
Abstract
The characteristics of distribution of Pseudomonas aeruginosa in patients with agranulocytosis and fever in 12 hospitals in Shanghai from 2012 to 2014 were retrospectively analyzed. WHONET 5.6 software was used to analyze the results of drug sensitivity test. Data from different diseases, different sample sources, and drug sensitivity tests were statistically analyzed to investigate the clinical distribution characteristics and drug resistance of Pseudomonas aeruginosa in patients with agranulocytosis and fever in Shanghai, China. This study revealed that, among these 109 strains of P. aeruginosa, they were mainly found in patients with acute myelocytic leukemia (AML; 48 strains, 44.04%) and patients with acute lymphocytic leukemia (ALL; 36 strains, 33.03%). The specimen sources were mainly respiratory tract secretions (58 strains, 53.21%) and blood (21 strains, 19.26%). The P. aeruginosa isolates from neutropenic sepsis patients showed high sensitivity to the following antibiotics: piperacillin/tazobactam, cefepime, ciprofloxacin, ceftazidime, and amikacin with 91.1%, 89%, 89%, 87.9%, and 85.7% of isolates being sensitive, respectively. Furthermore, for P. aeruginosa isolates from the AML group of patients, the lowest antibiotic resistance rates were seen for ciprofloxacin (0%), cefoperazone/sulbactam (2.1%), and cefepime (7.1%), while for the ALL group the lowest antibiotic resistance rates were seen for piperacillin (2.8%), ceftazidime (2.8%), and cefepime (2.8%). Isolates from AML patients (21.3%) were significantly more likely to be piperacillin resistant than those from the ALL patients (2.8%). Therefore, P. aeruginosa infection is relatively common in patients with agranulocytosis and fever. The strains had a certain degree of resistance to commonly used antibiotics.
Introduction
Hematologic patients with neutropenia have a high risk in morbidity of severe infections due to persistent neutropenia, immunosuppression of cells and/or body fluids, and barrier destruction for both the skin and mucous membrane. 1 It not only increases mortality, but also jeopardizes the overall disease prognosis. Hence, it is exactly necessary to perform appropriate antibiotic treatment in time. The proper choice of initial empirical anti-infective treatment needs to consider the patient’s clinical characteristics and epidemiological data of pathogenic microorganism and drug resistance. 2 Pseudomonas aeruginosa acts as one of the common opportunistic pathogens in immunocompromised patients and one of the main etiologies of hospital infections. Due to the extraordinary adaptability 3 and anti-multiple antibiotic mechanism 4 provided by P. aeruginosa strains, these induced infections may be life-threatening and a worldwide public health imperil. 5 At present, there is a lack of epidemiological data focused on P. aeruginosa in blood-borne patients with neutropenia and fever in the general population. Therefore, this study investigated and analyzed the distribution characteristics and drug resistance prevalence of P. aeruginosa in patients with neutropenia and fever, who were admitted in 12 hospitals in Shanghai, China.
Materials and methods
Strain resources
Strains were extracted from patients with neutropenia and fever, who were admitted in hematology wards in 12 hospitals in Shanghai for the period of 2012–2014. Overall, 1260 strains were detached. Among these strains, 109 strains were P. aeruginosa. All subjects gave informed, signed consent to participate in the study.
Diagnostic criteria
Neutropenia refers to the peripheral blood absolute neutrophil count (ANC) of <0.5 × 109/L or predicted ANC of <0.5 × 109/L after 48 h in patients. Severe neutropenia is defined as the ANC of <0.1 × 109/L. Fever refers to the oral temperature per measurement of ⩾38.3°C (axillary temperature ⩾ 38.0°C) or ⩾38.0°C (axillary temperature l37.7°C) for more than 1 h. 6
Culture, checkup, and drug-sensitive testing for bacteria
The segregation, checkup, and drug-sensitive analysis of strains were entirely according to “National Clinical Lab Protocols.” The segregation underwent a drug-sensitive test, according to the Clinical and Laboratory Standards Institute (CLSI) 2014 KGB (K-B). The quality control strains were Escherichia coli ATCC25922 and P. aeruginosa ATCC27853, respectively, which were finally judged according to the CLSI 2014 version. 7 Blood samples were simultaneously collected from two sites, particularly the catheter and other parts of the vein, for patients who underwent central venous catheterization. The positive bacterial culture of inpatients in these hematology wards were selected from January 2012 to December 2014, while the level of granulocytes in peripheral blood and maximum body temperature were presently looked up. The strain data of patients accorded with the diagnosis of neutropenia and fever, which were screened out.
Statistical methods
Drug resistance results were analyzed using WHONET 5.6 software, while other results were analyzed by SPSS 19.0 software. The proportions were demonstrated in percentage, while classified variables were compared by Pearson’s chi-square test when all theoretical number T was ⩾5 and the total sample size n was ⩾40. Continuously corrected chi-square test was used when the theoretical number T was <5, but T was ⩾1 and n was ⩾40. Fisher’s test was performed when the number of theoretical T was <1 or n was <40. P < 0.05 was considered statistically significant.
Results
Strain test results
From January 2012 to December 2014, a total of 1260 validated strains were detached from patients with neutropenia and fever. Among these strains, 109 (8.65%) stains were positive for P. aeruginosa, which was ranked fourth among all specimens. These 109 patients comprised 56 male and 53 female patients.
Specimen distribution features
Among these 109 P. aeruginosa strains, 48 (44.04%) cases were acute myelocytic leukemia (AML), 36 (33.03%) were acute lymphocytic leukemia (ALL), 7 were non-Hodgkin’s lymphoma, 6 (5.50%) were myelodysplastic syndrome (MDS), 6 (5.50%) were aplastic anemia (AA), and 4 (3.67%) were Hodgkin’s lymphoma tumors. Furthermore, two strains (1.83%) were multiple myeloma, as depicted in Table 1.
Specimen distribution features among these 109 Pseudomonas aeruginosa strains.
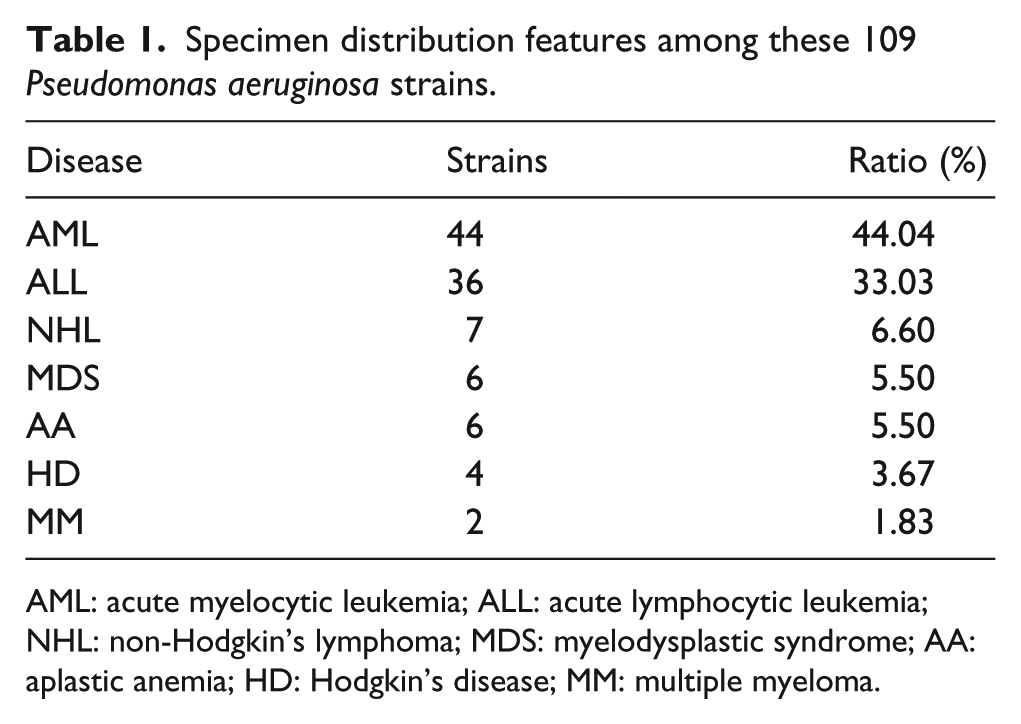
AML: acute myelocytic leukemia; ALL: acute lymphocytic leukemia; NHL: non-Hodgkin’s lymphoma; MDS: myelodysplastic syndrome; AA: aplastic anemia; HD: Hodgkin’s disease; MM: multiple myeloma.
Sample source distribution
In total, 58 strains (53.21%) were detached from respiratory secretions, 21 strains (19.26%) were detached from blood, 12 strains (11.01%) were detached from wound secretions, and 18 strains (16.51%) were from the other samples, as illustrated in Table 2. P. aeruginosa strains isolated from respiratory tract secretions and blood ranked fourth (both 10%) in strains in these samples.
Sample source distribution among these 109 Pseudomonas aeruginosa strains.

Drug resistance test results
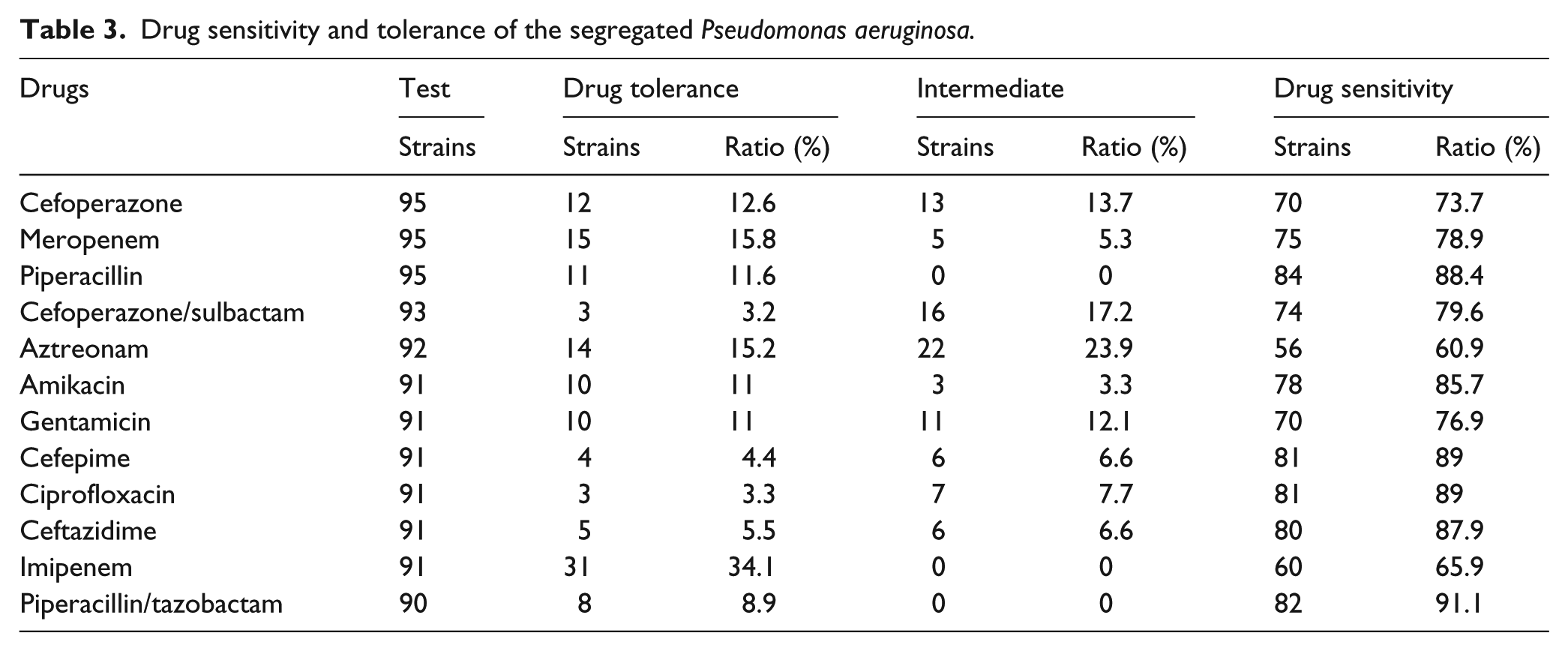
The P. aeruginosa isolates exhibited a lower sensitivity to aztreonam and imipenem, which were 60.9% and 65.9%, respectively. On the contrary, the sensitivity to piperacillin/tazobactam, cefepime, and ciprofloxacin were relatively high and the sensitivity rates were 91.1%, 89%, and 89%, respectively. In addition, sensitivity rates to other antibacterials such as meropenem, piperacillin, cefoperazone/sulbactam, amikacin, gentamicin, and ceftazidime were all above 75%, as shown in Table 3. This reveals that piperacillin and imipenem had significantly different resistance rates for P. aeruginosa between AML and ALL (P < 0.05), while no significant difference was observed in drug resistance rates for the other general antibacterials (P > 0.05), as shown in Table 4. Furthermore, there was no significant difference in resistant rates for general antibacterials between respiratory secretions and blood samples (P > 0.05). Moreover, no resistant bacteria emerged in respiratory secretions and blood samples. No neither for the cefoperazone/sulbactam, rhinophila, aztreonam, cefoperazone, ceftazidime, cefepime, amikacin, gentamicin, and ciprofloxacin appeared in blood samples; for details see Table 5.
Drug sensitivity and tolerance of the segregated Pseudomonas aeruginosa.
Comparison of drug resistance among different diseases.

AML: acute myelocytic leukemia; ALL: acute lymphocytic leukemia.
Comparison of drug resistance among different samples.

Discussion
This study retrospectively analyzed 109 strains of P. aeruginosa detached from inpatients in 12 hospitals in Shanghai, who suffered from neutropenia and fever from 2012 to 2014. Judging from these results, P. aeruginosa ranks fourth among both all specimen strains (8.65%) and gram-negative bacteria (13.19%). Furthermore, P. aeruginosa ranks second for non-fermentative Gram-negative bacilli.
Among patients with P. aeruginosa infection, AML and ALL patients accounted for 44.04% and 33.03%, respectively. P. aeruginosa were detached from respiratory tract secretions (53.21%), blood (19.26%), and wound secretions (11.01%). Drug sensitivity analysis revealed that the rates of P. aeruginosa resistance to aztreonam, meropenem, and imipenem were 15.2%, 15.8%, and 34.1%, respectively. The sensitivity rates of piperacillin/tazobactam, cefepime, and ciprofloxacin were all relatively high, which were 91.1%, 89%, and 89%, respectively. Statistical analysis results revealed that the differences in the resistance rates of P. aeruginosa to piperacillin and imipenem in AML and ALL among different diseases were statistically significant (P < 0.05), and both had high drug resistance rates in AML (21.3% and 57.1%, respectively). Furthermore, there was no significant difference in resistance rates to common antibacterials among respiratory secretions and blood samples (P > 0.05). There were no resistant bacteria in the respiratory secretions and blood samples with cefoperazone/sulbactam. In addition, none of the blood isolates were resistant to the antibiotics, for example, meropenem, aztreonam, cefoperazone, ceftazidime, cefepime, amikacin, and gentamicin. It was considered that this may be related to the high sensitivity of these drugs in the bloodstream infected with P. aeruginosa, or the number of blood samples was too small. Based on the above analysis, the initial empirical treatment of patients associated with fever should pay attention to cover P. aeruginosa, especially during the empirical use of carbapenem-based drugs, especially imipenem in patients with uncontrolled infection, but in the absence of etiological evidence, taking into account the possibility of non-fermentative bacteria such as P. aeruginosa, the anti-infective can be adjusted to piperacillin/tazobactam, cefepime, cefoperazone/sulbactam, or combined ciprofloxacin and amikacin. It is suggested that imipenem and piperacillin should not be applied to the AML neutropenic patients infected by P. aeruginosa.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.