
Abstract
Radiofrequency ablation (RFA) for hepatocellular carcinoma (HCC) located in the caudate lobe is technically challenging because of the tumor’s deep location and proximity to major vascular structures. A 71-year-old woman with a 2-cm HCC in segment I underwent conventional transcatheter arterial chemoembolization (TACE) via the femoral artery. Immediate RFA was not feasible because CT arterial portography revealed no safe puncture route due to surrounding vasculature. On the following day, angiography using a left transradial approach was performed with the patient in the prone position, enabling identification of a safe dorsal puncture path. After creation of an artificial pneumothorax, percutaneous CT-guided RFA was successfully completed without complications. Prone transradial angiography can facilitate safe RFA for hepatic tumors in anatomically challenging locations such as the caudate lobe. This approach may broaden treatment options when conventional supine access is not possible.
Keywords
Introduction
Hepatocellular carcinoma (HCC) located in the caudate lobe is technically challenging and often considered unsafe to treat with radiofrequency ablation (RFA) because of its deep location and proximity to major vascular structures.1,2 Previous studies have reported that HCCs in the caudate lobe have up to five times higher local recurrence rates compared with tumors in other hepatic segments. 1 This can be attributed to the heat-sink effect caused by large vessels such as the inferior vena cava and to the difficulty in obtaining an optimal puncture route because the tumor is surrounded by vessels.
Combined RFA and transcatheter arterial chemoembolization (TACE) is an established strategy for HCC.1,2 This approach mitigates the heat-sink effect, but when the tumor is encased by portal veins, establishing an appropriate puncture path remains problematic, which may lead to incomplete ablation.
In the present case, we initially attempted RFA combined with TACE in the supine position for a caudate lobe HCC, but a safe puncture route could not be obtained. We therefore performed angiography in the prone position using a left transradial approach, which has previously been reported in procedures involving extrahepatic organs.3–5 By combining this approach with the creation of an artificial pneumothorax, safe and complete ablation was achieved. The details of this technique are described below.
Case description/technique
A 71-year-old woman with a history of steatohepatitis and compensated liver cirrhosis (Child–Pugh class A) was diagnosed with a 2-cm HCC in segment I (caudate lobe) of the liver. The lesion was identified on contrast-enhanced computed tomography (CT), showing arterial-phase hyperenhancement and delayed washout, consistent with HCC.
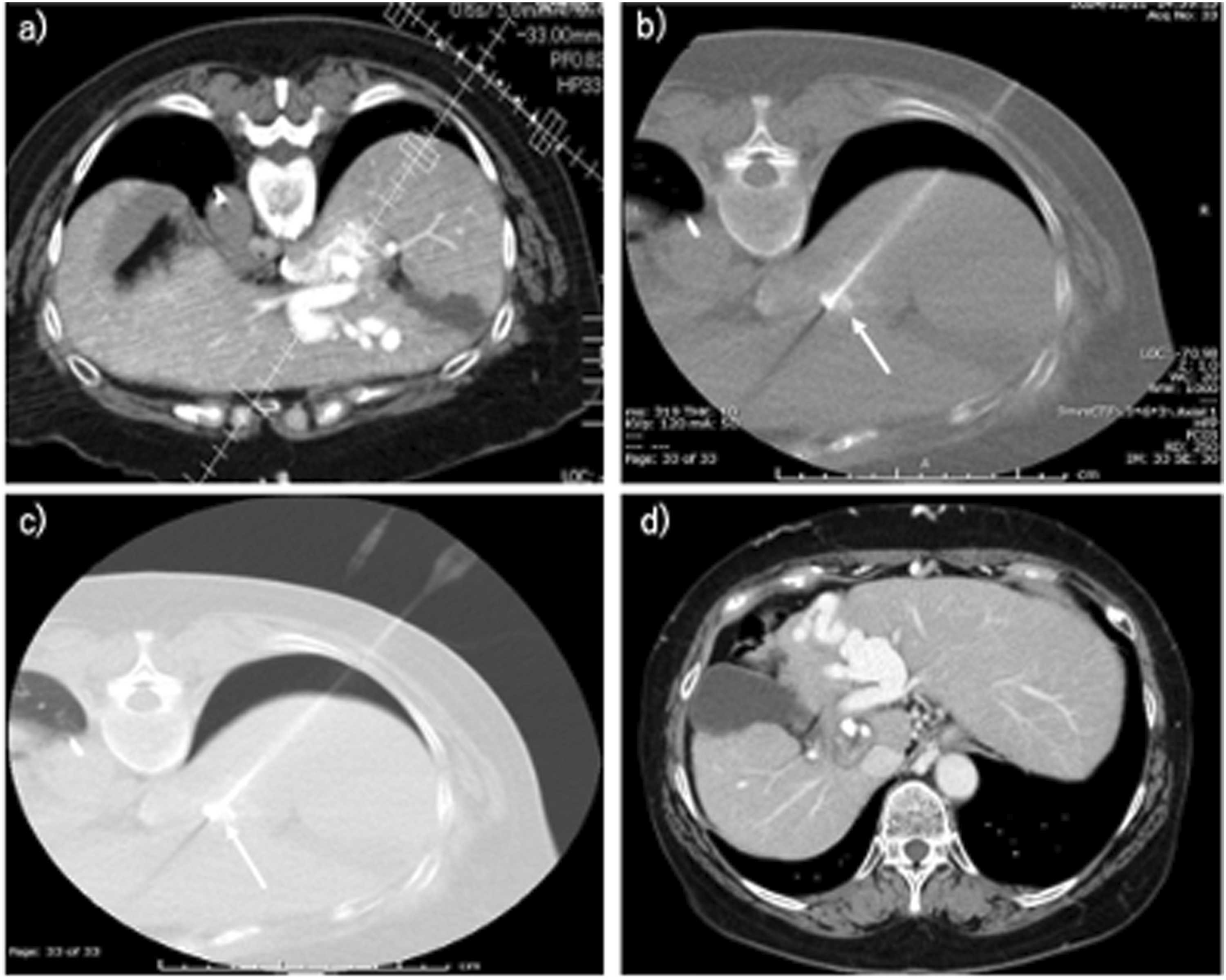
The tumor was not visualized on ultrasonography due to its deep location. A combined procedure of CT-guided percutaneous RFA immediately following conventional TACE was planned, using the femoral arterial approach with the patient in the supine position. However, CT arterial portography (CTAP) revealed no safe percutaneous route owing to the surrounding vascular structures (Fig. 1(a)). Computed tomography (CT) images of the patient (a and b). CT during arterial portography (a) and CT hepatic arteriography (b) performed with the patient in the supine position (arrow: target tumor). The portal vein runs over the ventral and lateral aspects of the tumor (a). (c) CT performed immediately after transcatheter arterial chemoembolization (arrow: lipiodol accumulation for target tumor).
It was considered that prone positioning might provide a feasible puncture path. Because a transradial device was not prepared at that time, only conventional TACE was performed on that day via the femoral artery using a mixture of lipiodol and epirubicin (total 2.3 mg).
On the following day, the superior mesenteric artery (SMA) was selectively catheterized for CTAP in the prone position using the left transradial approach with a 5-Fr Glidesheath Slender (Terumo, Japan) (Fig. 2(a)). CTAP confirmed a safe posterior puncture route avoiding major vessels (Fig. 3(a)). Artificial pneumothorax was created using the following method. Under CT guidance, an 18-G needle with a blunted tip was advanced to the pleural surface. After confirming its position, small amounts of air were gradually introduced while slightly advancing the needle, and pneumothorax formation was verified on CT. Subsequently, a VIVA radiofrequency electrode (STARmed, Goyang, South Korea) was inserted percutaneously from the dorsal side under CT guidance using angio-CT system (Canon, Tochigi, Japan), targeting the lipiodol-stained tumor (Figs. 2(b), 3(b) and 3(c)). RFA was performed using a 2.5-cm active tip. (a) Angiography performed via the left radial artery in the prone position using a 5-Fr Glidesheath Slender (Terumo, Japan). (b) Insertion of a VIVA RF needle (STARmed, South Korea) from the dorsal side after creation of an artificial pneumothorax. Puncture performed under computed tomography (CT) guidance. (a) Planning of puncture route for ablation based on CT during arterial portography with the patient in the prone position (arrow: target lipiodol). (b) Puncture performed under CT guidance using artificial pneumothorax with the patient in the prone position (arrow: target lipiodol). (c) Same image as shown in Fig. 3(b), in the lung window. (d) CT obtained at 9 months after the procedure.
After ablation, the celiac artery and common hepatic artery (CHA) were selectively catheterized to confirm the absence of arterial bleeding or arterioportal shunting on digital subtraction angiography. Air in the thoracic cavity was aspirated as much as possible. All procedures were performed by an interventional radiologist (R.S) with 10 years of experience in interventional oncology.
The procedure was completed without complications, as confirmed by post-procedural CT on the following day. The patient was discharged uneventfully. Follow-up imaging at 9 months demonstrated complete tumor necrosis with no evidence of local recurrence (Fig. 3(d)).
Discussion
RFA for HCC located in the caudate lobe is technically challenging because the tumor is deeply situated and surrounded by major vessels. In this case, the portal vein coursed over the tumor from its ventral to lateral aspect. Tilting the patient’s body alone did not allow for a puncture path that avoided the portal vein; therefore, the prone position was selected.
In the prone position, catheter manipulation through the femoral artery would have been difficult, and repositioning from supine to prone would have compromised the sterile field. Consequently, a transradial arterial approach was employed. Prone transradial access has previously been reported for intraoperative angiography during neurosurgical procedures6,7 and for combined embolization and ablation therapy for retroperitoneal tumors, such as those of the pelvis or kidney,3–5 but, to our knowledge, has not been reported for hepatic tumors.
This technique may be particularly useful when a dorsal puncture is required for RFA combined with TACE, as in lesions of the caudate lobe or posterior hepatic segments. However, because the puncture path usually traverses the lung, creation of an artificial pneumothorax is often necessary to ensure a safe approach.
Recent studies have also described RFA guided by CT hepatic arteriography (CTHA). 8 The present approach may be applicable in cases where conventional supine positioning does not provide a feasible puncture route, thereby offering an alternative for technically challenging ablations.
This report has several limitations that should be noted. It describes a single case with a follow-up period of only 9 months, and therefore, adequate ablation margins and long-term local control remain uncertain. Furthermore, because TACE and RFA were not performed in the same session, the feasibility of performing effective TACE in the prone position is still unknown. In this case, the SMA and CHA were successfully catheterized in the prone position, similar to standard supine procedures. Therefore, catheter manipulation itself appears feasible. However, whether TACE can achieve drug delivery equivalent to that in the supine position remains uncertain and requires further accumulation of cases.
Nevertheless, this case illustrates that modifying the patient’s position and access route can expand treatment options by enabling safe puncture even when standard approaches are not possible.
In conclusion, this case demonstrates that the prone position using radial arterial approach can be an effective alternative for performing RFA combined with TACE in patients with difficult-to-access posterior hepatic tumors. With careful patient selection and procedural planning, this approach may expand the technical possibilities of interventional oncology for liver tumors.
Footnotes
Author contributions
All authors contributed to the conception and design of the study. The first draft of the manuscript was written by RS, and all authors commented on previous versions of the manuscript. All the authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Our study was approved by the respective Institutional Review Board in our hospital (J2025-4-2025-1-3).
Consent for publication
Consent for publication was obtained from the patient.
Data Availability Statement
All data in this article are available from the corresponding author.