
Abstract
Lymphoplasmacytic lymphoma (LPL)/Waldenström macroglobulinemia (WM) is an uncommon mature B cell lymphoma usually involving the bone marrow and, less commonly, the spleen and/or lymph nodes. This case presents a pathology-confirmed isolated extramedullary relapse of LPL, located in subcutaneous adipose tissue, 5 years after successful treatment of WM.
Introduction
Lymphoplasmacytic lymphoma (LPL)/Waldenström macroglobulinemia (WM) is an indolent B-cell non-Hodgkin lymphoma (NHL) representing 1–2% of all NHLs, characterized by tissue infiltration of B-lymphocytes, lymphoplasmacytoid cells, and plasma cells, usually involving bone marrow (BM) and, less commonly, the spleen and/or lymph nodes.1–3 LPL is virtually always associated with a monoclonal immunoglobulin M (IgM), corresponding to WM, cases of LPL presenting without a serum monoclonal IgM are extremely rare. 4 The incidence of LPL/WM is approximately three per million people per year. 5 Presentation of extramedullary disease (EMD)/visceral disease based on pathological identification or positive Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) findings was identified in 4% and 11% of WM, respectively.6,7 21% of patients present with EMD involvement at initial WM diagnosis, and 79% develop EMD at WM relapse. Most frequent EMD sites involved were pulmonary (30%) and central nervous system (23%). 6 There have been only a handful of reports of soft tissue 18F-FDG PET LPL/WM infiltration in the central nervous system,8–10 lung and pleura, skin, liver, and bowel. 7 There has been a single report of WM infiltration as a subcutaneous mass by Palmer et al. 11 However, to the best of our knowledge, we report the first case of the isolated LPL presentation in subcutaneous adipose tissue, as detected on 18F-FDG PET/CT.
History
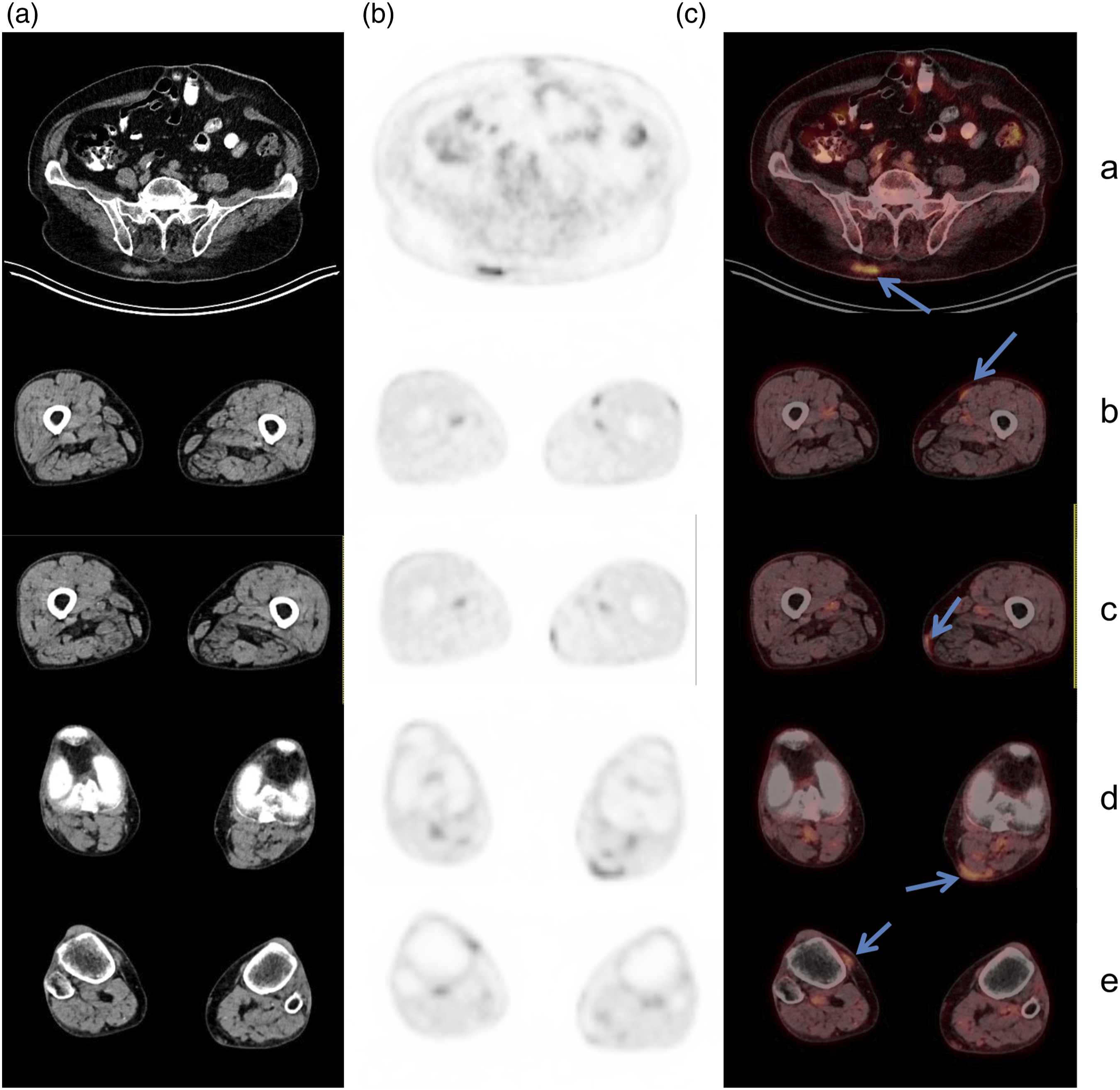
A 76-year-old lady was diagnosed with WM 5 years ago, presenting with anemia, a high serum monoclonal IgM of 49 g/L, and involvement of the BM, mediastinal and abdominal lymph nodes, and the spleen. She received initial treatment of four cycles of bortezomib, dexamethasone, and rituximab and subsequently 2 cycles of cyclophosphamide, dexamethasone, and rituximab due to neuropathy. Five years in complete remission, she presented with a thickening in the left popliteal fossa. Biopsy of the popliteal mass suggested LPL. Serum monoclonal gammopathy was not present, blood counts were normal and symptoms of the disease were absent. No enlarged lymph nodes or splenomegaly were observed. 18F-FDG PET/CT was performed. Several lesions with mild hypermetabolic activity were seen (arrows) on coronal and sagittal MIP of whole-body PET scan (Figure 1): irregular lobular soft tissue density measuring 32 × 11 mm in the right gluteal subcutaneous fat with an SUVmax 5.4 (Figure 2(a)), and several small fusiform nodules in the subcutaneous fat tissue of the left mid-thigh with an SUVmax 2.4 (Figure 2(b)), the left lower thigh with an SUVmax 2.9 (Figure 2(c)), the left popliteal fossa with an SUVmax 3.5 (Figure 2(d)), and of the right knee with an SUVmax 3.2 (Figure 2(e)). A physiologic uptake of FDG was seen elsewhere in the body, including BM, lymph nodes, and the spleen. A subsequent ultrasound-guided biopsy of the right gluteal subcutaneous formation confirmed LPL with IgM deposits in the tumor tissue. Due to lack of constitutional symptoms, normal blood counts and indolent nature of the disease it was decided to watch-and-wait until progression and not to proceed with systemic treatment. Within the following 2 years the disease did not progress and the IgM remained negative. Coronal and sagittal image of whole-body 18F-FDG PET/CT scan. Arrows mark multiple subcutaneous tissue hypermetabolic LPL lesions. Axial CT (a), PET (b), and fusion (c) whole body 18F-FDG PET/CT images of subcutaneous tissue hypermetabolic LPL lesions (arrows) in the right gluteal subcutaneous fat (a), the left mid-thigh (b), the left lower thigh (c), the left popliteal fossa (d), and the right knee (e).
Discussion
A presented case reports an unusual extramedullar presentation of LPL relapse in the subcutaneous tissue and negative serum IgM in a patient previously successfully treated for medullar and visceral WM. The utility of 18F-FDG PET/CT in assessment of EMD LPL/WM is demonstrated.
In conclusion,18F-FDG PET/CT could play a role in a diagnostic procedure of smoldering WM. Moreover, a whole-body head-to-toe PET-CT acquisition might be needed not to miss unexpected locations of the disease, while morphologic features seen on CT may not be indicative of a malignant nature of LPL/WM findings.
Footnotes
Authors’ note
Both authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All data presented are available upon request.
Ethical approval
The study was conducted in accordance with the Helsinki declaration.
Consent for publication
The patients signed an informed consent statement.