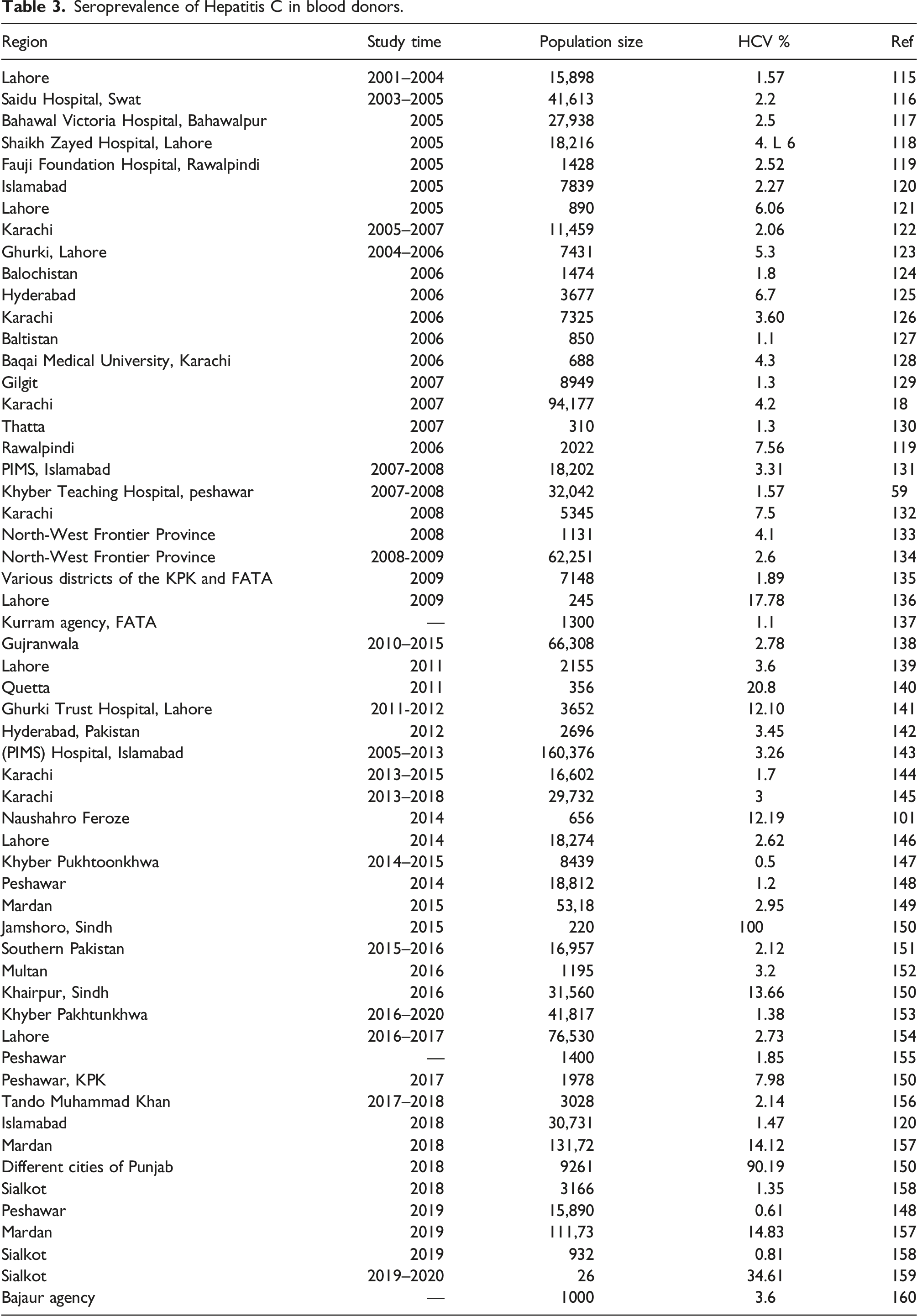
Seroprevalence of Hepatitis C in blood donors.
This equation was utilized for determining the weighted mean and the outcomes shows new percentage frequency in each category. Accordingly, the overall frequency was also determined.
Hepatitis C virus prevalence in various groups
Data was collected from 163 published studies and arranged into three groups, depending upon the population type such as (1) general population, (2) pregnant women, (3) blood donors.
General population
General population constituted the largest population data. Seventy five studies pertained to the Hepatitis C seroprevalence in general community (Table 1). Data published during 2003–2021 was taken. In this group the data of 765,426 individual was included. Studies were included from the four provines Punjab, Sindh, NWFP and Balochistan. The prevalence of hepatitis C was ranged from 1.7% in DI Khan to 91% in Swat. The mean prevalence was 16.47%.
Pregnant women
Thirty one studies describing the seroprevalence of HCV infection in 136,546 pregnant females were reported (Table 2). These studies covered 16 years from 2005 to 2021. The seroprevalence in the pregnant women ranged from 0.6%–35.34%. Overall seroprevalence was 9.3%. Twenty two studies showed prevalence >5%.
Blood donors
There were 57 studies in the blood donor’s group. In this group the population covered was 973,260. Data published during 2001–2021 was taken, spanned 20 year’s period (Table 3). Studies were included from all provinces of the country. The frequency of HCV infection ranged from 0.5 to 100% in Khyber Pukhtoonkhwa and Jamshoro, Sindh respectively. The mean prevalence was 8.20%. Only nine studies exhibited a prevalence greater than 10%.
Risk factors for transmitting hepatitis C in Pakistan
Among liver related diseases hepatitis C is the most common cause and HCV results in hepatocellular carcinoma which is a major cause of mortality and morbidity worldwide. 161 HCV is RNA virus, single stranded and it is related to flaviridae family. 162 Details of various risk factors associated with hepatitis C prevalence and progression in Pakistan are as follows.
Non sterilized and unnecessary needle use
In developing countries injections have been considered as main mode of transmission for HCV. 163 Some studies described a clear relationship between the injections usage and HCV seroprevalence. Khan took interview of 203 patients who left local clinics outside the Karachi. 164 On interview day 81% received injection. 135 patients gave serum sample, 44% had antibodies against HCV. Another study reported that hepatitis C positive patients in the previous 10 years, were more likely received more than five injections.
In Hafiz Abad the study of Luby et al. 165 showed that by using simple methods, the practice of using unsterilized needles could be improved. Multiple usage of a syringe in Pakistan is responsible for transmitting Hepatitis C virus. 166 Small business groups reported to be involved in the collection and repacking of used syringes without sterilization. 167 A study reported that out of 65% individuals who received injections in last 90 days, only 54% of them used freshly opened sterilized syringes. 168 Another study reported that reuse of syringes in Hyderabad and Sukhur was found to be 8% and 34% respectively. In Pakistan there is an increased trend of taking injections than using oral medications. 164 A person who takes 4 injections in a year has 11% more chances of getting Hepatitis C virus than the individuals who did not take injections. 169 Major cause of HCV infection is the usage of unsterilized syringes and needles. In rural areas of Pakistan, people usually believe that injection is the fastest way for relieving pain which increases the usage of syringes. 170 Data of 2 districts of Pakistan was collected (Dir and Mirpurkhas) in which it was showed that 68% of the people were given drugs by using syringes and out of them 54% used sterilized needles in past 3 months. 119 Developing countries should ensure the usage of properly sterilized needles and discard the used syringes and needles.
Transfusion of blood and blood products
To save people’s life blood transfusions are ultimate options in some circumstances. Due to frequency of increased transfusion of blood, prevalence of HCV is increasing day by day. In 1997, a study was carried out in Karachi. The number of blood banks selected were 24. It was shown that 23% of the blood banks were screened for HCV. 30% of the blood was not stored on recommended temperature. 25% of the blood banks were voluntarily donating the blood and 50% were paid donors.
Screening of blood is compulsory for safely donating the blood. Blood which is screened many times is safe. 171 Blood screening is necessary for safe transfusion of blood. Paid blood donation should not be despondent. Blood transfusion was thought to save the lives of the people, nowadays, is thought to be an increased source of HCV. 172 Transfusion of blood in thalassemia patients has increased the risk of HCV infection.
In Pakistan, number of blood centers are 1830, 85% out of them are private ones and rest of them are public centers, so therefore there is no uniformity. 173 Moreover, one of the major drawbacks is the gap which prevails in the surveillance system for transfusion as every third blood donor has hepatitis C. Similarly, distortion of human resources and infrastructure ensure the transfusion of blood because there are no proper setups for treatment of HCV in Larkana. 174
Shaving by barbers
In 1999, a study showed that in Rawalpindi, 13% of the barbers knew the fact that by using the contaminated syringes there is increased risk of HCV transmission. 175 11% of the barbers use sterilization techniques for washing razors and 46% of the barbers were again using the razors by not even washing. Therefore, the razors which are not properly autoclaved or sterilized can be the main sources of transmitting HCV because the virus remains on the razors and blades for many days. 176 In another study conducted in Gujrat, Pakistan, reported that 93% barbers did not know about the dangers of repeated use of shaving tools. 175 Seventy five percent barbers used the same potash alum on injuries resulted by facial shaves, a major contributing factor for transmitting Hepatitis C. 177 In Karachi a study conducted on 50 roadside barbers, 92% changed their razor blades for new customer. 178 Mostly, barbers disposed the used blades in general public waste, hence posing risk for sweepers during garbage handling. 179
A study showed that barbers are the main source of transmitting Hepatitis C virus. In sheikhupura and Punjab, prevalence of transfusion of HCV by barbers is 17.9% and among barbers is 58.6%. Another study conducted later in Islamabad, Punjab evidenced that in urban areas, nearly 92% and in rural areas, almost 68% possessed awareness about the disastrous effect of using contaminated razors and blades. 180
Lack of trained staff and needle pricking injuries
In Pakistan, transmission of HCV is more commonly in paramedics due to lacking of proper knowledge, standard procedures and training of medical procedures.175,181 Personals in the dialysis unit, paramedics, laboratory technicians, physicians and nurses are at high risk. Exposure to the infected blood which is occupational or non-occupational is the main risk factor. This is caused by improper handling of health care wastage, improper staff training for managing health care workers and unsatisfactory staff attitude towards the hospital discipline. 182 The procedures with increased risk of needle injury are withdrawing blood samples, subcutaneous or intramuscular injection, during intravenous cannulation, collision with someone, replacing cap on a used needle. 183 The prevalence of HCV is greater in HCV than in healthy people. The most common risk factor among healthcare professionals for transmitting the virus is reusing the syringes. 184
Pakistan faces several related challenges such as policy implementation in blood screening to meet national requirements, screening of all blood donations for different infections such as HCV in addition to adequate resources and availability of trained staff which may explain increased rates of blood transfusions. 185 Risk factor for HCV transmission among healthcare workers is percutaneous injury like a needle induced injury. A study investigated the HCV infection in the general public of Bannu, KPK stated that different factors such as illiteracy, lack of sterilized instruments and trained healthcare staff are the major reasons behind the HCV prevalence there.186,187 Usually, the health workers perform medical analysis on unsterilized syringes and most of them are not trained professionally and are not therapeutically capable and possess no knowledge regarding the general sterilization techniques. 188
Injection drug users
In Pakistan for acquiring hepatitis C, drug abusers are also the common factors. In Pakistan there are around 500,000 heroin addicts. 150, 000 (30%) are occasional while 75,000 (15%) are regular IDUs (103). Kuo et al. in 2003, reported HCV prevalence in the IDUs of Lahore 93% and Quetta 75% while in 2004, Achakzai et al. reported the prevalence of HCV in injection drug users of Quetta.
189
Intravenous drug users (IDUs) carry blood borne pathogens and act as a major contributor of HCV after blood transfusions
180
(Figure 1). Most common possible risk factors associated with the transmission of HCV infection in Pakistan.
In Pakistan, the major routes of HCV transfusion were studied and it was found that the maximum HCV prevalence was among IDUs. A study was conducted in which it was shown that out of (∼66,000) 52 of the IDUs, 88% (46) were having anti-HCV antibodies. High exposure to the HCV in the current study was correlated to the use of injectable drugs as well as awareness gap. In the same way a meta-analysis was performed regarding the HCV prevalence and stated that nearly 53.6% of the population that was used to inject drugs developed HCV. 75
Spousal transmission/household contacts
In a study Pasha et al. 190 reported that prevalence of HCV is 2.5 times greater in house members than general population. International literature reported that Hepatitis C virus transmission through the sexual contact is very low. 191 In another study it was shown that therapeutic usage of injections, previous surgery and sharing products like needles and nail cutters are the main cause of HCV seroprevalence in pregnant females. 192 A study showed that there is 4.4–38% increased risk of transmission of HCV among housemates. 193 Reinfection of HCV can also prevail in the household settings particularly, when family members are unaware of its transmission routes and hence, life style should be modified to avoid the reinfection. Also, there is a need to create awareness about the transmission routes in family members of HCV patients. 194
Unsterilized dental and surgical instruments
In Pakistan, unsterilized dental and surgical instruments are the main source of HCV transmission. Doctors use surgical instruments for treating indoor patients, this sometimes spread hepatitis C when Hepatitis C patients are surgically operated with reused instruments. Hospitals are not properly screened and sterilized and due to overcrowded patients, standard techniques are not being adopted. 195 Use of unsterilized instruments for dental and medical procedures has been regarded as a second most important risk factor towards the onset of HCV infection among healthy population, as dentists and medical experts use unsterilized medical equipment. 196
Improper disposal of hospital waste
In Pakistan, practice of improper disposal of hospital waste is rapidly increasing and due to this, used syringes are disposed of easily without proper destruction. 197 Currently, education programs for HCV awareness among the general populations are working on a limited level. In addition, some researchers often organize community awareness programs at their parent institutes. Counseling programs for the general public with higher risk groups and untreated patients provide an efficient preventive strategy against HCV globally. 198
Poor infra-structure
In Pakistan, government hospitals have not enough funds to provide health facilities and drugs. They have a short number of staff as some of them are absent on the duty therefore, reusing syringes and needles are the main source of spreading HCV among healthy patients and by 2030 it is expected that HCV infected patients will reach 12.6 million. Doctor’s irresponsible attitude, patients’ poverty, illiteracy and poor management of hospitals are main factors responsible for poor infrastructure. Health care system efficiency should be improved for achieving stipulated goals. 199 Lack of infrastructure and scarce human resources also serve as indirect sources of HCV hepatitis by compromising the safety of blood transfusions. More than 80% of the HCV infections range from low to middle income countries, where Pakistan harbors the second largest HCV burden globally and the number of infected persons is expected to reach 12.6 million by the end of 2030. 200
Others
In developing countries increased risk of Hepatitis C transmission is due to poor implementation of internationally accepted standards on perinatal transmission, body piercing, hemophilia, tattoos, hemodialysis, sexual activity, transplants, comb and razor sharing. 201 Vertical transmission, tattooing, multiple sexual partners, dialysis and ear and nose piercing were found risk factors for transmitting HCV infection. 202
Province-wise genotype distribution of hepatitis C virus
The development and severity of the disease, as well as the responsiveness of the patient to antiviral medication, are significantly influenced by the HCV genotype. As a result, precise genotyping of HCV isolates is critically important. Numerous methods of HCV genotyping have been published and extensively studied. In Punjab province, genotype 3 (subtype 3a, 80.23%) prevalence was much higher than the untypable (4.91%) genotype, which was significantly lower as compared to the other provinces. Following the subgenotype 3a were 4a (2.45%), 1a (6.46%), mixed (1.98%), and 3b (3.97%). Genotypes 1 (1b) and 2 (2a) accounted for 0.76 and 0.45% of the total sample pool, respectively. In Sindh province, the HCV patients with genotypes 4 (subgenotype 4b, 0.23%) and genotype 6 (subgenotype, 6a, 0.05%), genotype 3 (subgenotype 3a, 21%: 3b, 9%) and genotype 1 (subgenotype 1a, 4%: 1b, 2%), genotype 2 (subtype 2a, 2%) and mixed genotyped patients were 1%.203,204
Genotype 3 is the most prevalent in the provinces of Pakistan (Figure 2). This discovery also supports the existence of overlapping and related HCV transmission networks throughout Pakistan’s provinces. Only modest differences in genotype distribution were discovered among provinces, which appeared to represent transmission linkages with adjacent countries.205,206 In KPK, genotype 3 (3a, 49%) was followed by genotype 2 (2a, 12%) and untypable genotype (14%), however, in other parts of Pakistan, genotype 2 with subgenotype 2a was very uncommon. The prevalence of all other genotypes was genotype 3 (subgenotype 3b, 9%), genotype 1 (subgenotype 1a, 7%), and mixed genotypes were 5%. Genotypes 4 (subgenotype, 4a) and genotype 2 (subgenotype, 2b) were expressed as 1% of all KPK samples genotyped. The data from Baluchistan province is very scarce. The genotype distribution in (a) Azad Jammu and Kashmir, (b) Balochistan (c) Sindh, (d) Khyber Pakhtunkhwa (e) Punjab.
203
GT 1; Genotype 1: GT 2; Genotype 2: GT 3; Genotype 3: GT 4; Genotype 4: GT 5; Genotype 5: GT 6; Genotype 6.
In HCV-positive samples (28 patients) genotype was determined and the majority of patients of Balochistan were infected with genotype 3 (subgenotype, 3a, 50%), followed by untyped genotypes (32%), while genotype 1 (subgenotype, 1a) and genotypes 3 (subgenotype, 3b) were 11% and 7% respectively. The most prevalent genotype of Azad Jammu and Kashmir (AJK) was genotype 3 (subgenotype 3a, 59%) followed by genotype 1 (subgenotypes 1b, 7%: 1a, 7%), genotype 2 (subgenotype 2a, 4%) and genotype 3 (subgenotype 3b, 19%).
Genotypes 4, 5, and 6 were not identified in the AJK, Pakistan. In all provinces of Pakistan, genotype 3 (subgenotype, 3a) was the most abundant and its percentage distribution per province is Baluchistan (50%), KPK (49%), AJK (59%), Sindh (61%) and Punjab (80.23%). Untypable genotypes were the second most prevalent genotype in KPK (14%), Sindh (21%) and Balochistan (32%) as compared to Punjab (4.91%) and AJK (4%). 203
The quantitative analyses of several factors of Pakistan’s HCV pandemic are based on a systematic collection of HCV data.207,208 It was estimated that 12.9 million people in Pakistan have been infected with HCV, 8.7 million of whom are chronically infected but broadly consistent with previous estimates ranging from 6.7 to 7.8 million chronic infections.207,208
The number of patients with HCV who underwent treatment remained relatively low in 2016 which emphasizes the importance of implementing and planning to diagnose and treat HCV on large scale to reach WHO standards. 200 Pakistan’s National Hepatitis Strategic Framework (NHSF) 2017–2021 was established to eliminate HCV by 2030 and to address the high burden of HCV. 209
Pangenotypic treatment regimens in Pakistan
The pangenotypic is the most important factor in determining sustained virological response (SVR). In previous studies, interferon (IFN) was the principal therapeutic option in Pakistan because of its affordability and accessibility against certain genotypes. Direct-acting antivirals (DAA) have converted the therapeutic strategy to reduce side effects and increase SVR.
The Asian Pacific encourages the use of Solvadi to treat genotypes GT3, GT2, and GT1 for liver treatment. The identification of genotype is important to select therapeutic techniques and necessary to study the HCV genotype distribution in different provinces of Pakistan to appropriately develop a treatment plan based on viral genotype.210,211
New direct-acting antivirals (DAAs) are replacing older treatments for persistent HCV infections in Pakistan. One of the registered and widely available DAAs in Pakistan is Sofosbuvir (SOF) and ribavirin (RBV), which have been in the market since November 2014. When compared to IFN-based therapy, SOF was shown fewer adverse effects. Although SOF is highly successful, its exorbitant cost prevents widespread usage in Pakistan. Since Pakistan is one of the high-burden countries for HCV, 212 the government and the pharmaceutical companies producing SOF have agreed to give it at a significantly lower price. Furthermore, the National Guidelines for HCV treatment in Pakistan now include a SOF-based treatment regimen, which has expanded its utilization by doctors. Although the SOF-based therapy regimen has been the primary source of DAA use, newer more effective DAAs have been embraced in Pakistan. Daclatasvir (DCV) was recently introduced into the treatment plan and made available in Pakistan. Improvements in patient adherence and safety are a direct result of such additions 213
Different studies in Pakistan, mostly from the Punjab area, found that SOF-based therapy was effective in treating people infected with HCV genotype 3. Genotype 3 individuals have shown excellent response rates to dual or triple treatment based on SOF, ranging from 82.2% to 99.34%.214–216 The biggest research to date, conducted in Lahore between 2014 and 2016, found that patients infected with genotype 3 who received SOF as part of a double or triple therapy program had an SVR rate of 97–99%. 217
Discussion
Earlier studies depicted the prevalence of HCV in Pakistan and its geographic distribution are critical to managing the growing incidence of HCV. These studies aid in the development of more effective preventative and treatment techniques. 218 HCV has a critical healthcare issue in Pakistan since it causes acute and chronic infections that result in liver damage, cirrhosis and hepatocellular cancer. Hepatitis C virus is a blood-borne virus that is spread by exposure to tiny quantities of blood. HCV is transferred by the use of unsafe injections, the use of infected medical devices during surgical procedures, and the transfusion of unscreened blood and blood products. Globally, around 185 million individuals are afflicted with Hepatitis C. Pakistan has the second-highest seroprevalence of hepatitis C virus (HCV) infections in the world. HCV infected population of Pakistan is about 10 million. 219
Over 71 million individuals worldwide are infected with the chronic hepatitis C virus (HCV). HCV has the tendency of fibrosis, cirrhosis, and liver cancer. Mongolian children (1.74%) had the greatest frequency of HCV infection, followed by Pakistani children (1.02%). Pediatric HCV prevalence was found to be 1.88% in Punjab, Pakistan.220,221
In Pakistan, the most often detected subcategories of genotypes are 1a and 3a (genotype 3), with the greatest prevalence of genotype 3a. Untypable genotypes comprise the second-largest reading, followed by 1a, 1b, and 3b (genotypes 1 and 3). Earlier research found that 3a is more frequent in Punjab Provinces,222,223 and earlier research depicted that 2a and 1b are less prevalent in the region of Punjab. It was found that 3a is the most frequent genotype (50.8%) in the Sindh population, followed by untsypable (47%) and 2a (1.6%) in a total of 120 sample sizes. Injection drug usage was linked to a high frequency of HCV infection.203,224,225 The pangenotypic regimens are important to treat the infection, prognosis, and clinical treatment of HCV related to all genotypes. The Asian-Pacific region recommends Solvadi for the treatment of liver disease in people with the GT3, GT2, and GT1 genotypes. With the advent of direct-acting antivirals (DAA), the treatment approach has shifted to prioritize fewer adverse effects and a higher SVR. 210
An earlier study by Ayoub et al. used a method based on mathematical modeling and described the HCV pandemic in Pakistan, one of the greatest epidemics in the world. Based on Ayoub et al. findings, the rate of new HCV infections and the overall frequency of the virus have been falling for almost two decades, although very slowly. When compared to other worldwide HCV epidemics, the rapid growth of this large-scale pandemic from the 1970s through the 1990s and the fact that it has been mostly affecting people in their twenties and thirties is striking in Pakistan. 226 By 2050, the age group with the largest infection burden will be an individual older than 60, as the young infected cohort matures and the incidence continues to fall. The related diseases and infections owing to HCV such as fibrosis, cirrhosis and liver cancer are expected to grow, perhaps for many decades if the HCV pandemic is not controlled. 207
There is no single, definitive explanation for the observed decreases in HCV prevalence, chronic infection prevalence, incidence, and incidence rate. The first is the cohort effect, in which older age groups with a higher HCV prevalence are dying off and being replaced by younger age groups with a lower risk of HCV exposure and a lower HCV prevalence. This may be the result of specific historical events, such as Pakistan’s first 5 year health plan in the 1950s. The comparatively high fertility rate in Pakistan may cause a “demographic dilution” of the prevalence and incidence rate.
An enormous number of infants born each year join the community without prior exposure to HCV. Since the number of people used as a denominator in calculations of HCV prevalence and incidence rate is growing faster than the number of people infected with HCV, the results are skewed downwards.226,227 Increasing blood screening coverage and may be better infection control in certain parts of the healthcare system may also be significant factors. The considerable drop in HCV incidence rate seen in Pakistan soon after the virus’s discovery is consistent with international experience suggesting that even limited rollout of therapies may result in a quick fall in HCV incidence rate.228,229
Labs and doctors may be bound to report cases of HCV to local government health agencies for HCV monitoring. Both acute and chronic hepatitis C cases are tracked via surveillance efforts; however, not all regions have access to the diagnostic laboratory tests needed to differentiate between active and latent HCV infection. Furthermore, certain nations and local regions may lack the ability to investigate and diagnose cases due to the increase in chronic hepatitis C prevalence and the time-consuming follow-up studies. Despite the difficulties in hepatitis C monitoring, there is still hope for eradication since secondary transmission and consequences may be avoided by case management, more effective medicines, and alcohol counselling in addition to excellent primary prevention. Information gathered via surveillance systems is crucial for public health practitioners to use in formulating, enforcing, and assessing their own practices. 230
A positive antibody test is often the first step in reporting a case of HCV and can suggest either acute or chronic infection. Health departments have the option of doing follow-up investigations or waiting for future laboratory findings after checking the surveillance database to see whether the possible case has been reported before and had other epidemiologic or laboratory information. The next step could involve checking the case of the patient by the doctor to see if they experienced any hepatitis symptoms. In addition to the fact that the case meets the criteria for a newly reported case of acute HCV infection. There is a need to increase hygienic conditions or better awareness of the importance of maintaining proper hygiene and preventing exposure to contaminated food and water.
Hepatitis C treatment is available through the Prime Minister’s Program for Hepatitis Control, while awareness was raised through public awareness campaigns and world hepatitis day in Pakistan. The Hepatitis prevention and Treatment Program in Pakistan laid the groundwork for expanding access to testing and care. Establishing a national policy for HCV screening of the general population, setting screening and testing targets for local health facilities, training health care workers to increase access to screening and treatment, increasing the availability of low-cost diagnostics and treatment, streamlining diagnosis and treatment algorithms. In addition, new methods of financing might be investigated to help Pakistan get the funds necessary to expand its HCV screening and treatment programs. Successful testing and treatment would be crucial in the primary prevention of HCV infection by halting the ongoing risk of primary infections and additional infections, which would be an additional benefit of HCV treatment beyond merely slowing the progression of liver disease in people with HCV infection. Eliminating the spread of HCV in Pakistan may depend on bringing the rate of new infections down. 231
The Pakistani government has adopted national and provincial efforts based on well-established policies. On global hepatitis day in 2019, the aim of Pakistan was to eliminate HCV by 2030. These initiatives include medical staff training following the WHO-prescribed manual, management of treatments with drugs and diagnostic strategies in prisons, providing blood transfusion after the screening, public awareness programs, and enhancement of diagnostic tools and therapeutic centers. As there are no verifiable statistics about the developing facilities, it is premature to conclude that present measures are sufficient to combat persistent infection levels.224,225,232
In Pakistan, getting and analyzing data about epidemiology is hard because there are not enough death and disease data or health management. The present data is comprised of studies conducted in hospitals. There is great variability in the prevalence of HCV in different cities in Pakistan. The present review is focused on published data about the risk factors and prevalence of HCV in Pakistan. Anti-HCV antibody data from various regions of patients and the population was gathered.
In addition, the current review suggests that the incidence of HCV in rural and peri-urban regions is particularly high. This socioeconomic aspect of the HCV pandemic in Pakistan has received far less attention. Given that the bulk of Pakistan’s population dwells in these rural regions with high HCV incidence, the actual HCV burden in Pakistan is significantly greater. A greater emphasis is required to determine the incidence of HCV in rural regions to improve the diagnosis and implementation of preventive measures. In addition, because of current WHO recommendations, additional effort must be put into recognizing the prevalence of active HCV patients in Pakistan.
We discovered that eliminating HCV in Pakistan is possible, however, it would need significant effort; at least 25 million individuals will need to be tested annually to identify 900,000 HCV infections, and at least 700,000 patients will need treatment annually. This capacity objective, which would result in a multiplication of both treatment and diagnosis by a factor of four compared to current rates, may be useful in tracking advancement toward the ultimate goal of HCV eradication by 2030. Based on our findings, eliminating HCV in Pakistan may not be possible until these interim capacity objectives are achieved.
Our findings highlight the critical need to expedite the diagnosis of HCV infection and to identify the millions of people who are living with HCV infection but have not yet been identified. HCV testing and treatment are being expanded in Pakistan, however more people are getting therapy than getting tested. Multiple micro-elimination efforts are now underway for HCV, and these initiatives are crucial in locating infected people and getting them into treatment. Due to the widespread nature of the HCV epidemic in Pakistan, screening the entire population is necessary for the disease to be eradicated, but it could be optimized by focusing on higher-prevalence subpopulations first and facilitating better treatment linkage for those who are diagnosed. The results of these first attempts can then be extrapolated to other subgroups with a similar frequency.
While it would be necessary to make an initial expenditure to increase the capacity for diagnosis and treatment, our findings suggest that doing so may prove to be financially beneficial in the long run, particularly if novel methods are adopted for verifying the diagnosis. Savings higher than $2.6 billion are possible if the price of new diagnostics can be lowered. In addition, the relative distribution of HCV prevalence subtypes in all the provinces of Pakistan was different. Genotype 3 is the most frequent, and the prevalence of genotype 2 has increased in Sindh and KPK in recent years. This variation in the distribution of genotypes over time has profound consequences for eliminating HCV in Pakistan. A large population with HCV was not identified as a single genotype and requires modifications to present strategies to get a better knowledge of HCV evolutionary patterns and genotype distribution in Pakistan.
Conclusion
HCV burden is increasing in Pakistan. This present review examines the prevalence, risk factors and distribution pattern of HCV genotypes in the provinces of Pakistan. The absence of effective diagnostic techniques in Pakistan and the lack of awareness about the various mode of transmission of HCV contribute significantly to the development of the illness among the people. To prevent a far greater danger of HCV infections, sterilization and screening measures must be made obligatory in public health care facilities. The policy makers should create and enforce the implementation of regulations and prohibit the employment of untrained dental quakes across the province. A high incidence was identified among IDUs that indicated that the reuse of syringes was prevalent among IDUs.
The most prevalent HCV genotype was 3a. The majority of HCV positive patients were reported to have their faces and armpits shaved by barbers, demonstrating that barbershops were the primary source of viral transmission. Extremely few commercial sex workers used condoms and knowledge of sexually transmitted illnesses was poor within this population. In Pakistan, the anticipated number of injections per person per year is quite high since most Pakistanis believe that injectable medications are more effective than oral medications. People were often unaware of the many risk factors related to HCV transmission. The high cost of hepatitis treatment exerts a significant effect on the nation’s economy.
To reduce the future health and economic impact of the illness, more focus should be placed on preventative measures, such as screened blood transfusions, effective sanitation practices in clinics and hospitals and the use of disposable syringes and razor blades. The government should take active measures to raise public awareness via the use of the media or by altering the school curriculum. The most frequent genotype in Pakistan is 3a, followed by an untypeable genotype. There were no HCV patients data available from Gilgit Province and few records from Balochistan were recorded; hence, further systematic study of genotype distribution in these provinces is required. The identification of genotypes is essential for viral eradication and treatment efficacy. For the management of HCV is necessary to develop a medication with a high SVR and minimum side effects.
The actual burden of HCV in Pakistan is much higher. Moreover, because of recent WHO and CDC guidelines, more effort must be invested to determine the prevalence of active HCV infection in Pakistan. The analysis also showed a shift in the relative frequency distribution of HCV subtypes in various regions of Pakistan. The high proportion of samples that could not be assigned to a specific genotype demands improvements in the methodologies currently used to develop a better understanding of HCV genotype distribution and evolutionary trends in Pakistan.
A greater emphasis is required on determining HCV prevalence in rural regions to improve the assessment and implementation of prevention strategies for HCV. As a result of new WHO recommendations, more work must be done to find out how many people in Pakistan have active HCV infections. Preventive measures including screening blood transfusions, adequate sanitation practices in clinics and hospitals, and the use of disposable syringes and razor blades should be given more attention to reducing HCV and its economic cost.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.