
Abstract
Septic shock (SS) leads to a high mortality rate for sepsis patients. Norepinephrine (NE) is a preferred vasoactive agent in SS treatment. This study aimed to assess the effects of NE at different administration time and NE combined with SP treatment on the cardiac function and prognosis of SS.
SS patients received NE treatment at different administration time and NE combined with SP treatment were enrolled in this study. The serum levels of cardiac troponin I (cTnI) and B-type natriuretic peptide (BNP), ejection fraction (EF), and pressure-adjusted heart rate (PAR) value were analyzed to evaluate cardiac function. The 28-day survival information was collected and assessed using the Kaplan-Meier method and log-rank test.
The cardiac function of SS patients was improved significantly by NE treatment, especially in the patients received NE at 2 h after fluid infusion, which evidenced by the increased BNP and cTnI levels and EF% and the decreased RAP. In the NE-2 h group, SS patients had a better 28-day survival rate compared with those patients in NE-1 h and -3 h groups. Furthermore, the significantly improved cardiac function and survival outcomes were found in patients received NE combined SP treatment.
Taken together, this study results show that NE administration at 2 h after fluid infusion may be the optimal time point for the treatment of SS and NE combined with SP treatment can improve early cardiac dysfunction and 28-day survival outcomes in patients with SS.
Introduction
Sepsis is a life-threatening disease caused by the abnormal host response to infection. 1 Septic shock (SS) is defined as a subset of sepsis with profound cellular, circulatory, and metabolic abnormalities. 2 Patients with SS have a significantly high mortality rate compared with patients with sepsis alone. 3 The pathophysiological abnormalities of SS are characterized by infiltration into multiple organs, neutrophil activation, and cardiovascular dysfunction. 4 The invasion of pathogens leads to a stress reaction in tissues and organs, and the defensive capacity of the body can be enhanced by moderate stress responses, but prolonged exposure to pathogens will aggravate impairments in tissues and organs. 5 During the development of SS, impaired tissues and organs stimulate inflammatory responses by promoting the release of pro-inflammatory cytokines, such as IL-6 and TNF-α. 6 For the current treatment of SS, patients immediately receive intravenous injection, vasopressors, liquid injection to improve the balance of circulation. 7
It is reported that multiple organ failure is the leading cause of high SS mortality. 8 Most SS cases are accompanied by organ dysfunction, among which the damage to the organs in the cardiovascular system leads to cardiac dysfunction. 9 It is known that early effective fluid resuscitation can increase cardiac output, improve oxygen delivery, and improve tissue and organ perfusion in SS patients, but fluid overload may aggravate tissue edema and hypoxia. 10 Therefore, the rational application of vasoactive drugs has become a hot topic in current research. Thus, the rational application of vasoactive drugs and myocardial energy supplements are necessary to protect against cardiac dysfunction in the treatment of SS. In the International Guidelines for Management of Sepsis and SS in 2016, norepinephrine (NE) is recommended as the preferred vasoactive agent. 11 The clinical use and research about NE are mainly focused on the drug dosage, but the optimal administration time for NE remains indetermination. 12 Sodium phosphocreatine (SP) is defined as a new energy supplement, which can provide exogenous myocardial energy. 13 However, the understanding of the therapeutic application of SP in SS is limited.
This study retrospectively analyzed the cardiac function of SS patients after the treatment of NE or NE combined SP treatment. In addition, the survival outcomes of the patients were also evaluated in different groups. The results of this study may provide evidence to improve the clinical application of NE and SP in SS patients and uncover the effects of NE and SP on the prognosis of SS.
Materials and methods
Patient selection and sample collection
The data collected from 162 SS patients, who received treatment in the emergency department and critical care unit of Affiliated Hospital of Chengde Medical University between 2016 and 2019, were retrospectively analyzed in this study. The patients were recruited based on the following inclusion criteria: (1) diagnosis was performed based on the SS diagnosis criteria in the Sepsis 3.0 by the Society of Critical Care Medicine (SCCM) and European society intensive care medicine (ESICM) 14 ; (2) age of more than 18 years old; (3) had no diseases in heart, liver, kidney or other organs; (4) had no history of tumors; (5) no pregnant or lactating patients. All the patients received fluid resuscitation and anti-infection treatments, and were classified into four groups based on the different administrations of NE and SP, including NE-1 h group (NE administration at 1 h after fluid infusion, n = 32), NE-2 h group (NE administration at 2 h after fluid infusion, n = 48), NE-3 h group (NE administration at 3 h after fluid infusion, n = 40) and NE + SP group (NE combined SP administration, n = 42). NS (5–15 mg/min) was used by central venous pumping to maintain the mean arterial pressure (MAP) ⩾65 mmHg, and SP (2 g/day) was used by intravenous drip. The NE administration was performed at 2 h after fluid infusion in the NE + SP group.
Ethical approval
The experimental protocols of this study were approved by the Ethics Committee of Affiliated Hospital of Chengde Medical University (NO. 2016002). The informed consent was obtained from each patient for clinical data analysis. The personal information of the patients was anonymous.
Data collection
The serum levels of cardiac troponin I (cTnI) and B-type natriuretic peptide (BNP) were measured by Chemiluminescence immunoassay in the next morning after treatment. The ejection fraction (EF) was also evaluated using echocardiography at the same time. Marshall cardiac function score was obtained by calculating the pressure-adjusted heart rate (PAR) value. 15 Additionally, the levels of systolic arterial blood pressure (SBP), diastolic arterial pressure (DAP), and mean arterial pressure (MAP) were also recorded. The 28-day survival information of the participants was recorded for the subsequent survival analysis.
Statistical analysis
All the data obtained from this study were expressed as mean ± SD and analyzed using SPSS statistical software (SPSS Inc., Chicago, IL) and GraphPad Prism software (GraphPad Software, Inc, USA). Differences between groups were used Student’s t-test, Chi-square test or one-way ANOVA followed by Tukey’s test as appropriate. Kaplan-Meier survival curves were performed to evaluate the 28-day survival outcomes, and log-rank test was used to analyze the distribution of survival curves. A P value of less than 0.05 was considered statistically significant.
Results
Baseline characteristics of SS patients
The baseline characteristics of SS patients, including age, gender, acute physiology, and chronic health evaluation (APACHE) II score and sequential organ failure assessment (SOFA), were summarized in Table 1. By the comparison between groups, there were no differences in age, gender, APACHE II score and SOFA score between NE-1 h, NE-2 h, NE-3 h and NE + SP groups (all P > 0.05).
Baseline characteristics of SS patients in different groups.

SS: sepsis shock; NE: norepinephrine; SP: sodium phosphocreatine; APACHE: acute physiology and chronic health evaluation; SOFA: sequential organ failure assessment.
Cardiac function in SS patients with different times of NE administration
The cardiac function was evaluated in SS patients by analyzing BNP, cTnI, EF, PAR, SBP, DAP and MAP. As shown in Table 2, the cardiac function in each group had no difference before receiving treatment (all P > 0.05), and was significantly improved after basic treatment including NE administration (all P < 0.05). More importantly, we found that the therapeutic efficacy in cardiac function was markedly better in patients received NE treatment at 2 h after fluid infusion than that in the patients received NE administration at 1 h and 3 h, as evidenced by the significantly decreased levels of BNP, cTnI, EF% and PAR (all P < 0.05). Although the cardiac function-related data were also reduced in NE-3 h group compared with NE-1 h group, there was no statistical significance in the difference in addition to the results of BNP. Additionally, there was no significant difference for the levels of SBP, DAP and MAP among the three groups before or after NE administration.
Cardiac function changes in SS patients received CE administration at different time points.

SS: sepsis shock; NE: norepinephrine; SP: sodium phosphocreatine; BNP: B-type natriuretic peptide; cTnI: cardiac troponin I; EF: ejection fraction; PAR: pressure-adjusted heart rate; SBP: systemic blood pressure; DAP: diastolic arterial pressure; MAP; mean arterial pressure.
Compared to pretreatment data in each group, *P < 0.05; compared to NE-1 h group, #P < 0.05; compared to NE-2 h group, &P < 0.05.
Effect of NE combined with SP on cardiac function in SS patients
To further uncover the therapeutic efficacy of SP in SS patients, the cardiac function in patients received NE combined SP was examined. The data listed in Table 3 showed that no difference was presented in the cardiac function between NE group and NE + SP group before treatment (all P > 0.05). By comparing the cardiac function key indicators, the results revealed that SS patients received NE combined with SP treatment had lower levels of BNP, cTnI, and PAR compared with those without SP administration, and a higher level of EF% (all P < 0.05), indicating that the cardiac function was significantly improved by the treatment of NE combined with SP. But the levels of BP, DAP, and MAP showed no significant difference between the two groups (all P > 0.05).
Effect of NE combined with SP on cardiac function in SS patients.
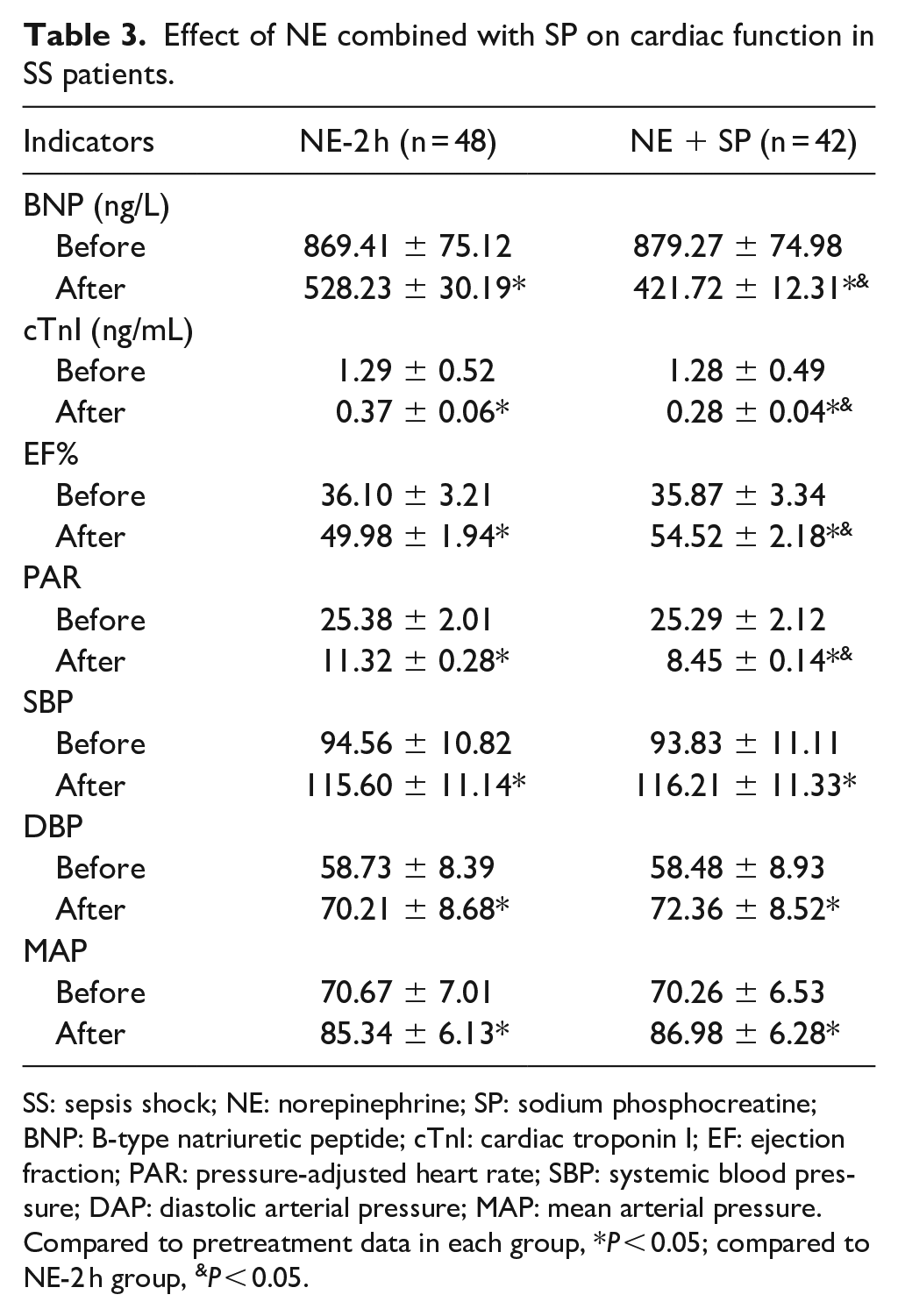
SS: sepsis shock; NE: norepinephrine; SP: sodium phosphocreatine; BNP: B-type natriuretic peptide; cTnI: cardiac troponin I; EF: ejection fraction; PAR: pressure-adjusted heart rate; SBP: systemic blood pressure; DAP: diastolic arterial pressure; MAP: mean arterial pressure.
Compared to pretreatment data in each group, *P < 0.05; compared to NE-2 h group, &P < 0.05.
Survival outcomes in SS patients with different times of NE administration
This study collected the 28-day survival information of the study population and found that there were 20 deaths (62.5%) in NE-1 h group, 19 deaths (39.6%) in NE-2 h group, 24 deaths (60.0%) in NE-3 h group and 8 deaths (19.0%) in NE + SP group. Kaplan-Meier curves were subsequently constructed to evaluate the effect of NE treatment on SS prognosis. As shown in Figure 1, SS patients received NE at 2 h after fluid infusion had the longest survival time than the patients in NE-1 h (log-rank P = 0.002) and NE-3 h (log-rank P = 0.040) groups. Although the survival rate in NE-3 h group was better than the NE-1 h group, the difference was not statistically significant (log-rank P = 0.158).

The 28-day survival curves for SS patients in different NE treatment groups. The curves were plotted by Kaplan-Meier method and compared by log-rank test.
NE combined with SP improves the prognosis of SS patients
The 28-day survival in SS patients between NE and NE combined SP groups also were analyzed. The survival curves shown in Figure 2 revealed that SS patients had longer survival time in NE + SP group compared with the NE-2 h group (log-rank P = 0.029), indicating that SP could significantly improve the prognosis of SS patients.

The 28-day survival curves for SS patients received NE and SP treatments. The curves were plotted by Kaplan-Meier method and compared by log-rank test.
Discussion
The essence of SS is the response of the body to infectious factors, and the vascular smooth muscle contraction disturbance, arteriovenous dilatation, and cardiac dysfunction induced by vascular paralysis are the leading causes of SS. 4 It is known that early effective fluid resuscitation can increase cardiac output, improve oxygen delivery, and improve tissue and organ perfusion in septic shock patients, but fluid overload may aggravate tissue edema and hypoxia, so the rational application of vasoactive drugs has become a hot topic in current research. NE is a well known vasoactive agent, based on full fluid resuscitation, NE constricts the volume of blood vessels and increases the volume of blood circulating in the center to correct the abnormal distribution of blood flow caused by the abnormal expansion of pathological blood vessels. It will reduce the incidence of low perfusion, systemic vascular resistance, even fatality rate. In this study, early resuscitation treatment was carried out strictly according to the international guidelines for the management of sepsis and SS edited in 2016, then based on full fluid resuscitation, NE was used to maintain the patient’s MAP at more than 65 mmHg to ensure the perfusion of important organs. 11
The results of this study showed that the SS patients had significantly low EF% and high PAR value, indicating that there were obvious cardiac dysfunction and hemodynamic disorders in the SS patients. After NE treatment, EF% was significantly increased, and PAR was significantly decreased, which was consistent with the previously reported results that also demonstrated the beneficial effect of NE on cardiac function of SS patients.16–18 BNP and cTnI are commonly used cardiac biomarkers. 19 In recent years, it has been found that BNP and cTnI are closely related to myocardial systolic dysfunction. 20 In SS, in addition to the direct action of inflammatory cytokines, the immunopathological response of the complement system and the imbalance of the autonomic nervous system, the dysfunction of mitochondria and abnormal energy metabolism can also lead to myocardial apoptosis and myocardial remodeling. 21 In this study, the increased BNP and cTnI levels were decreased significantly in SS patients underwent NE treatment. For the therapeutic mechanisms of NE, it is reported that NE can activate α or β-adrenoceptor, contract peripheral blood vessels, increase peripheral vascular resistance, increase blood pressure and cardiac blood volume, which leads to the increase in left ventricular stroke volume. 22 Therefore, the levels of SBP, DAP and MAP were also recorded, it was found that after NE treatment, they were all increased significantly in the three groups, indicating that NE treatment raised and keep the blood pressure stable.
Although NE has been widely used in the treatment of SS, the optimal administration time to use NE remains unclear. It is essential to ensure the application time of vasoactive drugs, which is our objective of the present study. In this study, we found that the increase in EF% and the decrease in PAR were more significant in SS patients received NE at 2 h after fluid infusion compared with those patients with NE at 1 and 3 h after fluid infusion. As the results indicated, the therapeutic efficacy in cardiac function was remarkably better in patients received NE treatment at 2 h after fluid infusion than that in the patients received NE administration at 1 and 3 h after fluid infusion. It is also reported that the improvement of cardiac function in septic shock patients under NE is mainly due to the increase in DAP, therefore, we further analyzed whether the different administration times of NE influence DAP. But the results suggested that there was no significant difference for the arterial pressure among the three groups 24 h after NE treatment. The results suggested that different administration time to use NE may have no significant influence on the increase of blood pressure 24 h after treatment, but it would be interesting to explore the efficiency time of NE treatment, which might before 24 h following NE treatment.
Cardiac dysfunction is a consequence of SS, which is one of the important components of multiorgan failure caused by severe sepsis. 23 The mortality of septic patients with systolic or diastolic dysfunction is higher than those without myocardial depression. 24 It is known that NE treatment in SS can not only activate α-adrenoceptor but also promote β1 or β2-adrenoceptor activation, which contribute to the regulation of cardiac rate and contractility.25–27 Consistently, the present results indicated that after NE treatment, cardiac contractility of SS patients was improved, which was reflected by the increase of the EF% level. The occurrence of cardiac dysfunction can also reduce the abilities of SS patients to produce ATP through oxidative phosphorylation and the imbalance of Ca2+ homeostasis in cardiomyocytes. Thus, the cardiac automaticity is inhibited due to the weakening in excitation-contraction coupling and deactivation of the Na+ - K+ channels, which results in the impossible to effectively transfer chemical energy to systolic work. 28 As a kind of molecular carrier of energy substance ATP in high energy-consuming cells, such as myocardium, skeletal muscle and brain cells, SP can balance ATP consumption and ensure energy reserves. 29 Therefore, this study further analyzed the cardiac function and prognosis in SS patients who received NE combined SP treatment. The cardiac function results revealed that EF% was elevated and PAR was reduced in the combination group compared with the NE group. And the 28-day survival rate in the combination group was significantly higher than that in the NE group. It is suggested that NE combined with SP may improve the early hemodynamics and improve the 28-day survival rate in patients with SS.
It has been reported that SS patients with systolic or diastolic dysfunction had high mortality than those without myocardial depression. 24 The 28-day survival in SS patients between NE and NE combined SP groups also were analyzed in the present study. By evaluating the 28-day survival information, patients in NE-2 h group showed better survival than that in the NE-1 h and -3 h groups. These results suggested that the cardiac function and prognosis of SS patients might be significantly improved by NE administration at 2 h after fluid infusion. In the case of inadequate fluid resuscitation, further constriction of blood vessels leads to further reduction of blood supply to important organs, which may be an important reason for the reduced survival rate in the NE 1H group. Additionally, as WAECHTER et al. reported, based on fluid resuscitation, the mortality of patients treated with vasoactive drugs in the early was lower, while the mortality of patients treated with vasoactive drugs in the early 1 h was higher, 30 which was consistent with our present results.
However, there are several limitations for the present study. Firstly, the study population of the present study is relatively small, and the results of the study are needed to be verified in other studies with a larger population. And the basic experiment is needed to explore the underlying mechanism in depth. Additionally, in the current study, limited biomarkers were included to reflect the cardiac function, which may also be influenced by other conditions, such as acute kidney failure, therefore, more indicators should be included in future studies.
Conclusion
To sum up, NE administration at 2 h after fluid infusion may be the optimal time point for the treatment of SS and NE can cooperate with SP to improve early cardiac dysfunction and 28-day survival outcomes in patients with SS. The results of the study may provide evidence to improve the clinical application of NE and SP. However, this study is a small group experiment, and the results require to be verified by large-scale clinical epidemiological investigations. And basic experiments are necessary to analyze the underlying mechanism more deeply.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
The experimental protocols of this study were approved by the Ethics Committee of Affiliated Hospital of Chengde Medical University. The informed consent was obtained from each patient for clinical data analysis. The personal information of the patients was anonymous.