
Abstract
Radioactive seed localization is a method widely used within breast cancer treatment. This case represents a 43-year-old male patient with a foreign body in his left axilla. We used radioactive seed localization for marking the foreign body, which made the subsequent surgery possible, quick, and minimal invasive.
Introduction
Radioactive seed localization (RSL) is a method of preoperative localization involving a small titanium seed containing radioactive iodine (I-125). In breast cancer treatment, RSL is widely used for localizing nonpalpable lesions, 1 as well as both the primary lesion but also metastatic axillary lymph nodes prior to neoadjuvant systemic treatment.2,3 RSL has been used outside breast surgery for localization of non-palpable lymph nodes in the axillary region, the head and neck region, and the inguinal region, 4 for localization of parenchymal lung lesions 5 and for localization of renal cell carcinoma in a patient with Von Hippel-Lindau disease. 6
The radioactive seed is preoperatively placed in or adjacent to the non-palpable lesion guided by ultrasound. Migration of the seed is found to be negligible (∼1 mm). 7 During surgery, the iodine seed is located with a handheld gamma-probe. The incision is made just above the lesion according to the auditory signal, or as in this case the radiologist can mark the skin closest to the foreign body (FB). The radioactivity is emitted from a small pin source permitting an accurate localization, and the gamma-probe allows for constant orientation during the procedure. Correct removal of the iodine seed is confirmed by measuring activity ex vivo and no remaining activity in the resection bed. Removal of the specimen with iodine seed can be confirmed by X-ray. The ultrasound guided placement of the seed can be done several days before surgery, which eases the logistics. Low rates of complications have been reported, 1 as well as high patient satisfaction compared to wire localization. 8
Retained FB can lead to secondary trauma and patient discomfort. Surgical interventions are often required for their removal. Usually, FBs lying just beneath the skin surface can be easily retrieved. When FBs lie deep in the soft tissues, it may lead to tissue damage, delayed wound healing, infection, chronic pain, allergic reactions, and late injury as a result of migration. 9 Surgical interventions for removal of such deep-lying FBs are highly time-consuming and involve higher levels of trauma to the surrounding tissue.
This case report describes the first experience of RSL for marking FB to make the subsequent surgery minimal invasive and less time-consuming.
Case Report
A 43-year-old male was 3 years earlier shot with an air rifle. He had a retained lead bullet in his left axilla. He developed a rash on his arms and legs and pain in his left hemithorax. The patient was convinced that his eczema was due to the lead bullet and wanted it removed. He was sent to the department of orthopedic surgery. He had a small scar, 2 × 2 mm, in the upper part of the anterior axillary line corresponding to the entrance of the shot. Palpation was normal though the patient was a little sore. X-ray of the thorax showed a lead bullet close to or in costa 6 (Figure 1). Subsequent CT scan of the thorax showed a foreign body between musculus pectoralis major and the fatty tissue in the axilla—not in relation to costae—18 mm from the skin surface. X-Ray of the thorax showing the lead bullet in the left side.
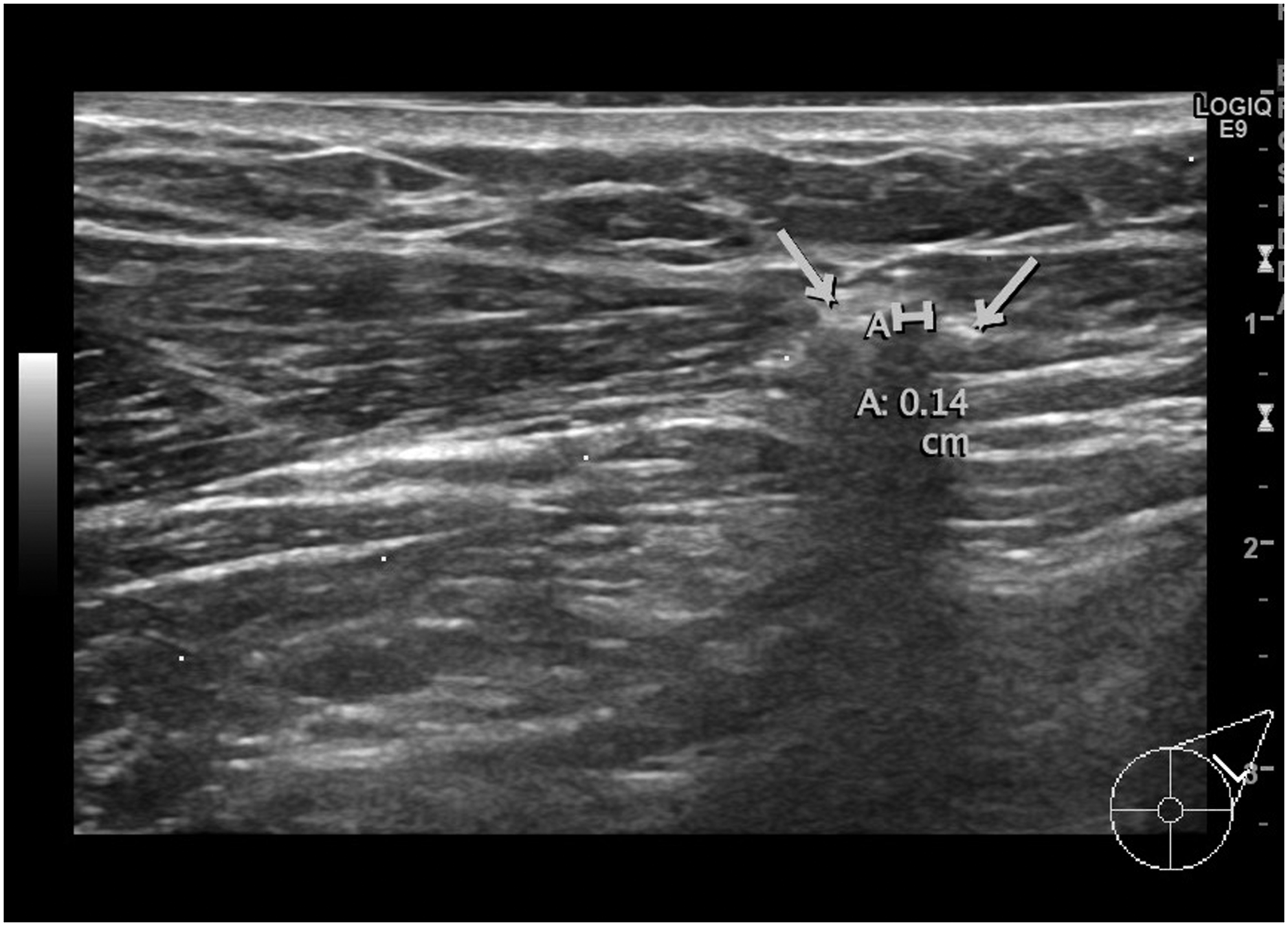
The patient was then referred to the department of breast surgery. Guided by ultrasound, the FB was identified (Figure 2) and marked with a radioactive seed. The marking was without discomfort to the patient. The ultrasound picture (Figure 3) shows the radioactive seed adjacent to the FB. Very rarely the radioactive seed is stuck to the stylet when it is retracted. To avoid this, the radiologist can twist the stylet before removing it. When the radiologist does the marking, there is pressure to the tissue by the ultrasound probe. Sometimes when this is released, the radioactive seed is seen displaced on the subsequent radiograph of the location. In this case, the radioactive seed was 15–20 mm lateral and caudal of the FB (Figure 4). Therefore, the radiologist also marked the skin above the FB about 20 mm cranial of the scar. Afterward, the FB was easily removed surgically guided both by the radioactive seed and the skin marking (Figure 5). The operating time was 25 min. The patient was discharged the same day. No complications occurred postoperatively. The lead bullet identified with ultrasound. Ultrasound-guided marking with radioactive seed. The bullet is marked with the arrow to the left and the radioactive seed with the arrow to the right. The distance between them is 1.4 mm. X-Ray showing both the lead bullet and the iodine seed. After removal. The lead bullet and the radioactive seed.


Technical details
The titanium seed measures 0.8 × 4.5 mm. In our institution, we use iodine seeds with an average activity of 0.207 MBq. The FB was visualized by ultrasound. The radioactive seed was introduced within an 18-gauche needle, guided near the FB and using a stylet moved into the soft tissue near the FB. An X-ray confirmed the exact position. After removal, the radioactive seed was placed in a shielded lead container before being returned to the department of nuclear medicine.
Discussion
This case report is to our knowledge the first to describe the use of RSL for removal of FB. RSL made the removal possible, quick, and uncomplicated.
The iodine seed used had an activity of 0.207 MBq, which leads to an absorbed maximum dose of 100 mGy to the surrounding tissue, believed to be acceptable for the patient. As the iodine seeds are regarded as sealed radioactive sources, all seeds must be traceable throughout the entire procedure, which requires extensive interdisciplinary collaboration. 10
RSL is widely used in breast surgery—both in the breast and the axilla. A feasibility study where RSL was tested in patients with suspect nonpalpable lymph nodes in the axillary region, the head and neck region, and the inguinal region concluded that RSL was indeed a feasible procedure. 4 All the nonpalpable lymph nodes were marked successfully using ultrasound and all were successfully localized and excised during surgery. The procedure was performed without complications in most of the cases. Another study has tested the use of RSL of lung lesions prior to video-assisted thoracic surgery with wedge resection. This study concluded that RSL of parenchymal lung lesions is a feasible technique with complication rates comparable to standard wire-guided localization. 5 Another case report has described the successful use of RSL for marking a renal cell carcinoma in a patient with multi-cystic kidney due to Von Hippel-Lindau disease. 6
Several studies describe the use of ultrasound-guided removal of soft tissue FBs.11–13 One of these measures the distance from the skin to the FB. In the 11 patients, where the procedure was successful, the distance from the skin to the FB was up to 13 mm. Only in one patient the ultrasound-guided procedure was unsuccessful and in this case the distance from the skin to the FB was 23 mm. 11 In our case, the distance was 18 mm. A case report describes the use of ultrasound-guided needle localization to aid FB removal. 12 The localization was done just before the surgery. Both localization and surgery were successful. With the use of RSL, the placement of the seed can be done days in advance and there is no risk of displacement.
We believe RSL can be used for marking foreign bodies and has the potential to improve treatment by easing both the marking and the surgical procedure. This may lead to reduced discomfort for the patient, reduced operating time, minimizing trauma to the surrounding tissue, and ultimately benefit the patient.
In conclusion, this case report presents a successful placement of an iodine seed improving the identification and removal of a deep-lying foreign body.
Footnotes
Author’s Note
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from The Department of Breast Surgery (APC), Herlev Hospital, Denmark.