
Abstract
The relationship between carotid atherosclerosis (AS) and levels of serum cathepsin K (CatK) and cystatin C (CysC) on patients with ischemic cerebral vascular disease (ICVD) was explored. In total, 266 patients with ICVD who were admitted in our hospital were enrolled. According to the results of carotid ultrasound, they were randomly divided into plaque group (n = 133) and control group (n = 133). According to atherosclerotic plaque type distribution, the plaque group was divided into stable plaque group and unstable group. The relationship between levels of serum CatK and CysC of two groups and carotid AS indicator (such as intima-media thickness (IMT)) were analyzed with Spearman’s correlation. Spearman’s correlation analysis showed that IMT level was positively correlated with stability of carotid atherosclerotic plaque (P < 0.05). The level of serum CatK in plaque group was significantly higher than control group, and the level of serum CysC in plaque group was significantly lower than control group (P < 0.05); the level of serum CatK in unstable plaque group was significantly higher than stable plaque group, and the level of serum CysC in unstable plaque group was significantly lower than stable plaque group (P < 0.05). Serum CatK and IMT levels were positively correlated, and serum CysC and CatK levels were negatively correlated (P < 0.05). CatK and CysC levels may be used as serum markers for predicting carotid AS plaque instability, providing a new observational index for prevention and treatment of ICVD caused by carotid AS plaque.
Keywords
Introduction
Ischemic cerebral vascular disease (ICVD) is a common nervous system disease of cerebral ischemia and dysfunction. If not treated in time, ICVD will easily develop into a stroke and endanger the patient’s life.
Carotid atherosclerosis (AS) refers to a systemic arterial disease and the arterial wall becomes thicker and less elastic. Carotid intima-media is prone to be involved in AS at the earliest stage, and many studies have shown that carotid AS plays an important role in ICVD, and plaque instability is one of the most important risk factors. 1 It has been reported that cathepsin K (CatK) participates in pathogenesis of AS by regulating the activity of lipid-related enzymes, vascular regeneration, cell migration and invasion, and protein matrix remodeling. 2 Studies have shown that cystatin C (CysC) level in AS plaque is significantly lower than normal arteries, suggesting that CysC may be involved in the pathophysiological process of cardiovascular and cerebrovascular AS. 3
The diagnosis of ICVD mainly depends on imaging method and could not predict the progress of AS and evaluate the stability of plaque. 4 This study is to evaluate the effect of CatK and CysC in ICVD by analyzing the levels of serum CatK and CysC in patients with ICVD and the correlation with cervical AS for clinical reference.
Materials and methods
Study subject
In total, 266 patients with ICVD who were admitted in our hospital were enrolled. According to the results of carotid ultrasound, they were randomly divided into plaque group (n = 133) and control group (n = 133). Inclusive criteria were as follows: ICVD diagnosis conforms to the diagnostic criteria set by the Fourth National Conference on Cerebrovascular Diseases, ICVD has been confirmed by brain computed tomography (CT)/magnetic resonance imaging (MRI), and all patients have signed informed consent form. Exclusive criteria were as follows: hemorrhagic stroke; familial hypertension; other serious organic diseases such as liver, kidney, or lung; malignant tumor; acute or chronic infection; myocardial infarction; peripheral vascular occlusive disease; immune diseases; patients taking inflammatory inhibitors, immunosuppressants, hormones, or other drugs that may affect the levels of CatK and CysC; and women in pregnancy and lactation or under taking long-term contraceptives. This study has been approved by the ethics committee in the hospital.
Data collection and serum biochemical indices detection
General clinical data of two groups, including age and sex, were recorded. Fasting venous blood samples from two groups of patients were taken. OLYMPUS AU2700 automatic biochemical analyzer (Japan) was adopted to analyze fasting blood glucose (FBG), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), lipoprotein a (Lp (a)), and uric acid (UA). Serum CysC level was determined with particle-enhanced immunoturbidimetry (Sichuan Xincheng Biotechnology Co., Ltd., Sichuan Food and Drug Machinery (approval) Word 2012 No.240229, Sichuan, China). Serum CatK level was determined with enzyme-linked immunosorbent assay (ELISA) method (K141-100; Shanghai Qiyi Biotechnology Co., Ltd, Shanghai, China).
Carotid intima-media thickness measurement
Carry out carotid artery ultrasound to test intima-media thickness (IMT) of ICVD patients within 72 h after hospitalization by three experienced doctors. Use ACUSON Sequoia 512 (USA) doppler ultrasound instrument to examine at 7.5 MHz. Scanning steps were as follows: use the probe to transversely cut the carotid artery, which showed the short-axis image, placed in the middle of the image; closely watch the short-axis carotid artery and slowly rotate the probe to make it a long-axis image and get the maximum section; use the probe to observe the carotid artery anterior wall, posterior wall, IMT abrasion, and internal echo from bottom to top; and when sliding from head side to the bifurcation of internal carotid artery and external carotid artery, pay more attention to this position. Because of the anatomical structure specificity of this position, it affects the blood flow and it is easy to make intima thickening, sclerosis, and form plaque. Finally, trace the thickness and internal echo of the internal carotid artery and external carotid artery. After obtaining clear two-dimensional ultrasound images, automatically measure the IMT of bilateral common carotid artery, internal carotid artery, and external carotid artery; take average value of the three IMT as common carotid artery IMT; and judge the atherosclerotic plaque type based on internal echo of the carotid artery. According to the shape and echo characteristics of plaques under ultrasound, divide plaques into hypoechoic lipid soft plaques, medium echogenic collagen-rich fibrous flat plaques, hyperechoic calcified hard plaques, and ulcerative mixed plaques with different echo intensity. Soft plaques, flat plaques, and ulcerative mixed plaques belong to unstable plaques.
Statistical analysis of data
Use statistical software package SPSS 19.0 software system (IBM, Chicago, IL, USA) to analyze and process the data. Express measurement data as (
Results
Comparison of general clinical data of two groups
There were no significant differences in sex, hypertension history, diabetes mellitus history, smoking, drinking, FBG, TG, TC, HDL-C, and LDL-C between the plaque group and control group (P > 0.05). There were significant differences in age, diabetes mellitus history, serum Lp (a), and homocysteine (Hcy) levels (P < 0.05). The average age of plaque group was significantly higher than control group, and the number of patients with diabetes mellitus history in plaque group was significantly higher than control group. The serum Hcy and Lp (a) levels in plaque group were significantly higher than control group (P < 0.05; Table 1).
General clinical data.

FBG: fasting blood glucose; TC: total cholesterol; TG: triglyceride; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; Lp (a): lipoprotein a; Hcy: homocysteine.
IMT level and distribution of carotid atherosclerotic plaques
The IMT of plaque group (1.53 ± 0.12) was significantly higher than the control group (0.92 ± 0.14; P < 0.05; Figure 1(a)). The coefficient of variation (CV) of the plaque group and control group was 7.84% and 7.61%, respectively, with no significant difference (P > 0.05). Among the 133 patients with plaque, there were 27 (20.30%) cases of hypoechoic lipomatous soft plaques, 44 (33.08%) cases of fibrous flat plaques, 36 (27.07%) cases of calcified hard plaques, and 26 (19.55%) cases of ulcerative mixed plaques. Therefore, there were 36 (27.07%) cases of stable plaques and 97 (72.93%) cases of unstable plaques. Besides, there were 68 cases (51.13%) of left carotid artery plaques and 64 (48.12%) cases of right carotid artery plaques. A total of 27 cases (20.30%) were tested cavity stenosis, including 10 mild cases (7.52%), 16 moderate cases (12.03%), and 2 severe cases (1.5%). According to the distribution of atherosclerotic plaque types, divide plaque group into stable plaque group and unstable plaque group. The IMT level of stable plaque group was 1.25 ± 0.41 mm, and IMT level of unstable plaque group was 1.77 ± 0.72 mm. The IMT level of unstable plaque group was significantly higher than stable plaque group (Figure 1(b)). Set assignment value of stable plaque as 1 and assignment value of unstable plaque as 2. Spearman’s correlation analysis showed that IMT level was positively correlated with the stability of carotid atherosclerotic plaque. The IMT level is higher, and the carotid atherosclerotic plaque stability is worse (P < 0.05; Figure 2).
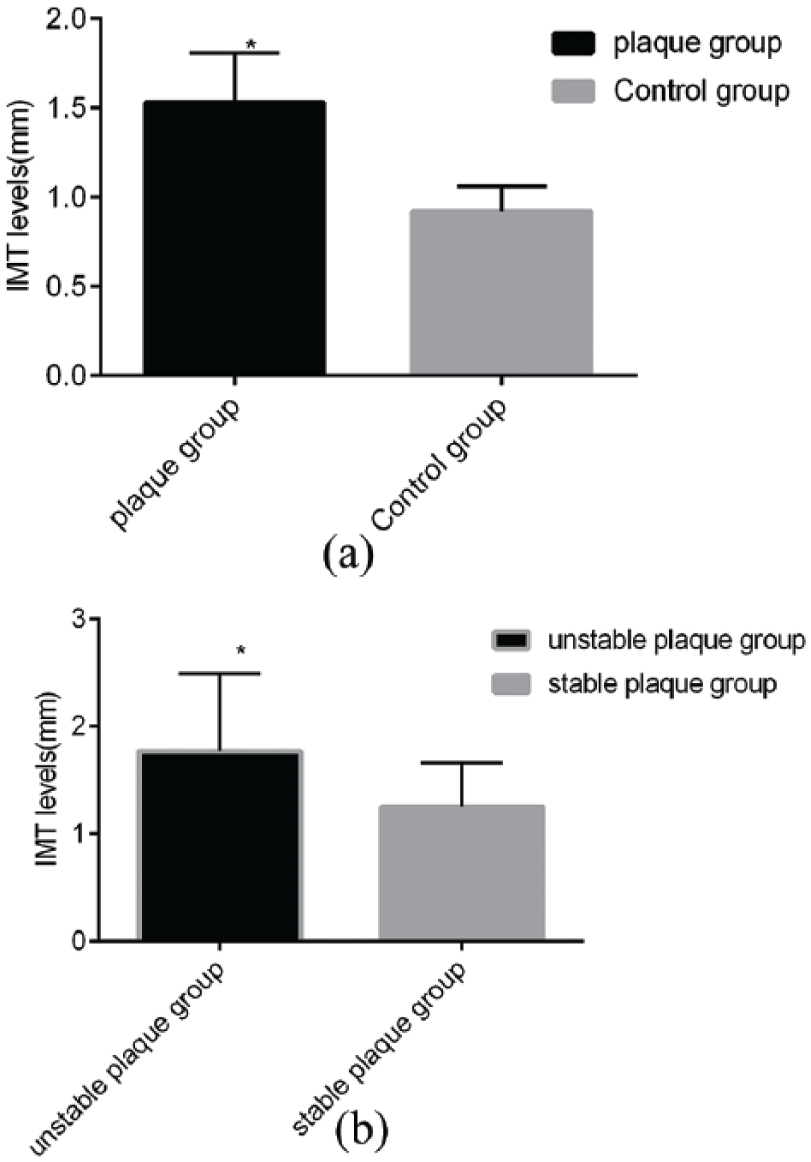
Comparison of IMT levels: (a) comparison of IMT level between plaque group and control group: IMT of carotid artery in plaque group and control group was measured by ultrasound. The results showed that IMT in plaque group was significantly higher than that in control group (P < 0.05) and (b) comparison of IMT levels between stable plaque and unstable plaque. The results showed that the level of IMT in unstable plaque group was significantly higher than that in stable plaque group (P < 0.05).
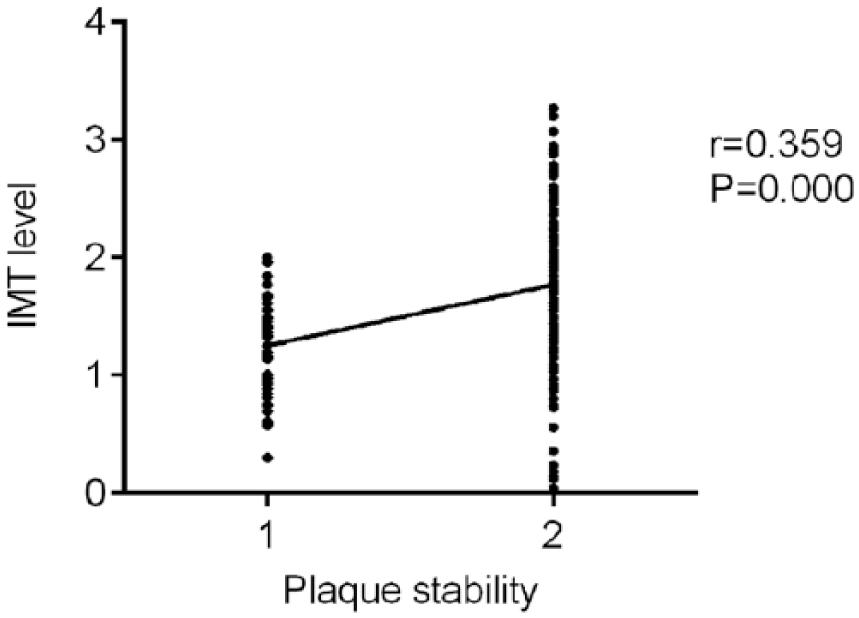
Spearman’s correlation analysis between IMT and atherosclerotic plaque type.
Correlation analysis of levels of serum CatK and CysC and IMT
The serum CatK levels in plaque group and control group were 19.35 ± 0.58 ng/L and 17.23 ± 0.38 ng/L, respectively. Inter- and intra-CV of plaque group and control group was 3.00% and 11.54% and 2.21% and 10.87%, respectively, with no significant difference (P < 0.05). The serum CysC level in plaque group and control group were 0.76 ± 0.06 mg/L and 1.18 ± 0.11 mg/L, respectively. Inter- and intra-CV of plaque group and control group was 7.89% and 13.21 % and 9.32% and 15.75%, respectively, with no significant difference (P < 0.05). The serum CatK level of plaque group was significantly higher than control group, and the serum CysC level of plaque group was significantly lower than control group (P < 0.05; Figure 3(a)). According to the distribution of atherosclerotic plaque types, divide plaque group into stable plaque group and unstable plaque group. Analyze relationship between the levels of serum CatK and CysC and the stability of atherosclerotic plaque. Serum CatK level of unstable plaque group was 20.87 ± 2.16, which was significantly higher than control group of 18.54 ± 1.17; the serum CysC level of unstable plaque group was 0.83 ± 0.33, which was significantly lower than control group of (0.66 ± 0.17; P < 0.05; Figure 3(b)). Pearson’s correlation analysis of serum CatK and IMT level indicated that serum CatK and IMT levels were positively correlated (P < 0.05; Figure 3(c)); Pearson’s correlation analysis of serum CysC and IMT level indicated that serum CysC and IMT levels were positively correlated (P < 0.05; Figure 3(d)). Pearson’s correlation analysis of serum CysC and CatK levels showed that serum CysC and CatK levels were negatively correlated (P < 0.05; Figure 3(e)).

Serum levels of CatK and CysC: (a) serum levels of CatK and CysC in plaque group and control group: serum CatK level in plaque group was significantly higher than that in control group, and serum CysC level was significantly lower than that in control group (P < 0.05); (b) comparison of serum CatK and CysC levels with plaque stability: when the relationship between serum CatK and CysC levels and the stability of atherosclerotic plaque was analyzed, it was found that the serum CatK level in unstable plaque group was significantly higher than that in stable plaque group, and the serum CysC level in unstable plaque group was significantly lower than that in stable plaque group (P < 0.05); (c) serum CatK and IMT levels Pearson correlation analysis: the Pearson correlation analysis of serum CatK and IMT levels showed that there was a positive correlation between serum CatK and IMT levels (P < 0.05); (d) serum CatK and IMT levels Pearson correlation analysis: Pearson correlation analysis between serum CysC level and IMT level showed that serum CysC level was negatively correlated with IMT level (P < 0.05); and (e) serum CatK and CysC level levels Pearson correlation analysis: the Pearson correlation analysis between serum CysC level and CatK level showed that there was a negative correlation between serum CysC level and CatK level.
Discussion
Various studies have shown that Hcy of AS endothelial vascular tissue is significantly higher than normal endothelial tissue. 5 This research found that the level of serum Hcy in plaque group was significantly higher than control group.
It is found that CysC deficiency can promote the formation of AS in mice, 3 which is consistent with the results of this study. The mouse experiment verified the relationship between CysC and AS in the animal model again and explained that CysC may affect AS by regulating autophagy. CatK can degrade collagen and elastin and participate in vascular remodeling. 6
It has been reported that AS is mediated by inflammation. 7 Inflammatory substances can stimulate vascular elastin damage area to produce CatK and inhibit the expression of CysC, so the imbalance of CysC and CatK levels is one of important reasons for causing AS.
Currently, there are still no unified evaluation criteria on carotid plaque stability, and carotid ultrasound is often used to evaluate. This study found that serum CysC and CatK levels were closely related with IMT and plaque properties, but whether serum CysC and CatK levels could be used as biological indicators still needs to be verified by prospective experiment with more samples and multiple centers.
There are some deficiencies in this study. We did not observe dynamically the changes of the factors during and after treatment. Second, the results of carotid ultrasound examination may be different due to the doctors’ experience. In addition, small sample size limited the correctness of the results.
In conclusion, CatK and CysC levels may be used as serum indicators for predicting plaque instability in carotid AS.
Footnotes
Acknowledgements
A randomized controlled study of the safety and efficacy of staging angioplasty and primary stenting in patients with high perfusion risk of carotid artery stenosis (2014015).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.