
Abstract
Background
One major challenge when inserting a tunneled, cuffed central venous catheter (CVC) for hemodialysis under fluoroscopy is to accurately place the catheter tip by assessing its position in relation to the cardiac silhouette to approximate the right atrium (RA).
Purpose
To investigate whether a weighted mean calculated from published results for two two-dimensional landmark reference distances may be useful in assessing CVC tip positions in relation to the RA.
Material and Methods
Central venous catheter tip positions attained under fluoroscopic imaging during insertion using the cardiac silhouette as approximation were retrospectively related to two reference distances (carina to cranial RA border and craniocaudal RA extent), which were used to group catheter tip locations above (1), within (2), or below (3) the RA (henceforth referred to as landmark technique approximation, LTA). The LTA-derived catheter tip locations were validated by correlation with postinterventional computed tomography (CT) datasets acquired shortly after implantation (if available).
Results
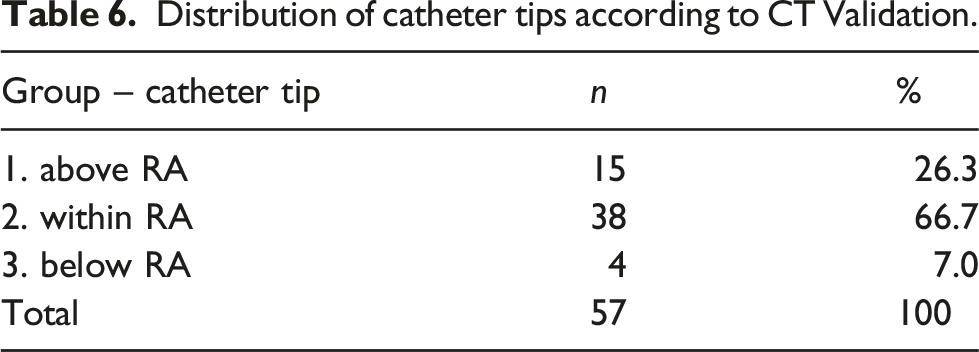
Based on LTA, 45 catheter tips (10.6%) were above, 179 (42.2%) within, and 200 (47.2%) below the RA. Postinterventional CT (n = 57; 13.4%) visualized 26.3% above, 66.7% within, and 7.0% below the RA.
Conclusion
The LTA reference distances appear to lead to a rather low categorization of the CVC tips, or the tips have been placed rather low in the study population. Validation using postinterventional CT indicated an underestimation of the RA in the LTA. Patient characteristics with a higher risk of false estimation through LTA have been defined.
Introduction
Tunneled, cuffed central venous catheters (CVCs) are frequently used for hemodialysis (HD). To ensure sufficiently high HD flow, the tip should be at the level of the mid-right atrium (RA). 1 Accurate placement of the tip for efficient hemodialysis is a major challenge when inserting a CVC under fluoroscopy and requires assessment of tip position in relation to the RA. Using the two-dimensional cardiac silhouette and other landmarks like the trachea and its carina, while taking into consideration possible factors altering tip position (e.g. upright versus prone body posture, breathing condition in inspiration or expiration, body mass index, and insertion site), the optimal catheter tip position in relation to the RA can be approximated on peri-interventional fluoroscopic imaging.
The objectives of this retrospective study were to 1. assess postinterventional catheter tip positions attained with fluoroscopic imaging during the insertion procedure using the cardiac silhouette and other landmarks like the trachea and its carina as approximation and compare outcomes with post hoc tip positions determined using the weighted means of published data for two two-dimensional landmark reference distances (landmark technique approximation, LTA) to group CVC tip positions as above (1), within (2), or below (3) the RA and 2. use CT images for validation of catheter positions that underwent postinterventional CT with the catheter still in place, when available.
Material and methods
Database query, study population and vascular access site
A retrospective database query was performed to identify patients who underwent CVC procedures in an interventional radiology unit of a German University Hospital. The search identified 664 patients, who were then assessed for exclusion criteria (see Figure 1). CVC interventions (n = 664) identified by database query and flowchart of exclusion. The search identified 432 eligible tunneled, cuffed CVC insertions. Eight patients had to be excluded because the catheter tip could not be measured. Final analysis included 424 CVC insertions that could be classified by tip position in relation to the RA (above, within, or below). CVC: central venous catheter; RA: right atrium
Demographic and relevant clinical information was extracted from postinterventional clinical reports, the Radiology Information System (Centricity Ris-I 5, Version 5.0.9.11, GE, Boston, Massachusetts, USA) and the Picture Archiving and Communication System (PACS Version 3.2, GE Medical Systems, Milwaukee, WI, USA).
Types of catheter
The catheters used were categorized into two groups, catheter type 1 (Palindrome™, Medtronic GmbH, Earl-Bakken-Platz 1, 40670 Meerbusch, Germany) and catheter type 2 (HemoStar®, C. R. Bard GmbH, Wachhausstraße 6, 76227 Karlsruhe, Germany).
Landmark technique approximation
An approach termed landmark technique approximation (LTA) was used to determine and classify catheter tip positions as above (1), within (2), or below (3.) the RA. (Figure 2) This technique involved the use of two weighted means calculated from published results for the following two-dimensional landmark reference distances: • from the carina to the cranial border of the RA, also known as the superior vena cava-RA transition (Table 1)—to approximate the upper border of the RA on the fluoroscopic image2–6 and • the craniocaudal extent of the RA (Table 2)—to approximate the lower border of the RA on the fluoroscopic image (in combination with the aforementioned cranial border of the RA).7–10 Fluoroscopic depiction after tunneled, cuffed CVC insertion with catheter tip location in relation to the RA (a), with real metric distances measured according to the approximated landmark technique reference distances of 5.3 cm (carina to cranial ending of RA) and 4.5 cm (craniocaudal extent of the RA); (b), and schematic depiction of relevant anatomy, reference distances and possible catheter tip locations in relation to the RA (c), including respective groups (above, within and below the RA). SVC: superior vena cava; IVC: inferior vena cava; CVC: central venous catheter; RA: right atrium. (Measurements performed by dropping a craniocaudal perpendicular from the carina on the fluoroscopic image). Carina to cranial RA border. Published distances used to calculate a weighted mean as reference distance. Craniocaudal RA extent. Published distances used to calculate a weighted mean as reference distance.



The datasets were validated by an expert reader (interventional radiologist >6 years of experience).
Postinterventional CT—validation of catheter tip positions
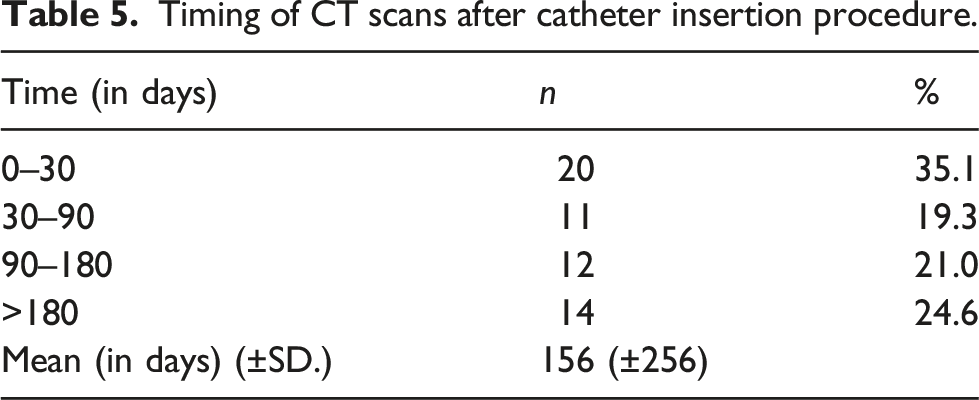
Catheter tip positions were validated by correlation with postinterventional computed tomography (CT) datasets acquired shortly (Table 5) after implantation with the catheter still in place (in patients where this examination was performed). The CT datasets were evaluated by an expert reader (interventional radiologist >6 years of experience).
Statistical analysis
Statistical analysis was performed with IBM/SPSS Statistics 24 (International Business Machines Corp., New York). Non-normal distribution was assumed, and non-parametric tests were performed. Descriptive statistics are given as frequency and percentage for categorical variables. Quantitative parameters are presented as mean (± standard deviation) and median. p-values are reported with the confidence interval set at 95%.
Results
Descriptive statistics
Study population demographics.

LTA-Approximation
Distribution of catheter tip positions estimated using landmark technique approximation (LTA) - grouped into above, within, and below the RA.

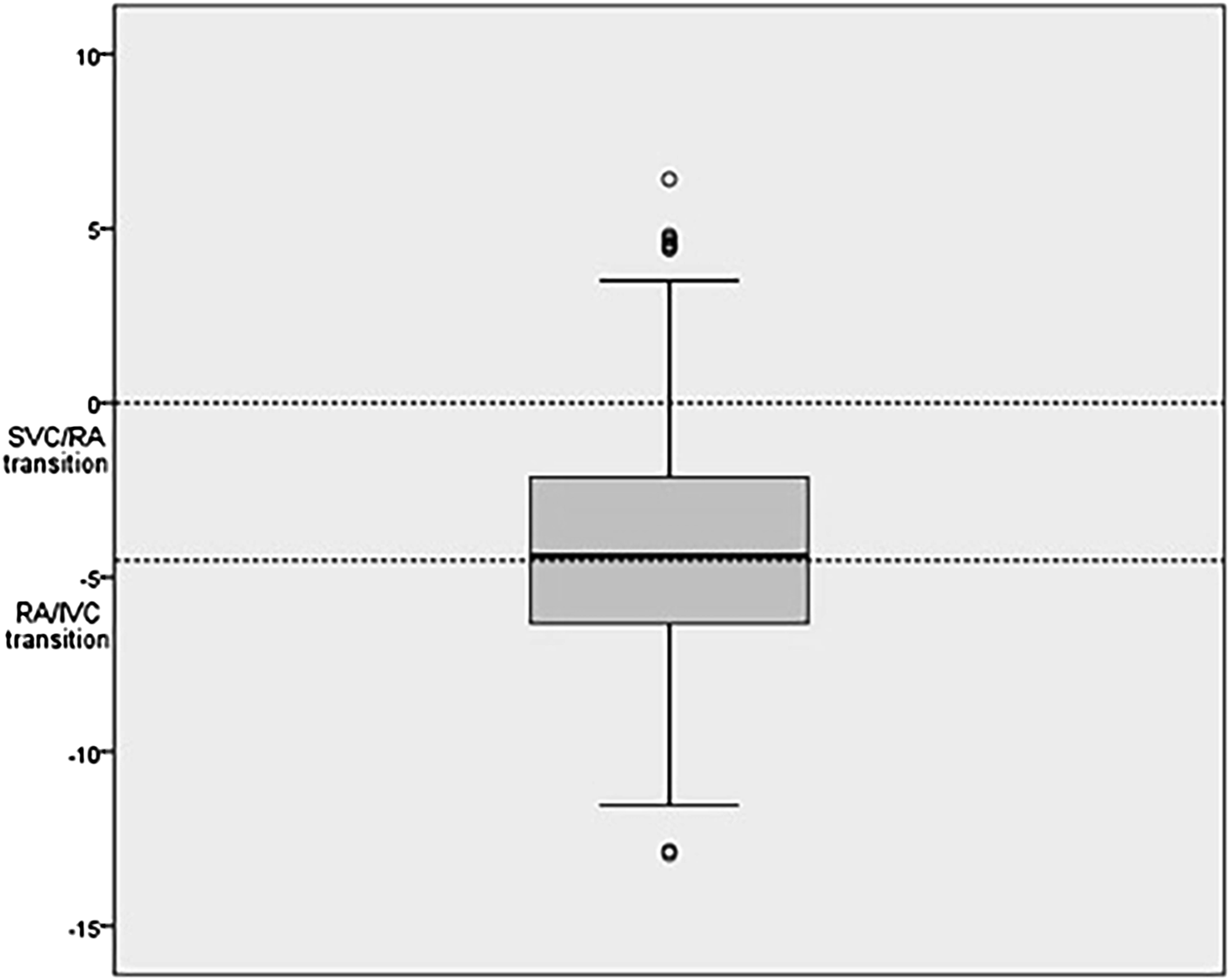
Boxplot of all catheter tip positions in relation to the cranial border of the RA (SVC/RA) and the caudal border of the RA (RA/IVC) approximated with reference distances by landmark technique (LTA) (n = 424). Y-axis in cm, calibrated with 0 at SVC/RA transition. IVC: inferior vena cava; SVC: superior vena cava; RA: right atrium.
Postinterventional CT Validation
Timing of CT scans after catheter insertion procedure.
Distribution of catheter tips according to CT Validation.
Subgroup analysis
Subgroup analysis of discrepant fluoroscopy/LTA and CT catheter tip positions: patient characteristics.

Note: LTA: landmark technique approximation.
Discussion
In this study, postinterventional catheter tip positions attained with fluoroscopic imaging during the insertion procedure were post hoc related to a weighted mean of published two-dimensional landmark reference distances (landmark technique approximation, LTA).
Using literature-derived weighted reference distances of 5.3 cm (carina to cranial border of RA; Table 1) and 4.5 cm (craniocaudal extent of RA; Table 2), LTA (Figure 2) found 10.6% of catheter tips (n = 424) to be located above the RA (1), 42.2% within the RA (2) and, rather surprisingly, 47.2% below the RA (3). These findings can be interpreted as follows: Either LTA was precise and catheter tips of the inserted cuffed, tunneled CVC have a tendency of being placed rather low in the given study population (I) or the landmark approximation may itself have led to lower catheter tip estimates in relation to the RA (above, within or below), than was actually the case (II).
Regarding condition I, many experienced interventionalists involved in treating the study patients, while targeting the mid-right atrium, opt to position the tip rather below this level than above with the patient supine (see Figure 3). Nazarian et al. report that a catheter tip can migrate significantly from its initial position at the time of placement compared to its position on upright follow-up chest radiographs (mid-right atrium initially, to low superior vena cava on follow-up). 11 Further, a change in tip position due to arm movement can result in an average displacement of 3.2 cm (+/− 1.8); as a result, the catheter tip could migrate into the SVC. 12 Other causes of tip movement could be related to catheter pull back known to occur based on the extent of overlying soft tissues and gravity after the patient sits up or stands. For future prospective investigations, a possibility to mitigate the tip movement would be to apply the LTA method to CXR performed after the insertion procedure, ideally at the time of the CT scan. The mean time from intervention to CT for this population was 152 days. Whether this may support or refute the likelihood of significant changes in catheter position over time seems to depend mainly on the possibility of catheter migration over time. Since all dialysis catheters used featured a subcutaneous dacron cuff that grows tissue within three to 4 weeks in order to prevent the catheter from slipping out (and germs from entering the bloodstream), catheter migration seems rather unlikely. A deeper implantation could prevent adverse events associated with device migration into the SVC and has been recommended. 12
Condition II assumes that LTA systematically yielded lower catheter tip positions than may actually be the case, implying that reference distances are inaccurate or inapplicable. The reference distance of 5.3 cm (carina to cranial border of RA) would need to be shorter (to include more catheter tips of the 10.6% classified as lying above the RA) and, even more relevant for the study population investigated here, the reference distance of 4.5 cm (craniocaudal extent of RA) would need to be longer (to include more catheter tips of the 47.2% classified as lying below the RA). Although an extensive literature search was performed to identify available data on published distances, the data may still not be robust. Many published values were obtained using echocardiography, which holds true especially for the craniocaudal RA diameter.7–10,13–15 Therefore, one needs to consider that different imaging methods may not always yield consistent quantitative measurements. 16 To further account for condition II, the CT validation of the data available (sample size n= 57/424; 13.4%) showed more catheters above the RA (26.3% vs. 10.6%), more catheters inside the RA (66.7% vs. 42.2%), and less catheters below the RA (7.0% vs. 47.2%) in comparison to LTA. In this sample, the group below the RA is much smaller and the group above the RA is larger suggesting that the RA could be underestimated in the LTA or it needed to be shifted cranially to deliver results comparable to the CT measurements. It is worth emphasizing that postinterventional CT could only be analyzed retrospectively, when available. To minimize respiratory artifacts, the respiratory commands for the patients undergoing fluoroscopy and CT were standardized. During fluoroscopy, patients were asked to inhale and stop breathing before the image was taken, and during CT scan the same commands are integrated automatically and given directly prior to scan.
Because of the discrepant findings of tip positions between LTA and CT validation, a subgroup analysis was performed to define specific patient characteristics as possible risk factors for incorrect approximation when relying on fluoroscopy/LTA alone. A typical patient at risk in this subgroup received a catheter type 1 via left-sided access, was male, and younger than the average patient in the study population. This leads us to the conclusion that if these patient characteristics are met the interventionalist should keep the higher risk for false estimation via LTA in mind, and if in doubt of correct tip position, more diagnostics like CT could be considered to ensure the catheter tip is located at the recommended position, the RA.
Strict technical categorizations like above, within, or below the RA may not reflect actual anatomy with flowing transition areas, which can challenge individual assessment and exact measurement.17,18 Only interventions using an upper thoracic access were included, whereas femoral and translumbar access sites were excluded from analysis. No correlation between tip position and hemodialysis efficiency was performed. For completeness, other factors including age and sex were also investigated and had no measurable statistically relevant influence on tip position. Other methods such as echocardiography-correlated tip positioning yield promising success rates and minimize radiation. 19 In conclusion, postinterventional CT validation indicates that the LTA reference distances applied on fluoroscopic images may have led to a rather low categorization of CVC tips (condition II), instead of CVC tips having been placed rather low in the study population (condition I). Validation using available postinterventional CT indicated that a majority of the catheter tips were actually located within or above the RA, while LTA suggested a rather too low catheter tip position. Younger than average male patients, who received catheter type 1 via left-sided access were at higher risk for false estimation when tip position was attained via fluoroscopy/LTA and could be controlled via CT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.