
Abstract
This study was to investigate the feasibility and safety of patient-controlled intravenous analgesia for opiate titration in patients with severe cancer. Eligible patients with cancer pain were randomly divided into two groups, which were titrated with a subcutaneous injection of morphine and patient-controlled intravenous analgesia, respectively. The time required for patients to begin titration to reach visual analog scale score ⩽ 3, the adverse reactions during titration, the time spent by nurses in titrating each patient, and the time to complete the titration with a delayed-release dosage form analgesic effect and adverse reaction. The mean titration time of patient-controlled intravenous analgesia group (1.09 ± 0.82 vs 2.97 ± 1.98) and morphine dosage (18.78 ± 12.32 vs 13.23 ± 8.07) were significantly lower than those in the subcutaneous group (P < 0.05). The incidences of nausea, vomiting, pruritus, urinary retention, and sedation in the subcutaneous injection group were significantly lower than those in the subcutaneous injection group (P < 0.05). The assessment times of the two groups (10.19 ± 3.72 vs 10.25 ± 4.88) were similar (P > 0.05). However, the time required for subcutaneous injection in patients under patient-controlled intravenous analgesia was significantly lower than that in the subcutaneous injection group (36.36 ± 12.15 vs 132.36 ± 32.79), which was statistically significant (P < 0.05). After the titration, the controlled release opioid was used to treat cancer pain. The visual analog scale score of the patient-controlled intravenous analgesia group was significantly lower than that of the subcutaneous group (2.44 ± 1.37 vs 2.73 ± 0.91) at 7 days after treatment in the subcutaneous group (1.05 ± 0.30 vs 2.45 ± 1.29; P < 0.05). Patient-controlled intravenous analgesia technique can effectively and quickly complete the titration of cancer pain treatment with less occupational care resources and is better than the subcutaneous injection titration.
Keywords
Introduction
Dose titration is required prior to the first opiate or tolerant patient opiate adjustment in non-tolerant patients. 1 For severe pain patients with a visual analog scale (VAS) score ⩾ 7, titration is usually performed by subcutaneous or intravenous injection. 2 The subcutaneous and intravenous injections by a nurse executive will require a great deal of care and a long time. Patient-controlled analgesia (PCA) can be given by the patient according to the degree of pain. The principle of PCA is to allow the patient to choose when to administer a bolus of an analgesic, with the clinician prescribing the bolus dosage and the lockout period between the two boluses. The patient is no longer dependent on the evaluation method or the uncertain availability of staff. PCA corresponds to the principle of continuous intravenous titration of analgesic doses required for each patient, potentially resolving both the methodological difficulties of evaluating pain and the pharmacological problems linked to the use of analgesics like opioids. Small dose, multiple self-administrations, and the previous treatment for postoperative pain show good curative effect and safety while significantly reducing the workload of the nurse, so that patients can get better and faster pain relief. 3
However, PCA technology can be used for cancer pain opioid dose titration it? To this end, we examined opioid titration for cancer pain with subcutaneous injection of morphine (SIOM) and morphine patient-controlled intravenous analgesia (PCIA) to see if PCIA could be used to safely and efficiently to complete opiate titration.
Patients and methods
Patients
In total, 186 patients with severe cancer who were treated in our hospital from June 2015 to June 2017 were randomly divided into SIOM group and PCIA group by random number table method. The SIOM group contained 97 cases including 52 males and 45 females, with age 52.1 ± 10.2 years, body mass index (BMI) of 22.3 ± 0.5 kg/m2, and VAS score of 84.6 ± 1.2 points. There were respiratory system tumors in 25 cases, digestive system tumors in 42 cases, gynecologic tumors in 15 cases, and other systemic tumors in 15 cases. There were 50 males and 39 females in the PCIA group, with a mean age of 51.9 ± 9.8 years, a BMI of 22.6 ± 0.9 kg/m2, and a mean VAS score of 84.5 ± 1.0 points, including 22 cases of respiratory system tumors, 40 cases of digestive system tumors, 18 cases of gynecological tumors, and 9 cases of other system tumors. The inclusion criteria contained patients with numerical rating scale (NRS) score ⩾ 7, body weight ⩾ 50 kg, no opioid contraindication, no severe heart, lung, liver, kidney, or other important organ dysfunctions, no mental disorders, and those who can be treated by subcutaneous or intravenous injection,. The subjects who exhibited severe opioid-related complications, cannot be relieved by symptomatic treatment, changed to other analgesia methods, and changed in condition were excluded. All patients signed informed consent and the test process was in line with the principles of human ethics. This study was approved by the ethics committee in our hospital. There was no significant difference between the two groups in baseline data (P > 0.05).
Methods
Subcutaneous injection of 5 mg morphine (Northeast Pharmaceutical Group Shenyang First Pharmaceutical Co., Ltd, H20013351) was performed. The pain was assessed after 30 min and the titration dose was given according to the degree of pain until VAS score < 3 (see Table 1 for the dose adjustment principle), at which point the cumulative dose of morphine was administered subcutaneously at a rate of 4 h/time. Within 4 h of the medication interval, if the VAS score is >3, rescue dose may be given, and the rescue dose was one-tenth of the total amount for 24 h (every 4-h dosage × 6) until the VAS score is ⩽3 in accordance with the principle of titration. The titration was finished at 24 h after the total amount of morphine converted to controlled release opiate drug administration. Titration process, such as serious adverse reactions, and NRS ⩽ 3, should be considered titration dose down regulate 25%, while giving symptomatic treatment of adverse reactions.
The reference standard of dose titration increase depending on VAS score.

In this study, VAS score ⩾ 7, 50% increase in dose; 3 < VAS score < 7, dose increase of 25%; VAS score ⩽ 3, dose unchanged.
In the PCIA group patients with PCIA titration, the concentration of morphine in the PCA pump storage bag is 0.5 mg/mL, the loading dose of morphine is 5 mg, the bolus dose of morphine injection is 2 mg/time, the lockout time is 15 min, and the maximum limit of 40 mg for 4 h. Pre-titration church patients used VAS for pain assessment and self-administered PCA pump administration. The pain was evaluated by a nurse using VAS at 15 min after the loading dose was given. For example, if the VAS score is >3, the patient pressed the PCA pump button and was given the bolus dose. At 15 min after the bolus dose administration, if the VAS score is >3, the patient can call a nurse and will be given the bolus dose again. After the administration of bolus dose, if the VAS score is ⩽3, then there is no longer administration until the patient NRS score is >3, the patient presses the PCA button again. The process was repeated to maintain the patient’s VAS score ⩽ 3 at 24 h after the cumulative dose of morphine converted to controlled release formulations. If the patient effectively presses the PCA button three times in continuous 15 min after the PCA button is administered, still with VAS score > 3, the PCA pump bolus dose needs to be adjusted by the healthcare provider and the titration continues. The bolus dose adjustment principle was that the bolus dose is increased by 50% for VAS score ⩾ 7 and by 25% for 3 < VAS score < 7; nurses and patients are involved in each pain assessment and nurses do not intervene in the patient’s pain assessment and controlled drug delivery, titration was stopped by the nurse only when the patient developed a serious adverse reaction, and the doctor was advised to perform rescue. Patients with VAS score ⩾ 7 during titration and for more than 12 h, the SIOM can be changed to PCIA titration, and the PCIA group may consider compound ketamine or other auxiliary drugs (antineuropathic pain drugs such as lidocaine), while exiting the study.
Observation index
All patients underwent titration during blood pressure, electrocardiography (ECG), respiratory rate, heart rate, and pulse oxygen saturation monitoring. The VAS score was used for pain assessment, with 0 indicating no pain and 100 indicating the most severe pain. Patients treated by SIOM were evaluated 30 min after each dose and in the event of an outbreak of pain they were evaluated immediately. Patients in the PCIA group were evaluated for pain 15 min prior to each administration and on their own; once the titration was completed, a routine assessment of pain was performed daily, with pain assessment of any episodes of pain occurring at any time; observation and recording of titrations were made from the beginning of titration to VAS score < 3 The time required, the cumulative amount of morphine consumed by each patient at the end of titration, and the patient’s satisfaction with titration therapy were assessed by digital simulation.
Statistical method
The data were analyzed using SPSS 17.0 software. The measurement data were presented as mean ± standard deviation (x ± s) and compared using t test. Enumeration data were compared by the X2 test or Fisher’s exact probability method. P < 0.05 was considered as statistically significant.
Results
Patients’ titration results and satisfaction results
The difference was statistically significant (P < 0.05) between the PCIA group and the subcutaneous injection group with respect to the mean titration time (1.09 ± 0.82 vs 2.97 ± 1.98) and morphine dosage (18.78 ± 12.32 vs 13.23 ± 8.07). The satisfaction rate of patients in the PCIA group was significantly higher than that in the morphine group, and the difference was statistically significant (P < 0.05; Table 2). After treatment, the incidences of adverse reactions, such as nausea, vomiting, pruritus, urinary retention, and sedation in the PCIA group were significantly lower than those in the SIOM group (P < 0.05; Table 3). The duration of the pain assessment and subcutaneous injection by the nurse during titration.
Titration results of two different titration methods (x ± s).

NRS: numerical rating scale; SIOM: subcutaneous injection of morphine; PCIA: patient-controlled intravenous analgesia.
Two groups of patients after treatment incidence of adverse reactions (n).

SIOM: subcutaneous injection of morphine; PCIA: patient-controlled intravenous analgesia.
Data analysis showed that there was no significant difference between the two groups (10.19 ± 3.72 vs 10.25 ± 4.88) during titration (P > 0.05). However, the time required for subcutaneous injection in PCIA patients was significantly lower than that in the morphine group (36.36 ± 12.15 vs 132.36 ± 32.79, P < 0.05; Table 4). Evaluation of analgesic effect and satisfaction of titration post-controlled Release Opiate.
Evaluation of nurses during titration and pain assessment and time required to complete subcutaneous injection (x ± s).
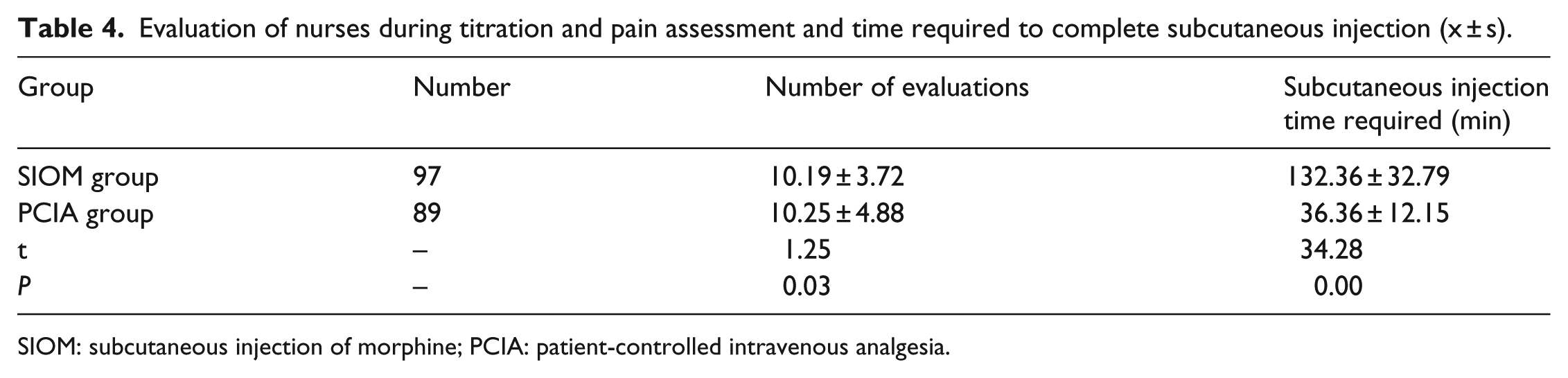
SIOM: subcutaneous injection of morphine; PCIA: patient-controlled intravenous analgesia.
After completion of the titration, instead of using a controlled release opioid for the treatment of cancer pain, the VAS score was significantly lower at 7 days after PCI in the PCIA group than in the SIOM group (2.44 ± 1.37 vs 2.73 ± 0.91). Morphine injection group (1.05 ± 0.30 vs 2.45 ± 1.29) was statistically significant (P < 0.05; Table 5).
Titration after controlled release opioid analgesic effect and satisfaction evaluation (x ± s).
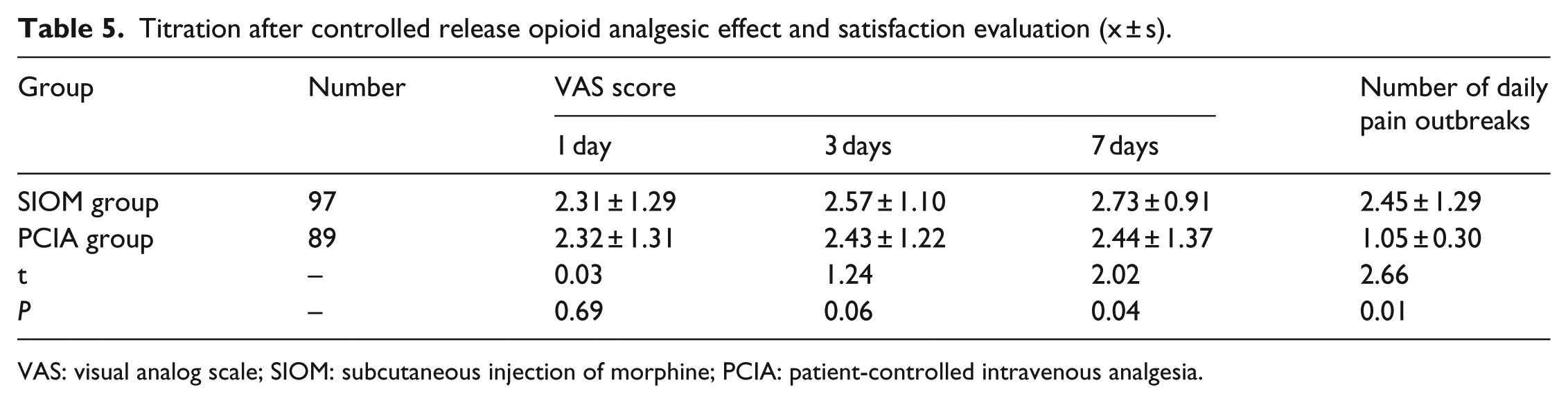
VAS: visual analog scale; SIOM: subcutaneous injection of morphine; PCIA: patient-controlled intravenous analgesia.
Discussion
Although there have been many advances in the treatment of cancer pain, opioids are still the key drugs for the treatment of cancer pain. Based on this unique feature of opioid drugs, first dose titration is emphasized in the initial clinical opioid or opiate dose adjustments to ensure safe and effective individualized drug use. 4 Due to the slow onset of oral morphine, patients need to adjust the dose several times to obtain accurate opioid demand. It usually takes 2–3 days to complete one titration, or even longer. Patients have to suffer pain during titration, which severely reduces the satisfaction. 5
To understand the feasibility of PCIA technology for opiate titration in patients with severe cancer, we used PCIA technology for opiate titration in patients with severe cancer. The shorter time needed in this study may be due to the need for multiple assessments and administrations during oral, subcutaneous, or intravenous titration, and in particular the substantial increase in the workload of the health care workers by injection. The titration time in the PCIA group was only about one-fourth of that in the subcutaneous injection group, which may be due to the fact that PCIA is administered intravenously and can be treated at small doses over short periods of time. The analgesic effect of the PCIA group was better than that of the subcutaneous injection group when the slow-release opiate was used instead.
Due to the limitation of the mode of administration, this study cannot be double-blind, which may affect the objectivity of observation. In addition, due to the limited sample size, the study failed to stratify age, nor did it perform a categorical and controlled analysis of the types and genders of cancer pain, which are all further research directions. To sum up, PCIA technology can rapidly, effectively, and safely complete opioid dose titration for cancer pain treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.