
Abstract
The objective of this study is to explore changes in main immune cells during acute coronary syndrome (ACS), including changes in subsets of monocytes, T cells, and inhibitory myeloid-derived suppressor cells (MDSCs), and to evaluate possible mechanisms. A total of 50 patients suffering from ACS were divided into two subgroups based on attacks of acute infarction, acute myocardial infarction (AMI) with infarction including ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina (UA). Third, the subgroup of 19 healthy subjects was labeled the normal group (NG). CD14, CD16, and CD45 were used as markers of the subset of monocytes. CD4, CD8, and CD3 were used as markers of the subset of T cells and CD14, human leukocyte antigen—DR isotype (HLA-DR), and CD45 were used as markers of inhibitory MDSCs. Both CD11b+ CD206+ and CD11b+ CD68+ cells were also assayed. Our data indicated that lymphocytes/karyocytes and monocytes/karyocytes as well as those of CD3+ CD4+ T cells, CD14+ CD16– monocytes, CD14+ CD16+ monocytes, and CD11b+ CD68+ monocytes were significant in all three groups (P < 0.05). The ratio of T-cell subtypes to total lymphocytes among the three subgroups can be represented as AMI > UA > NG (P < 0.05). The ratios of CD14+ monocytes to total karyocytes among the three subgroups can be represented as NG > UA > AMI (P < 0.05). The ratios of CD14+ CD16– monocytes to total karyocytes among the three subgroups can be represented as NG > UA > AMI (P < 0.05). The ratios of CD14+ CD16+ monocytes to total karyocytes among the three subgroups can be represented as AMI > UA > NG (P < 0.05). There were no significant differences in the proportion of MDSCs (P > 0.05). Certain subsets of monocytes are closely associated with ACS, of which CD14+ CD16– monocytes present a negative association, while CD14+ CD16+ monocytes show a positive association. In addition, adaptive immunity is associated with unstable plaques of ACS, and CD3+ CD4+ T cells may play a role in early stages of ACS.
Based on the latest research, atherosclerosis is believed to be a chronic disease induced by the innate immune response and adaptive immune response. It is also known that various immune cells play important roles during the development of this disease.1–3 Acute coronary syndrome (ACS), the terminal stage of coronary atherosclerotic heart disease (CAD), is considered to be a major threat to health and life. 4 ACS, as a kind of acute ischemic syndrome caused by occlusion of thrombosis due to rupture or erosion of unstable plaques, may lead to worse clinical outcome. Coronary angiography (CAG) has been confirmed as the golden standard for ACS and clinically ACS can be defined when any two items of the following three criteria are found: (1) ischemic chest pain, (2) dynamic changes of electrocardiography (EKG), and (3) elevation of myocardial enzymes. Clinically, ACS is classified into three subtypes based on whether or not ST-segment elevation is observed: ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina (UA). Myocardial infarction is found in both STEMI with complete obstruction of the lumen and NSTEMI with partial obstruction (>70%) of the lumen, which means that positive creatine kinase MB (CK-MB) and cardiac troponin I (cTnI) are often found in these two subtypes. However, single myocardial ischemia is found in UA with negative CK-MB and cTnI.
It is suggested that there is an association between heart disease and immune cells, including T cells as well as mononuclear macrophages, and ACS;5–7 however, few studies have focused on further investigating this relationship and any possible mechanisms. This study aims to demonstrate changes of immune cells in three subtypes of ACS and explore potential mechanisms.
Materials and methods
Subjects
A total of 50 patients with ACS admitted to the First Affiliated Hospital of Anhui Medical University between June and October 2016 were enrolled, together with 19 healthy subjects. The patients were divided into two subgroups with or without acute myocardial infarction (AMI), AMI with infarction including STEMI and NSTEMI, and UA with unstable angina. Third, the subgroup of remaining healthy subjects was labeled as the normal group (NG). ACS was diagnosed by history, CAG, EKG, echocardiography, and biomarkers of myocardial injury. All patients with ACS were older than 40 years and the number of heart attacks within 72 h was at least one. All healthy subjects were also older than 40 years and without any angina history and with normal 24h Holter recordings, echocardiography, and cTnI. The exclusion criteria were acute and chronic inflammatory diseases including inflammatory bowel disease, rheumatoid arthritis and systemic lupus erythematosus, cancer, chronic liver injury, kidney failure, left ventricular ejection fraction (LVEF) < 40%, structural deformity of the heart, and hematological disease. Any patients who had received anticoagulation agents, antiplatelet agglutination (including aspirin) as well as antiarrhythmics, immunosuppressants, antibiotics, glucocorticoids, or other complex Chinese traditional medicines which could disturb the results, within 6 months before the study, were also excluded. In addition, any patients with a history of percutaneous coronary intervention (PCI), autoimmune diseases, or genetic disorders and without a clear medical history were also excluded. Furthermore, patients with UA who suffered cardiac arrest, cardiac shock, hypotension, or pulmonary congestion were excluded. The estimation of sample size was confirmed based on major effect index (total proportion of lymphocytes) as well as comparison between the AMI and NG groups. Intergroup expected difference of the proportion of lymphocytes was 11 and standard difference was also 11. The power of test was 0.8 and the drop rate was 0.2. Therefore, the minimum size for each group was 17.
This study has been approved by the Ethics Committee of the First Affiliated Hospital of Anhui Medical University. All patients participating in the study have signed the informed consent.
Diagnostic criteria
Hypertension was defined as blood pressure > 140/90 mmHg or stabilization with medical intervention. Diabetes mellitus was defined as a level of blood glucose > 126 mg/dL or random glucose > 200 mg/dL or stabilization with medical intervention. Smoking history was defined as a period of smoking > 6 months. STEMI was defined as acute chest pain with a period of angina more than 30 min and elevated ST-segment, together with elevated biomarkers of myocardial injury and acute obstructive lesions matching the changes of EKG within the main coronary arteries. NSTEMI was defined as acute chest pain, with the period of angina lasting more than 30 min, together with ST-segment depression. Biomarkers of myocardial injury were elevated and acute obstructive lesions within the main coronary arteries (>70%) were found. UA was defined as irregular chest pain with the period of angina lasting less than 30 min, together with ST-segment depression. Biomarkers of myocardial injury were almost normal and acute obstructive lesions within the main coronary arteries (>70%) were found.
Material selection and sampling
Clinical materials
The clinical materials of patients were history and general information including age, gender, smoking history, alcohol consumption, medical intervention, and past history (hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, surgery, family genetic disease). Ejection fraction (EF), CAG, and EKG were recorded.
Sampling
A 3mL sample of blood anticoagulated with ethylenediaminetetraacetic acid (EDTA) was taken from patients with ACS by EKG, history, and cTnI at the time of CAG within 6 h after the onset of ACS and before invasive PCI which could disturb the results. Samples from the 19 healthy subjects were taken after normal 24h Holter recordings, echocardiography, and cTnI were confirmed. Flow cytometric assays were performed at 3 h after sampling.
Cell assays
Assay of monocytes
Heparinized anticoagulated blood was placed into two tubes, 100 µL per tube. Then 10 µL of anti-CD206 fluorescein isothiocyanate (FITC) and 10 µL of anti-CD11b PE (markers of M2 monocytes) were added to the first tube, while 10 µL of anti-CD68 FITC and 10 µL of anti-CD 11b PE (markers of M1 monocytes) were added to the second tube. A control tube was set up and treated with the same 10 µL of antibodies. All tubes were mixed with a whirlpool mixer and then placed away from light at room temperature for 15 min. To each tube was added 900 µL hemolytic agent, and then it was shaken evenly and placed into a water bath at 37°C for 10 min before analysis by fluorescence-activated cell sorting (FACS). The number of cells in each sample was more than 10,000 and the assay data were stored in Listmode.
Assay of monocyte subtypes
Aliquots of whole blood were placed into two tubes, 100 µL per tube, and 10 µL of each of the antibodies anti-CD14 FITC, anti-CD16 PE, and anti-CD45 PC5 was added to one tube. The other tube was used as the control and treated with 10 µL of the same antibodies. After mixing in a whirlpool mixer, all tubes were placed away from light at room temperature for 15 min. After incubation, 900 µL hemolytic agent was added to each tube, shaken evenly, and then placed into a water bath at 37°C for 10 min before analysis. CD14 was used to label monocytes, and the labeled monocytes were further divided into CD14+ CD16– subtype and CD14+ CD16+ subtype based on the expression level of CD16. The number of cells sampled was more than 10,000 and the assay data were stored in Listmode.
Assay of myeloid-derived suppressor cells
Whole blood was placed into two tubes, 100 µL per tube. To one tube was added 10 µL of each of the CD14 FITC, human leukocyte antigen—DR isotype (HLA-DR) PE, and CD45 PC5 antibodies. The other tube was used as the control and the same 10 µL of antibodies were added. All tubes were placed away from light at room temperature for 15 min after mixing in a whirlpool mixer. Each tube was treated with 900 µL hemolytic agent, shaken evenly, and then placed into a water bath at 37°C for 10 min. CD14+ HLA-DR was used to label myeloid-derived suppressor cells (MDSCs). The number of cells in each sample was more than 10,000 and the assay data were stored in Listmode.
Assay of subtypes of lymphocytes
Whole blood was placed into two tubes, 100 µL per tube. Antibodies against CD4 FITC, CD8 PE, and CD3 PE-Cy5 (10 µL of each) were added to one tube. The other tube was used as the control and the same 10 µL of antibodies were added. All tubes were placed away from light at room temperature for 15 min after mixing in a whirlpool mixer. Each tube was then treated with 900 µL hemolytic agent, shaken evenly, and then placed into a water bath at 37°C for 10 min. CD3+ was used to label total T lymphocytes. CD3+ CD4+ T lymphocytes represent helper T cells. CD3+ CD8+ T lymphocytes represent cytotoxic lymphocytes. The number of cells in each sample was more than 10,000 and the assay data were stored in Listmode.
Statistical analysis
A data bank was established with Excel 2007 and analyzed with SPSS 23.0. Mean ± standard deviation was used to describe quantitative data with normal distribution. A chi-square test was used to compare intergroup differences. If a difference was significant, the Student–Newman–Keuls (SNK) test was used for pairwise comparison. M (P25, P75) was used to describe quantitative data with skewed distribution. A non-parametric test was used to compare intergroup differences. If a difference was significant, pairwise comparison was performed. Pearson’s correlation coefficient was used to measure correlation among variables of quantitative data with normal distribution, while Spearman’s correlation coefficient was used to measure correlation among variables of quantitative data with skewed distribution. P < 0.05 was considered significant.
Results
General characteristics
There were no significant differences in gender or age among the three groups (Table 1).
General information and comparison of subtype cells.

AMI: acute myocardial infarction; UA: unstable angina; NG: normal group.
Significant compared with AMI (P < 0.05).
Significant compared with UA (P < 0.05).
Comparative analysis of cell subtypes
Our results indicated that the ratios of lymphocytes:karyocytes and monocytes:karyocytes as well as those of CD3+ CD4+ T cells, CD14+ CD16– monocytes, CD14+ CD16+ monocytes, and CD11b+ CD68+ monocytes (inflammation-promoting M1 monocytes) were significant in all three groups (P < 0.05).
Ratio of lymphocytes to total karyocytes
The relationship of the ratio of lymphocytes to total karyocytes among the three subgroups can berepresented as NG > UA > AMI, with significantdifferences between the AMI and UA groups as well as between the AMI and NG groups (P < 0.05); however, there was no significant difference between the UA and NG groups (P > 0.05; Figure 1 and Table 1).
Ratios of lymphocytes to total karyocytes.
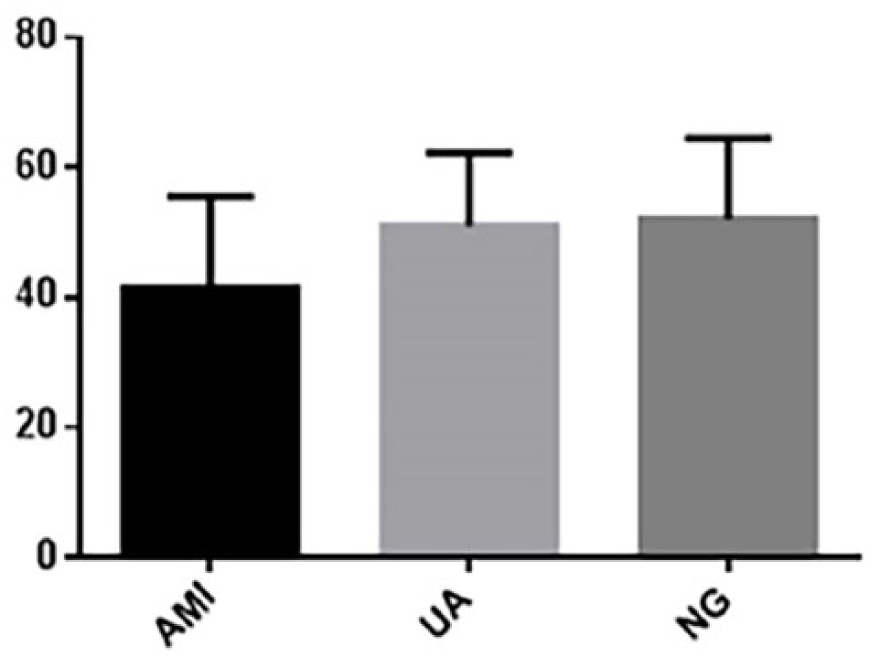
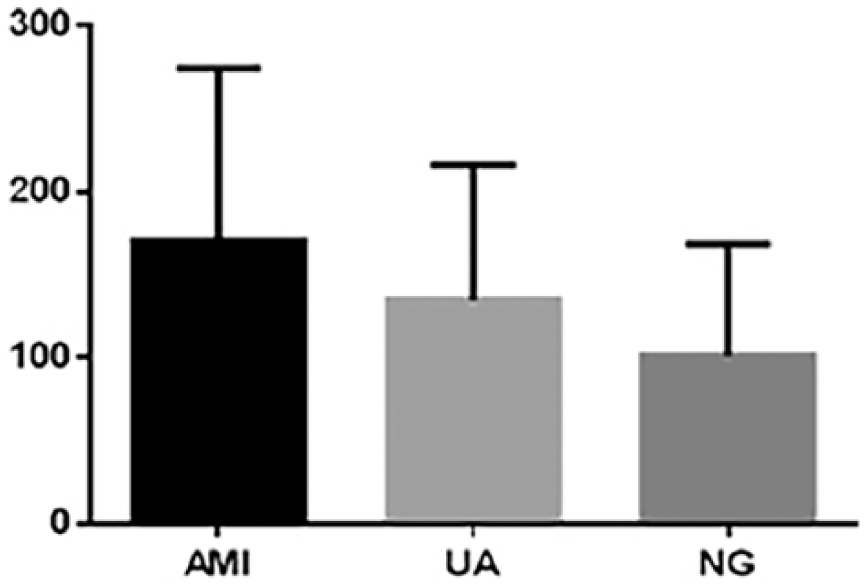
Ratio of T-cell subtypes to total lymphocytes
The relationship of the ratio of T-cell subtypes to total lymphocytes among the three subgroups can be represented as AMI > UA > NG, with a significant difference between the AMI and NG groups (P < 0.05); however, there were no significant differences between the AMI and UA groups or the UA and NG groups (P > 0.05; Figure 2 and Table 1). There were no significant differences in the proportions of CD3+ T cells, CD3+ CD8+ T cells, CD4+/CD8+, CD4+ CD8+, and CD4– CD8– cells among the three subgroups (P > 0.05).

Ratios of CD3+ CD4+ T cells to total lymphocytes.
Ratio of monocyte subtypes to total karyocytes
The relationship of the ratio of CD14+ monocytes to total karyocytes among the three subgroups can be represented as NG > UA > AMI, with a significant difference between the AMI and NG groups (P < 0.05); however, there were no significant differences between the AMI and UA groups or between the UA and NG groups (P > 0.05; Figure 3 and Table 1).
Ratios of CD14+ monocytes to total karyocytes.
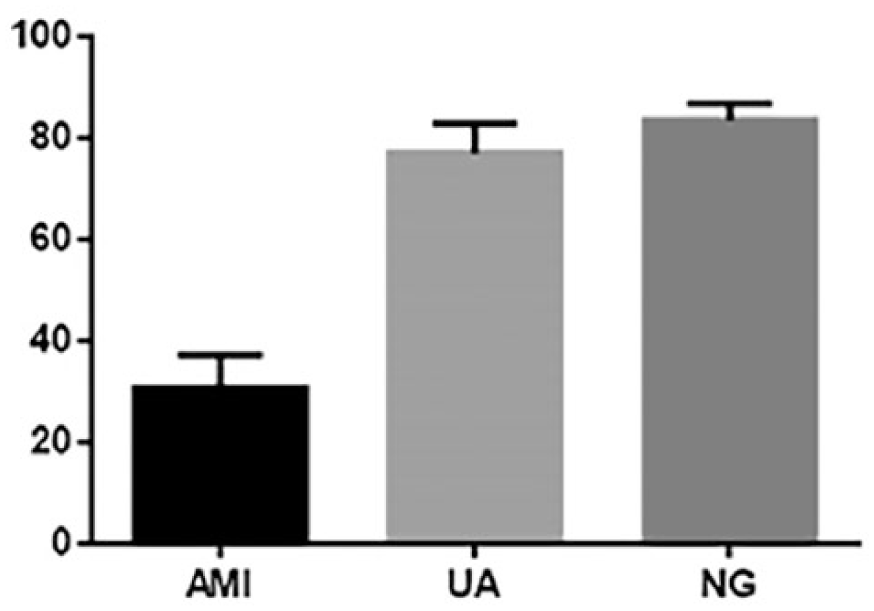
The relationship of the ratio of CD14+ CD16– monocytes to total karyocytes among the three subgroups can be represented as NG > UA > AMI; there were significant differences in pairwise comparisons among the AMI, UA and NG groups (P < 0.05; Figure 4 and Table 1).
Ratios of CD14+ CD16– monocytes to total karyocytes.
The relationship of the ratio of CD14+ CD16+ monocytes to total karyocytes among the three subgroups can be represented as AMI > UA > NG; there were significant differences in pairwise comparisons among the AMI, UA and NG groups (P < 0.05; Figure 5 and Table 1).
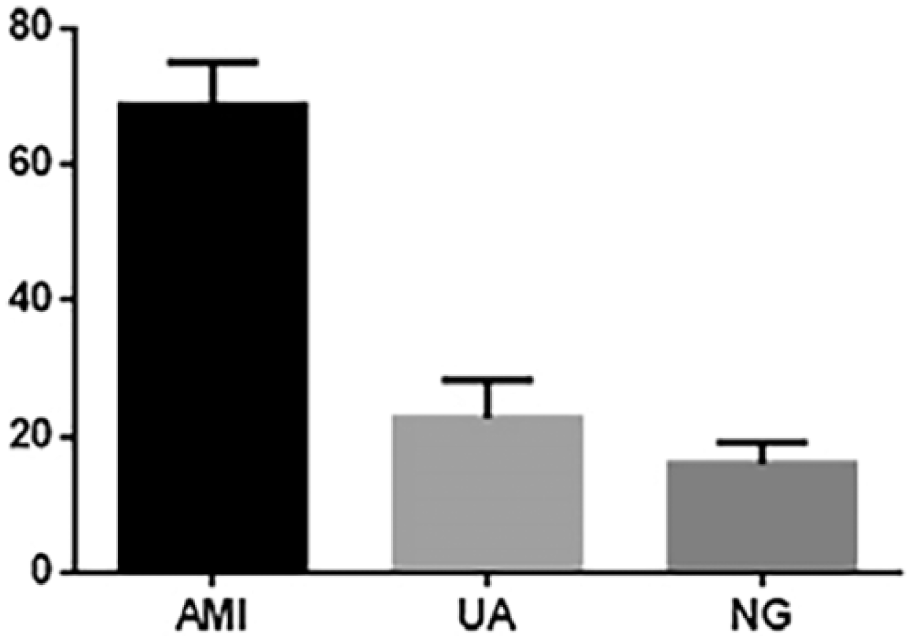
Ratios of CD14+ CD16+ monocytes to total karyocytes.
Subtypes of monocytes
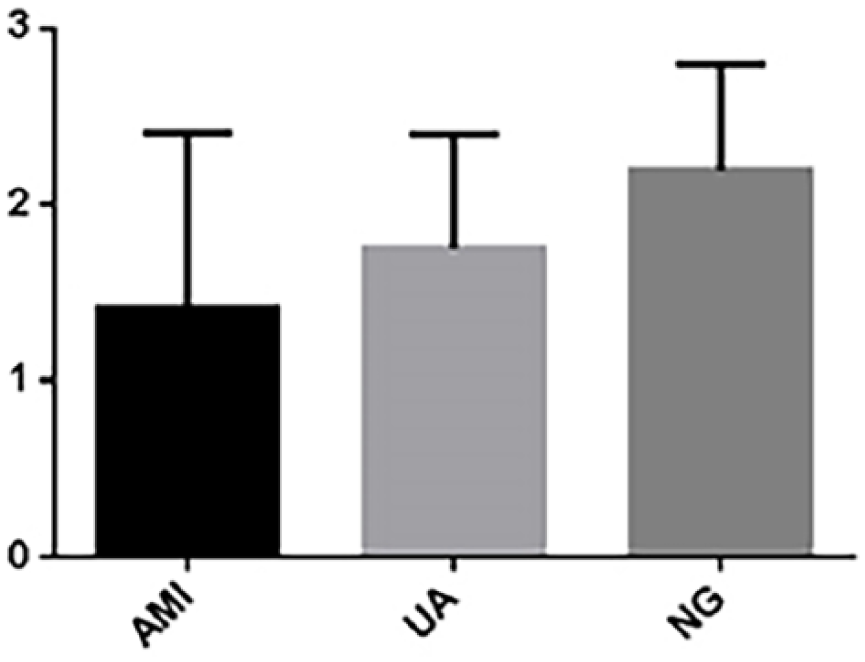
The relationship of the ratio of CD11b+ CD68+ monocytes (inflammation-promoting M1 monocytes) to total karyocytes among the three subgroups can be represented as AMI > UA > NG; there was a significant difference between the AMI and NG groups (P < 0.05); however, there were no significant differences between the AMI and UA groups or between the UA and NG groups (P > 0.05; Figure 6 and Table 1). As shown in Table 1, the ratios of CD11b+ CD206+ monocytes (inflammation-inhibiting M2 monocytes) to total karyocytes were not significantly different among the AMI, UA, and NG subgroups (P > 0.05).
Ratio of CD11b+ CD68+ monocytes to total karyocytes.
MDSCs
There were no significant differences in the proportion of MDSCs, identified as CD14+ HLA-DR–, among the AMI, UA, and NG subgroups (P > 0.05; Table 1).
Discussion
Atherosclerosis is a chronic non-degenerative aseptic inflammation of the arterial wall, in which inflammatory plaques containing a large number of immune cells play a critical role in the cascade response of plaques from vulnerability to rupture.8–10 It has been indicated that, among patients at higher risk of cardiovascular diseases, the percentage of both intermediate and non-classical subtypes is relatively higher, which means that these two subtypes are potential biomarkers of disease severity. 11
In this study, the relationship of the ratios of CD14+ monocytes/total karyocytes in the three subgroups was NG > UA > AMI, among which, compared with NG, the ratio in AMI decreased significantly. It has been demonstrated that there is a dramatic association between monocytes and the development and severity of ACS during the acute stage of MI. The relationship of the ratio of CD14+ CD16– monocytes to total karyocytes among the three subgroups was NG > UA > AMI; for the ratio of CD14+ CD16+ monocytes to total karyocytes, the relationship was AMI > UA > NG. In fact, the sampling in this study was performed at the CAG point after regular diagnosis of ACS including EKG, past history, cTnI, and before PCI. The hyperacute stage of inflammation had been delayed at the sampling point, and consequently the inflammation-promoting and transient classical subtypes had decreased. Nevertheless, compared with healthy subjects, the proportion of CD14+ CD16+ monocytes among patients in both the STEMI and NSTEMI groups increased significantly and was positively associated with the severity of ACS. Meanwhile, the number of differentiated M1 macrophages derived from CD14+ CD16– and CD14+ CD16+ monocytes increased during advanced ACS; hence, the results indicated that the number of CD14+ CD16– subtype monocytes decreased and that of CD14+ CD16+ subtype monocytes increased in patients with STEMI. Recently and interestingly, it has been found that there is a conversion effect of different subtypes of monocytes during the inflammation stage, demonstrating a drift from the classical subtype partly to the intermediate and mostly to the non-classical subtype, based on the results of flow cytometry. 12
The relationship of the ratio of CD11b+ CD68+ monocytes (inflammation-promoting M1 monocytes) to total karyocytes among the three subgroups was AMI > UA > NG; compared with healthy subjects, the proportion of CD11b+ CD68+ monocytes to total karyocytes among patients in the AMI group increased significantly, which indicates, first, that a special functional cell without a clear mechanism between monocytes and macrophages may exist in the peripheral blood, and, second, that monocytes may preferentially differentiate into M1 macrophages during the acute inflammation stage. However, in our study, there were no significant differences in the MDSC population.
Meanwhile, the relationship of the ratio of CD3+ CD4+ T cells to total lymphocytes among the three subgroups was AMI > UA > NG, and, compared with healthy subjects, the proportion of CD3+ CD4+ T cells among patients with AMI increased significantly. There were no significant differences in the proportions of CD3+ T cells, CD3+ CD8+ T cells, CD4+/CD8+, CD4+ CD8+, and CD4– CD8– cells. Based on our findings, we suggest that the adaptive immune response could be closely associated with the instability of ACS plaques.
In summary, CD14+ CD16– monocytes are positively associated with the severity of ACS, while CD14+ CD16+ monocytes are negatively associated with the severity of ACS. M1 macrophages are positively associated with the acute stage of ACS. The adaptive immune response is associated with the instability of ACS plaques and CD3+ CD4+ T cells may play an important role in the early stage of ACS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.