
Abstract
The aim of this study was to evaluate the relationship of prognosis of patients with multiple myeloma having extramedullary involvement (EMM) with the 18F- fluorodeoxyglucose(18F-FDG) maximum standardized uptake value and the expression of Ki-67 in biopsy samples. Sixty-five patients were newly diagnosed with multiple myeloma presenting with EMM at our hospital from January 2005 to January 2015. Of these 65 patients, 20 were enrolled in this study. Over the last decade, both the maximum standardized uptake value and Ki-67 expression in these extramedullary lesions significantly correlated with progression-free survival, respectively (P= .039, P =.009). After combining—the maximum standardized uptake value and the Ki-67 expression as an integral—there was a significant correlation between both the overall survival (P = .027) and progression-free survival (P= .014). Patients have poor outcomes when EMM is detected at presentation. Both the maximum standardized uptake value and Ki-67 expression could aid in accurately evaluating EMM patient prognosis.
Multiple myeloma (MM) is a B-cell disorder characterized by the clonal proliferation of malignant B cells in the late stages of lymphoid differentiation. 1 The overall survival (OS) of patients with MM has significantly increased due to the availability of drugs such as bortezomib and lenalidomide as well as the frequent transplantation of autologous stem cells. Although the bone marrow is usually involved, MM can spread to extramedullary involvement (EMM) and inhabit any tissue, including the liver, lymph nodes, spleen, kidneys, breast, and pleura. 2 Blade et al 3 proposed 2 distinct mechanisms that lead to EMM: direct spread of bone plasmacytomas upon cortical destruction and hematogenous dissemination of MM cells as an “escape phenomenon.” Importantly, the presence of EMM is associated with a poor prognosis based on high-risk features on gene expression profiling and shorter progression-free survival (PFS) and OS. 4
Positron emission tomography/computed tomography (PET/CT) examines both morphology and function and is a tool useful in staging patients with multiple tumors, including for those with MM. 5 -7 Positron emission tomography/CT has been demonstrated to have a sensitivity of 96% and a specificity of 77.8% for detecting EMM. 8 Furthermore, PET/CT is an excellent imaging tool for monitoring the response to treatment and assessing prognosis. 9,10 Interestingly, PET/CT has been reported to be more sensitive at detecting EMM than other plasma cell tumors; however, the mechanisms behind this and the implications of the reports that PET/CT could increase sensitivity are unclear.
Ki-67 is a cell proliferation marker that is exclusively expressed during active phases of cell cycle. The percentage of Ki-67 positive tumor cells has been confirmed to be indirectly correlated with prognosis of patients with a number of cancers in terms of PFS and OS. 11 Multiple myeloma is a type of cancer that typically proliferates at a very low rate. In retrospective MM studies, Ki-67 staining has been reported in less than 10% of cancer cells. Extramedullary involvement is an indication to evaluate Ki-67 at presentation. Proliferation as measured by Ki-67 expression by immunohistochemistry is associated with advanced pathological stages of MM and is also an important prognostic factor when evaluating MM. 12,13 Therefore, this study assessed the association between PET-CT and Ki-67 and their significance in evaluating the prognosis of patients with EMM.
Materials and Methods
Patients
Sixty-five patients presented with EMM at the Tianjin Medical University Cancer Institute and Hospital between January 2005 and January 2015. Twenty of these patients were enrolled in this study. Written informed consent for publication of their clinical details was obtained from the patient/parent/guardian/relative of the patient. All 20 enrolled patients met the International Myeloma Working Group (IMWG) criteria 14 and underwent a PET/CT scan and immunohistochemical staining of a biopsy for Ki-67. The clinical and laboratory data were reviewed in retrospect, and data collected included patient gender, age, pathologic subtype of EMM, clinical stage of EMM, treatment, time to relapse or death, date of last follow-up, serum lactate dehydrogenase (LDH) levels, plasma cell population size, and Ki-67 expression levels in extramedullary lesions.
Positron Emission Tomography/Computed Tomography
The PET/CT was purchased from the GE Company (Fairfield, Connecticut). Prior to performing the PET/CT, patients fasted for at least 4 to 6 hours so that blood glucose levels were less than 6.8 mmol/L. After the patient rested 15 minutes, 18F-FDG was intravenously injected into the arm. Forty to 60 minutes after the injection, a full body scan was initiated and performed and then the data were collected. All resulting images were carefully and independently analyzed by 2 nuclear medicine physicians. An area was designated a region of interest (ROI) when it was 5 to 10 mm large within the malignant lesions by adjustment. The standardized uptake value (SUV) of the ROIs was calculated using SUV = [mean activity (ROI) (MBq/mL)/injected dose (MBq)]/total body weight (g). In this study, the targeted lesions were defined as maximum SUV (SUVmax) > 2.5 in the baseline PET/CT images with a maximum diameter > 1 cm in CT images. 15,16
Tumor Samples
Biopsies were taken of extramedullary lesions by cutting or puncturing the mass. All specimens to be examined by histological staining were fixed in formalin and embedded in paraffin. Paraffin sections were immunostained with antibodies against Ki-67 using a labeled streptavidin–avidin biotin method. Ki-67 immunohistochemistry was performed in tumor-rich areas. Healthy tonsil tissue was used as a positive control when evaluating Ki-67 reactivity. The Ki-67 score is expressed as the percentage of cells that were positive for nuclear-staining compared to the total number of invasive cells in 3 high-power fields viewed using the 40× objective. The samples were then divided into those that had high levels of Ki-67 expression (≥35%) and low levels (<35%).
Treatment and Assessment of Response
Chemotherapy regimens included VADT (vincristine, doxorubicin or liposomal doxorubicin and dexamethasone, thalidomide) and BD (bortezomib and dexamethasone). If patients presented with oppression symptoms, local radiotherapy was performed. The response of the patient to treatment was assessed using the IMWG uniform response criteria, 14 which was scaled as the patient having a complete response (CR), near CR (nCR), very good partial response, partial response (PR), minimal response (MR), progressive disease (PD), and stable disease.
Statistical Analyses
Overall survival was defined as the length of time between a diagnosis of MM and death or, in censored patients, last follow-up. Progression-free survival was measured as the length of time between the start of treatment and the progression of disease or mortality. All data analyses were performed using SPSS software version 21.0 (SPSS Inc, Chicago, Illinois) and Graph Pad Prism 5. P values are presented as 2-sided, where statistical significance was considered a P < .05.
Results
Clinical Features
In the 644 patients who presented with plasma cell tumors at the Tianjin Medical University Cancer Institute and Hospital between January 2005 and January 2015, approximately 10.1% (65/644) had EMM. The major clinical characteristics of the 20 patients enrolled in this study are shown in Table 1. The most common locations of extramedullary lesions were the parosteal soft tissues (beside spine [8/20, 40%] and beside ribs [4/20, 20%]), lesions were also found in neck (2/20, 10%), walls of the chest (2/20, 10%), liver (1/20, 5%), gums (1/20, 5%), lungs (1/20, 5%), and kidneys (1/20, 5%; see Supplementary Material Table 1, Supplementary Material Figure 1). All of the enrolled patients had 1 site of extranodal involvement. Most of the patients presented with unexplained neoplasm. Fifteen patients (15/20, 75%) presented with stage III according to the Durie-Salmon (DS) scale, while 10 (10/20, 50%) were stage III based on the International Staging System (ISS). Clinical features were primarily manifestations of the extramedullary lesion or MM. In terms of hematological and chemical manifestations, no special modifications were found. Positron emission tomography/CT scans of these 20 patients revealed extramedullary lesions.
Clinical Characteristics of 20 Patients With EMM.

Abbreviations: DS, Durie-Salmon; ISS, International Staging System; LDH, lactate dehydrogenase.
Treatment Parameters and Outcomes
In this study, 16 patients were treated solely with chemotherapy (10 patients received VADT × 6 cycles and 6 patients received BD × 6 cycles), and 1 patient received BD × 4 cycles and underwent autologous transplantation. Radiotherapy (40-50 Gy) was performed on 3 patients (2 patients received VADT × 6 cycles and 1 patients received BD × 6 cycles) in order to reduce their symptoms. Overall survival and PFS statistics are only for 16 patients who were treated solely with chemotherapy.
The follow-up time, starting from the date of diagnosis until July 31, 2016, or death, ranged from 3 to 90 months with a median of 32 months. At 3 and 5 years post-diagnosis, the OS was 85.9% and 82.9% and the PFS was 80% and 59.6%, respectively (Figure 1). The response to therapy was assessed, while 4 (4/20, 20%) patients achieved a CR/nCR, 4 (4/20, 20%) patients had a PR, 5 patients had an MR, 5 patients had a PD, and 2 patients relapsed. Both of the patients who relapsed were stage III based on both DS and ISS at diagnosis.
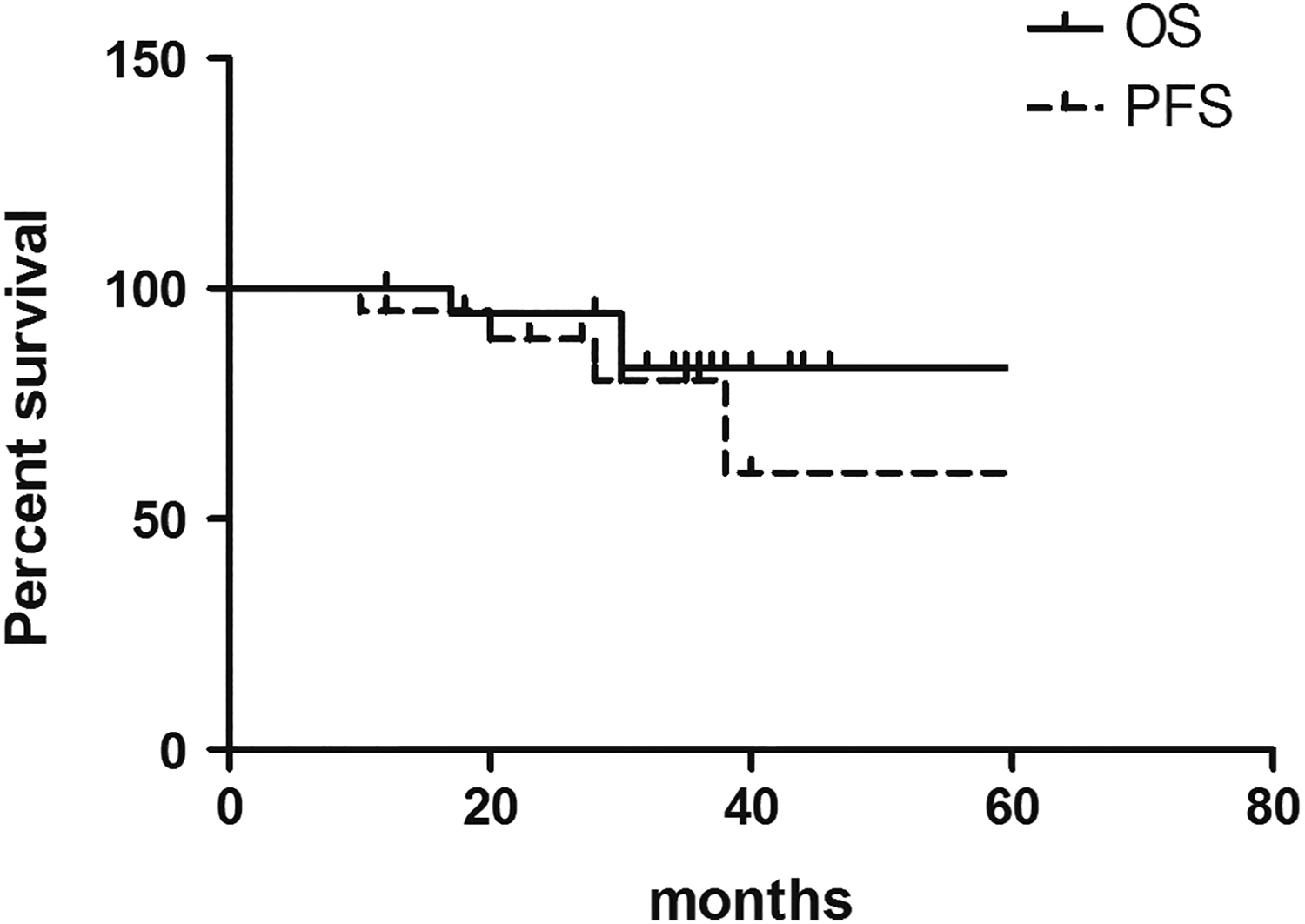
Overall survival (OS) and progression-free survival (PFS) rate of patients with extranodal involvements.
Positron Emission Tomography/CT and Prognostic Analysis
All of the patients enrolled in this study were evaluated by PET/CT. The average SUVmax of the extramedullary lesions was 15.0 (range: 3.0-30.0), where 9 patients had a SUVmax higher than the average. The highest SUVmax of the extramedullary lesions for each patient was analyzed against age, gender, DS stage, ISS stage, serum LDH, serum β2-MG, albumin, creatinine, Ca2+, and Ki-67 expression. The SUVmax of the extramedullary lesions was significantly correlated with Ki-67 expression (r = .789; P = .01) and serum β2-MG levels (r = .609; P = .004) but had no observed relationship with the other analyzed factors. No significant differences were observed between the OS and the SUV (P = .096), while the SUVmax of the extramedullary lesions was related to the PFS (P = .039).
Ki-67 and Prognostic Analysis
The Ki-67 ranged from 1% to 90% and averaged 35.0%, where the Ki-67 expression was lower than the average in 10 patients (see Supplementary Material Figure 2). The expression of Ki-67 in the extramedullary site with the highest SUVmax was analyzed against the age, gender, DS stage, ISS stage, and serum LDH, serum β2-MG, albumin, creatinine, and Ca2+ levels of the patient. The Ki-67 expression in patients who were diagnosed with a DS stage III was higher than stage I and II patients (P < .01). No significant relationship was observed between the OS and the Ki-67 expression (P = .064), but the PFS significantly correlated with Ki-67 expression (P = .009).
Finally, patients were stratified according to their SUVmax (≥15) and Ki-67 expression (≥35%), where each index was 1 score. Patients with an integral ≤1 and 2 were considered low and high risk, respectively. Finally, the 3-year OS and PFS were both higher in the low-risk group than in the high-risk group (OS: 100% vs 71.8%, P = .027, Figure 2; and PFS: 92.6% vs 34.1%, P = .014, Figure 3, respectively).

Overall survival (OS) rate of patients with extramedullary involvements. Patients were stratified according to their SUVmax (≥15) and Ki-67 expression (≥35%), where each index was 1 score. Patients with an integral ≤1 and 2 were considered low and high risk, respectively.

Progression-free survival (PFS) rate of patients with extramedullary involvements. Patients were stratified according to their SUVmax (≥15) and Ki-67 expression (≥35%), where each index was 1 score. Patients with an integral ≤1 and 2 were considered low and high risk, respectively.
To examine whether the effect on the prognosis of SUV and Ki-67 was affected by the treatment, patients with the same chemotherapy regimens (VADT or BD) were also stratified according to their SUVmax (≥15) and Ki-67 expression (≥35%), where each index was 1 score. Patients with an integral ≤1 and 2 were considered low and high risk, respectively. Finally, the 3-year OS and PFS were also higher in the low-risk group than in the high-risk group (P < .05, data not shown).
Discussion
Previous publications have reported the incidence of EMM to be 7% to 20% at presentation and 6% to 20% as the disease progressed. The overall incidence of EMM has increased in recent years, likely due to an increase in MM patient survival and the use of sensitive imaging modalities. 17 Importantly, the findings in this study are mainly consistent with previous studies. For example, similar to our patient population, EMM patients make up approximately 10.1% of patients with plasma cell tumors. For patients with MM, extramedullary involvement is an indicator of a poor prognosis. 4 The outcomes of the EMM patients in our study of a 5-year OS of 82.9% and PFS of 59.6% are better than in previous reports. To some extent, we speculate that EMM involving the liver and lungs may be related to a poor prognosis compared to those with EMM beside the bone, but it needs a large amount of data to evaluate this hypothesis.
Positron emission tomography/CT is a new technology that uses both functional and morphological capabilities to evaluate the extent and activity of tumors as well as directly visualize the tumor burden. In recent years, PET/CT has been used more frequently to evaluate hematological malignancies, especially in cases with lymphoma and myeloma. Positron emission tomography/CT is an important tool in predicting the survival of MM patients. 18 Zamagni et al 19 found that the presence of at least 3 focal lesions, an SUVmax greater than 4.2, and the presence of EMM on PET/CT in patients with MM predicted lower PFS, SUV > 4.2, and EMM were also correlated with shorter OS. In our study, an SUVmax greater than 15 had a negative correlation with the PFS of patients with EMM. However, there were few studies published on evaluating the prognosis of patients with EMM, and, therefore, further research is required to support our conclusions. It has been shown that patients with EMM have a poor prognosis, and EMM is more often seen on PET/CT. In a meta-analysis that included 2 studies on isolated EMM, PET/CT had a sensitivity of 96% and a specificity of 77.8% for detecting EMM, which was higher than that for detecting intramedullary lesions.
Ki-67 is a nuclear protein that is expressed in every phase of the cell cycle of proliferating cells but is absent in G0 cells. Therefore, it is widely used as a marker of tumor proliferation 20 and is a significant predictor of the prognosis in patients with MM. The level of Ki-67 expression is closely related to the disease progression. 21 Alexandrakis MG 11 reported that patient survival was higher when Ki-67 was less than 8%. Reports on Ki-67 expression in EMM are lacking, but in our study, Ki-67 expression lower than 35% was significantly correlated with a better EMM patient PFS.
In our study, an increase in 18F-FDG uptake correlated with Ki-67 expression in patients with EMM, which is consistent with many studies on the relationship between 18F-FDG uptake and Ki-67 expression in patients with lymphoma. 22 -24 Many studies have shown that 18F-FDG uptake and Ki-67 expression can be used to accurately evaluate the prognosis of patients with lymphoma. 25 -27 However, the SUVmax of the extramedullary involvements and Ki-67 expression alone were unsuitable for evaluating the prognosis of patients with EMM in our study, and combining these values can be used to accurately evaluate the prognosis of EMM patients. The SUV value and Ki-67 expression showed great importance in the diagnosis of MM, they can reflect the proliferation and invasion of MM cells, clinical judgment for tumor proliferation activity, estimate prognosis, and provide important basis for treatment.
In conclusion, PET/CT is a useful tool for the initial staging of EMM and detecting disease sites. Patients with MM involving extramedullary involvement at presentation may have poor outcomes than those without extramedullary involvement. In addition, joint use of the SUVmax and Ki-67 expression can be used to accurately evaluate EMM patient prognosis. Limitations of our study include a small sample size, retrospective study design, and a lack of analysis of treatment factors. Therefore, in-depth research is needed to confirm our conclusions.
Supplemental Material
supplementary_materials_(4) - Correlation Between Uptake of 18F-FDG During PET/CT and Ki-67 Expression in Patients Newly Diagnosed With Multiple Myeloma Having Extramedullary Involvement
supplementary_materials_(4) for Correlation Between Uptake of 18F-FDG During PET/CT and Ki-67 Expression in Patients Newly Diagnosed With Multiple Myeloma Having Extramedullary Involvement by Qian Li, Jing Ma, Han Li, Wengui Xu, Zeng Cao, Su Liu, Lin Chen, Shuang Gao, Tinghui Yan, Dongying Li, Xue Wang, Yuanfang Yue, Zhigang Zhao, Xiaofang Wang, Hongliang Yang, Haifeng Zhao, Yong Yu, Yizhuo Zhang, Feiyue Fan and Yafei Wang in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
Q.L. and J.M. contributed equally to this work. This article does not contain any studies with human or animal subjects performed by any of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the key technologies R & D program of Tianjin under Grant 13ZCZCSY20300; Science and Technology Project Affiliated to the Education Department of Tianjin under Grant 20140112.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.