
Abstract
This study aims to investigate the postoperative cognitive function changes of infants who underwent endoscopic third ventriculostomy (ETV) or ventriculoperitoneal shunt (VPS) for the treatment of congenital hydrocephalus. Data of 70 hydrocephalus infants and children were retrospectively analyzed. Among these patients, 20 patients underwent ETV, 27 patients underwent VPS, and 23 patients did not undergo any operation (controls). All patients were routinely cared after discharge. The Gecell Developmental Diagnostic Scale was filled for all patients at 2 weeks, 2 months, and 6 months after diagnosis. A total of 20 patients in the ETV group were followed up for 6 months. Among these patients, the clinical symptoms of 18 patients significantly improved. Results determined at 6 months after surgery in the ETV group was statistically significant, compared with the control group (P < 0.05). Results determined at 2 and 6 months after surgery in the VPS group were statistically significant, compared with the control group (P < 0.05). Developmental quotient (DQ) values in these two operation groups increased after the operation (P < 0.01), and the differences were statistically significant. ETV and VPS can improve the cognitive function of infants with hydrocephalus. Improvement of cognitive function by VPS is more significant for infants.
Keywords
Introduction
Hydrocephalus can occur in children and adults, but is more common in children. The estimated incidence of hydrocephalus is 1%–1.5%, and the incidence of congenital hydrocephalus is 0.2–3.5/1000 newborns. 1 Up to the 1950s, with the application of the valve shunt system and gradual improvement of the shunt device, ventriculoperitoneal shunt (VPS) operation has been widely used, and even become the only choice of treatment for hydrocephalus for a period of time. However, there are some complications related to shunt tubes such as shunt tube blockage, 2 shunt system infection, 3 and excessive shunt. 4 As endoscopic instruments and surgical techniques constantly developed, third ventriculostomy has gradually become one of the removal methods for the treatment of hydrocephalus. It has been reported that the incidence of complications of endoscopic third ventriculostomy (ETV) was significantly lower than that of VPS. 5 At present, both ETV and VPS are the main treatment methods for hydrocephalus in children. However, the most appropriate kind of surgery still remains controversial.
For infants with hydrocephalus, quality of life (QOL) is the most important prognostic indicator. 6 Previous studies revealed that among the indexes for evaluating the QOL of children with hydrocephalus, cognitive impairment was the most important one. 7 To determine the effect of these two kinds of surgical approaches on cognitive function of infants with congenital hydrocephalus, we conducted this retrospective cohort study. The data of 70 infants with congenital hydrocephalus, who were admitted in our hospital from January 2009 to December 2014, were collected and analyzed.
Materials and methods
This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the Ethics Committee of The First Affiliated Hospital of Xinjiang Medical University. Written informed consent was obtained from the participants.
General information
We retrospectively evaluated 70 patients treated for hydrocephalus from January 2009 to December 2014. Among those, 20 patients (13 males, 7 females; age range: 0.25–1 years; mean: 0.58 years) were treated by ETV (ETV group), 27 patients (17 males, 10 females; age range: 0.25–1 years; mean: 0.66 years) were treated by VPS; and 23 patients (12 males, 11 females; mean age: 0.58 years) did not undergo any operation for various reasons (control group). The inclusion criteria were the following: patients who were ⩽1 year old, diagnosed with hydrocephalus by computed tomography (CT) or magnetic resonance imaging (MRI), had definite clinical manifestations of children hydrocephalus. The exclusion criteria were the following: patients with hydrocephalus caused by acute intracranial infections, hemorrhage, tumors or other diseases; hydrocephalus patients with meningocele, myelomeningocele, Chiari malformation, and other congenital diseases.
Diagnostic criteria
According to the Vassilouthis method, CT/MRI was used to determine the degree of hydrocephalus by measuring the ventricle/skull ratio, a ratio <0.15 is regarded as normal, a ratio between 0.15 and 0.20 suggests mild hydrocephalus, a ratio between 0.20 and 0.25 suggests moderate hydrocephalus, and a ratio >0.25 suggests severe hydrocephalus. 8
Surgical methods
(1) ETV: After successful general anesthesia, the patient was placed in the supine position, and the head was elevated by 10°–15°. A horseshoe-shaped incision was made at the site 2 cm in front of the right coronary suture and 2 cm from the midline. The flap was folded up from the subgaleal layer to the forehead, the periosteum was cut off and opened, a hole was drilled on the skull (the bone hole should not be under the incision), a bone flap with a size of 3 cm × 3 cm was made using a milling cutter (infants with unclosed anterior fontanelle did not undergo this step). The dura matter was cut off in a horseshoe shape in the reverse direction of the skin incision. After local brain tissue was burned by electrocautery, the surface of the frontal lobe was punctured with a sheath. When a large amount of cerebrospinal fluid was found to flood out, water was rapidly perfused into the inner cavity of the sheath to prevent gas bubble formation. An Aesculap 0° ventriculoscope PE184A (Germany) was inserted through the sheath into the lateral ventricle, interventricular foramen was found through anatomical relationship, and the ventriculoscope entered the third ventricle through the interventricular foramen. Then, the structure of the third ventricle was observed. A fistula was made in the thinnest and vessel-free area in the central part of the front parts of the bilateral mammillary bodies. The stoma was expanded to approximately 7 mm to observe the important anatomical landmarks in the interpeduncular cistern through the stoma, detect any active bleeding, and confirm that the third ventricle communicated with the interpeduncular cistern. If bleeding was found during the operation, the endoscope should not be withdrawn. Instead, continuous flushing toward the bleeding points should be performed. Most small amount of bleedings could be stopped after washing. During the whole process of the operation, washing was continued with normal saline at 37°C to ensure that the ventricle was filled with liquid at the end of the operation, preventing the occurrence of intracranial pneumatosis and cortical collapse. The sinus was obstructed with small pieces of gelatin sponge, and it should be ensured that the dural suture must be tight, in order to prevent cerebrospinal fluid leakage. The bone flap underwent reduction and fixation, and the periosteum, subcutaneous tissue, and skin were sutured successively. Then, the incision was tied and covered with sterile dressing materials, and the operation was finished. (2) VPS: According to head CT or MRI, the location and depth of the puncture were determined before the operation. After general anesthesia, the patient was placed in the lateral decubitus position with the head turned to the left, and the right shoulder was elevated with a pad. After positioning according to the image, the location of the incision was determined in the right occiput area, and the skin and subcutaneous tissue were cut off in turns up to the periosteum. Usually, the puncture point was located at the site 7 cm above the occipital tuberosity and 3 cm on the right side from the midline. A hole was drilled on the skull and the dural matter was cut off, local brain tissue was burned by electrocautery, and the puncture was performed on the occipital horns. A ventricular catheter was placed. The head of the ventricular catheter was located at the site 1–2 cm in front of the interventricular foramen, and the split flow pump was embedded in the lateral outside of the puncture site. Abdominal incision was made on the rectus abdominis in the right upper abdomen. Incision length was 3 cm. The skin and fascia were cut off to expose the anterior sheath of the rectus abdominis, the rectus abdominis was gradually separated up to the peritoneum, and a small incision was made on the peritoneal surface. When all the above operations were determined to be correct, the abdominal catheter was inserted into the abdominal cavity with enough length of insertion, and the end was left free. The tube traveled along the back of the neck, the lateral margin of the sternocleidomastoid muscle, and to the suprasternal fossa. Then, the tube traveled along the surface of the sternum to the right upper abdomen, the upper margin of the sternum, passed through the abdominal incision, and was connected with the split flow pump via the abdominal catheter. The incision was sutured layer by layer. The incision was tied and covered with sterile dressing materials. The operation was finished.
Inspection content
At 2 weeks, 2 months, and 6 months after surgery, all patients underwent head CT/MRI to measure the width of the bilateral ventricles corresponding to the frontal angles and the width of the third ventricle. Then, the developmental quotient (DQ) for adaptive behavior, large motor behavior, fine motor behavior, language behavior and the individual-social behavior of infants was measured by professionals using the Gesell Developmental Diagnostic Scale. 7
Statistical analysis
Data were analyzed using SPSS 18.0 statistical software. Count data were expressed as percentage. DQ, frontal angle width of bilateral ventricular, and diacele width were measured and expressed as mean ± SD (standard deviation). Comparison of DQ among three groups was determined by one-way analysis of variance (ANOVA) and the pairwise comparison was determined by least significant difference (LSD). The comparison of frontal angle width of ventricular and diacele width at different times was determined by ANOVA for repeated measurement. Inspection level was set at α = 0.05. P < 0.05 was considered statistically significant.
Results
The 20 patients in the ETV group were followed up for 6 months. Among these patients, 18 patients had significantly improved clinical symptoms. For the remaining two patients, no improvement was achieved and the ventricles continued to increase. The 27 infants in the VPS group were followed up for 6 months. The clinical symptoms of all 27 patients significantly improved, and no obvious complications occurred. The infants in the control group were followed up for 6 months, and their clinical symptoms were not relieved.
Comparison of DQ values among the ETV, VPS, and control groups is shown in Figure 1. The DQ value of ETV group was statistically significant compared to the control at 6 months after surgery (P < 0.05). But for the results measured at other treatment time, the difference between ETV and control groups was not significant (P > 0.05). We also observed that the difference of DQ values between VPS and control groups was statistically significant at 2 and 6 months after surgery (P < 0.05). Moreover, we found that DQ values in these two operation groups increased after the operation, and the values between the two groups were significantly different at 2 and 6 months after surgery, respectively (P < 0.05).
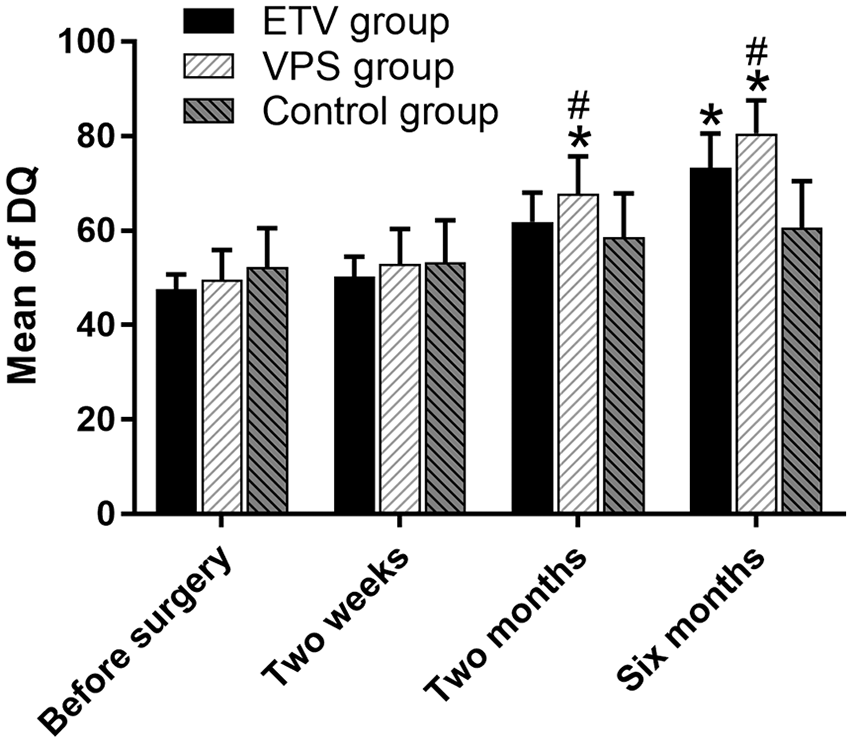
Mean of DQ among the ETV, VPS, and control groups. *P < 0.05 versus control group; #P < 0.05 versus ETV group.
Results of the preoperative and postoperative ventricular measurements are shown in Tables 1 and 2. From the data, the lateral ventricle and third ventricle shrunk after the operation in the ETV group, and the differences were statistically significant (P < 0.05; Table 1). Furthermore, the lateral ventricle and third ventricle shrunk after operation in the VPS group, but the difference in the lateral ventricle was not statistically significant (P > 0.05), while the difference in the third ventricle was statistically significant (P < 0.05; Table 2).
CT/MRI ventricle size measurement results preoperative and ETV postoperative (mm).

CT: computed tomography; MRI: magnetic resonance imaging; ETV: endoscopic third ventriculostomy.
Results adjusted by Greenhouse–Geisser.
CT/MRI ventricle size measurement results preoperative and VPS postoperative (mm).

CT: computed tomography; MRI: magnetic resonance imaging; VPS: ventriculoperitoneal shunt.
Results adjusted by Greenhouse–Geisser.
Discussion
ETV and VPS are the main treatment methods for hydrocephalus in children. The purpose of these two surgical treatments is to establish a cerebrospinal fluid circulation bypass that could reduce pressure in the brain, improve the symptoms of hydrocephalus, and restore brain function. A study revealed that the clinical symptoms of patients with obstructive hydrocephalus were significantly improved within 1 week after ETV, and the positive predictive rate was as high as 94.1%. 9 In this study, the 20 infants in the ETV group were followed up for 6 months. Among these infants, 18 had significantly improved clinical symptoms. A high response rate was also found in our VPS group, the clinical symptoms of all 27 patients were significantly improved, and no obvious complications occurred. Furthermore, the differences in DQ between the ETV group and control group, and between the VPS group and control group, were statistically significant. These results indicated that both ETV and VPS could improve the cognitive function of infants with hydrocephalus.
Previous studies have revealed that quantitative detection of the morphology of the third ventricle could reflect the curative effect of ETV.10,11 In this study, although third ventricle changes in the ETV group were not as significant as that in the VPS group, the comparison between before and after surgery was statistically significant, and this was consistent with that reported in literature.10,11
Some experts and scholars proposed that age is one of the key factors for the success of surgery in hydrocephalus children. 12 In this study, the differences in DQ determined at 2 and 6 months after the operation between the ETV group and VPS group were statistically significant. We strongly believe that the effect of VPS on the recovery of brain function in infants is better than ETV.
This study has some limitations. First, the causes of hydrocephalus were not strictly evaluated. Second, since clinicians had a certain tendency to choose the surgical procedures, the reported results had a high risk of selection bias. Third, the follow-up period was not enough to observe the long-term effects of the two treatment methods. These problems would be refined in our further studies.
Conclusion
ETV and VPS can improve the cognitive function of infants with hydrocephalus. Improvement of cognitive function by VPS is more significant for infants. However, in clinical work, it is recommended that the guardians of these infants should be fully informed of the advantages and disadvantages of these two surgical approaches. In the choice of surgical procedures, we should take into the desire of the guardians of the infants.
Footnotes
Acknowledgements
W-Y.J. and N.C. contributed equally.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.