
Abstract
Background
Echo-planar imaging (EPI)-diffusion-weighted imaging (DWI) may take unclear image affected by susceptibility, geometric distortions and chemical shift artifacts.
Purpose
To compare the image quality and usefulness of EPI-DWI and turbo spin echo (TSE)-DWI in female patients who required imaging of the pelvis.
Material and Methods
All 57 patients were examined with a 3.0-T MR scanner. Both TSE- and EPI-DWI were performed with b values of 0 and 1000 s/mm2. We compared geometric distortion, the contrast ratio (CR) of the myometrium to the muscle and the apparent diffusion coefficient (ADC) values for the myometrium and lesion. Two radiologists scored the TSE- and EPI-DWI of each patient for qualitative evaluation.
Results
The mean percent distortion was significantly smaller with TSE- than EPI-DWI (p = 0.00). The CR was significantly higher with TSE- than EPI-DWI (p = 0.003). There was a significant difference in the ADC value for the uterus and lesions between the EPI- and TSE-DWI (p < 0.05). Finally, the ADC values of cancer were significantly different from those for the uterus and benign with both the two sequences (p < 0.05). The scores for ghosting artifacts were higher with TSE- than EPI-DWI (p = 0.019). But there were no significant differences between TSE- and EPI-DWI with regard to image contrast and overall image quality.
Conclusion
TSE-DWI on the female pelvis by 3T MRI produces less distortion and higher CR than EPI-DWI, but there is no difference in contrast and image quality.
Introduction
Diffusion-weighted imaging (DWI) is a functional magnetic resonance imaging (MRI) sequence that reflects the diffusion of water molecules in tissues. DWI is rapidly becoming a standard MRI modality that can be used to obtain images of various parts of the human body, including the female pelvis. 1
Echo-planar imaging (EPI)-DWI is the most frequently used method due to the rapid readout sequence. However, the quality of female pelvic images acquired by EPI-DWI can be unsatisfactory due to intestinal tract air and peristalsis, 2 which tend to cause substantial magnetic susceptibility artifacts in images obtained with the EPI-based sequence. Because there is no refocusing radiofrequency (RF) pulse with the EPI-based sequence, the spinning protons accumulate phase errors that lead to magnetic susceptibility artifacts. Such artifacts often result in image distortion, signal dropouts, and signal heterogeneity that can lead to difficulty in reading DWI.
The turbo spin echo (TSE) method is an alternate approach for performing DWI. Because TSE-DWI uses a 180° RF refocusing pulse for each measured echo, susceptibility artifacts are smaller and image distortion is less marked than with EPI-DWI. While a lower signal-to-noise ratio (SNR) and a long acquisition time were previously disadvantages of TSE-DWI, recent commercial TSE-DWI sequences for 3T MRI units have adapted the RF pulse shape to reduce the echo space, which could result in faster scanning, a higher SNR, and reduced blurring.3,4
Therefore, this retrospective study was performed to compare the image quality and usefulness of EPI-DWI and TSE-DWI in patients who required imaging studies of the female pelvis.
Material and Methods
This retrospective study was approved by our Institutional Review Board and the requirement for informed consent was waived.
Patients
Between January and June 2019, 57 consecutive female patients aged 13–84 years (mean age: 49.5 years) with suspected or confirmed malignant tumors of the pelvis underwent EPI-DWI and TSE-DWI. Among them, 10 patients had histologically confirmed uterine cancer (five with endometrial cancer, four with cervical cancer, and one with carcinosarcoma). Twenty-three patients had histologically confirmed benign lesions (12 uterine myoma, 4 endometrial hyperplasia, and 7 benign ovarian lesions), and 24 patients had suspected benign lesions based on clinical course and repeat imaging (9 uterine myoma, 5 cervical cyst, 8 benign ovarian lesions, 1 urethral diverticulum, and 1 with no abnormal findings).
MRI protocol
MRI was performed with a 3T scanner (Philips Ingenia Elition 3T; Philips Medical Systems, Best, The Netherlands) using a 32-element anterior torso phased-array coil coupled with an integrated posterior 20-element array in the tabletop. All patients were taking anti-peristaltic agent.
The MRI protocol consisted of axial and sagittal T1-weighted imaging (T1WI), T2-weighted imaging (T2WI) in three orthogonal planes (transverse, sagittal, and coronal), dynamic contrast-enhanced sagittal T1WI, contrast-enhanced axial and coronal T1WI with fat suppression (FS), and axial EPI-DWI and TSE-DWI.
Axial TSE-T2WI was performed with the following parameters: repetition time (TR)/echo time (TE), 3000–8000/100 ms; slice thickness, 5 mm; inter-slice gap, 1 mm; number of slices, 20; field of view (FOV), 22 cm; number of signals acquired (NSA), 1; sensitivity encoding (SENSE) factor, 1; and total scan duration of 2 min.
We used a single shot echo-planar imaging sequence for EPI-DWI and a single-shot turbo spin echo sequence for TSE-DWI. When EPI-DWI and TSE-DWI are performed, a motion probing gradient pre-pulse is used to obtain a diffusion signal. We employed the same imaging parameters as much as possible for the two DWI sequences (Table 1). Especially, we tried to obtain equivalent spatial resolution images on the two DWI sequences.
Imaging parameters for DWI sequences.

DWI: diffusion-weighted imaging; EPI: echo-planar imaging; TSE: turbo spin echo; TR: repetition time; TE: echo time; FOV: field of view; SPAIR: spectrally adiabatic inversion recovery.
Diffusion-encoding gradients were applied at b values of 0 and 1000 s/mm2 in the three orthogonal directions of the motion-probing gradients before administration of contrast medium. Maximum intensity projection DWIs were reconstructed in the axial plane with 5 mm reconstruction voxels. Apparent diffusion coefficient (ADC) maps were automatically generated by using the manufacturer’s software.
Quantitative evaluation
A radiologist (R.Y.) with 14 years of experience who was blinded to the MRI protocols recorded data from the axial source images. We selected a representative slice that clearly depicted the acetabulum in each patient. Geometric distortion was evaluated by comparing lesion lengths between the axial TSE-T2WI and the corresponding DWI. The anterior-posterior (AP) body surface length and the left-right (LR) distance between the floor of both acetabula were measured, and the percent error was calculated as DWI distance – T2WI distance/T2WI distance × 100.
We also selected a representative slice that clearly depicted the uterus in each patient. The signal intensity was set for EPI-DWI and TSE-DWI to allow 30 mm2 circular regions of interest (ROI) to be placed on the uterine myometrium (uterus), the gluteal muscles and lesions.
The contrast ratio (CR) was determined as the ratio between the signal intensity (SI) of the uterus and the SI of the gluteal muscles (CR= | uterus SI − gluteal muscle SI |/| uterus SI + gluteal muscle SI |)
On each ADC parameter map, ADC values were measured by placing a circular ROI (30 mm2) on the uterine myometrium (uterus) and the lesion. When measuring the signal intensity and ADC, care was taken to only measure the target region without including structural borders or prominent vessels within an anatomic segment.
Qualitative evaluation
Two radiologists performed qualitative assessment of the DWI on an SDS DICOM Viewer (Techmatrix Ltd, Tokyo, Japan). The image data sets were randomized, and the readers were blinded to the acquisition parameters. Adjustment of the window level and width during qualitative assessment was allowed.
Qualitative evaluation was based on a 5-point Likert scale. Ghosting artifacts were rated as follows: 1 = definitely interfering with interpretation, 2 = possibly interfering with interpretation, 3 = present with little impact on interpretation, 4 = faint, or 5 = none. Image contrast was rated as follows: 1 = marked blurring without definable margins, 2 = blurring with definable margins, 3 = minimal blurring, 4 = sharp definition, or 5 = very sharp definition. Overall image quality was rated as follows: 1 = non-diagnostic, 2 = poor, 3 = acceptable, 4 = good, or 5 = excellent. Each reader independently assessed the EPI-DWI and TSE-DWI and decisions were made by consensus when there was divergence of opinion between them.
Statistical analysis
The Shapiro–Wilk test was used to determine whether mean values were normally distributed. Differences of mean values between EPI-DWI and TSE-DWI were analyzed by Wilcoxon signed rank test after confirming a normal distribution by using the Shapiro–Wilk test.
Inter-observer agreement between the two image assessors was estimated by using kappa statistics, with the following cutoff points for the level of agreement: 0–0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good; and 0.81–1.00, excellent. 5 The correlation between the reviewers’ scores was determined by the Kendall test. Qualitative scores were compared using the Wilcoxon signed-rank test.
The ADC values of each lesion on each DW were compared by using the Kruskal–Wallis test, followed by Mann–Whitney U tests with Bonferroni’s correction for multiplicity of testing.
All statistical analyses were performed with IBM SPSS version 22.0 for Windows (IBM Corp.: Armonk, NY), and a p value < 0.05 was considered to indicate significance.
Results
Quantitative analysis
The mean percent distortion was significantly smaller with TSE-DWI than EPI-DWI (AP length: 0.6% ± 0.6 vs. 1.7% ± 1.2; LR width: 1.4% ± 1.3 vs. 2.6% ± 1.9) (respectively, p = 0.00) (Fig. 1).

Box-and-whisker chart showing the geometric distortion evaluated by comparing lesion lengths between axial T2WI and the corresponding DWI. The mean percentage error of distortion was significantly lower on TSE-DWI than EPI-DWI (AP length: 0.6% ± 0.6 vs. 1.7% ± 1.2, LR width: 1.4% ± 1.3 vs. 2.6% ± 1.9) (p = .00). The boxes show the 25th–75th percentiles, and the horizontal line indicates the median value and × show the mean values.
The CR of the myometrium to the muscle was significantly higher with TSE-DWI than EPI-DWI (0.52 + 0.11 vs. 0.47 + 0.12, p = 0.003) (Fig. 2).

Box-and-whisker chart showing the association the CR between EPI-DWI and TSE-DWI. The CR of the myometrium to the muscle was significantly higher on TSE than EPI-DWI (0.52 ± 0.11 vs. 0.47 ± 0.12, p = 0.003). The boxes show the 25th–75th percentiles, and the horizontal line indicates the median value and × show the mean values.
There was a significant difference of the ADC value for the uterus between the two sequences (1.49 ± 0.22 × 10−3 mm2/s with EPI-DWI vs. 1.40 ± 0.23 × 10−3 mm2/s with TSE-DWI, p = 0.002). Significant differences of the ADC values for lesions were also noted between each sequence (malignant lesions: 0.81 ± 0.07 × 10−3 mm2/s with EPI-DWI vs. 0.84 ± 0.08 × 10−3 mm2/s with TSE-DWI, p = 0.043; benign lesions: 1.60 ± 0.64 × 10−3 mm2/s with EPI-DWI vs. 1.52 ± 0.60 × 10−3 mm2/s with TSE-DWI, p = 0.00). Finally, the ADC values of malignant lesions were significantly different from those for the uterus and benign lesions with both EPI-DWI (uterus: 1.49 ± 0.22 × 10−3 mm2/s, benign lesions: 1.60 ± 0.64 × 10−3 mm2/s, malignant lesions: 0.81 ± 0.07 × 10−3 mm2/s; all p < 0.05) and TSE-DWI (uterus: 1.40 ± 0.23 × 10−3 mm2/s, benign lesions: 1.52 ± 0.60 × 10−3 mm2/s, malignant lesions: 0.84 ± 0.08 × 10−3 mm2/s; all p < 0.05) (Fig. 3).

Box-and-whisker chart showing the association the ADC between uterus, the benign lesions, and malignant lesions on EPI-DWI and TSE-DWI. There were significant differences in the ADC values of uterus, the benign lesions, and malignant lesions on each sequence (#p < .05). Moreover, there were significant differences in the ADC of malignant lesions from uterus and benign lesions on each sequence (
Qualitative analysis
The scores for ghosting artifacts were higher with TSE-DWI than EPI-DWI (3.1 ± 0.4 vs. 2.8 ± 0.8, p = 0.019). However, there were no significant differences between TSE-DWI and EPI-DWI with regard to image contrast (3.4 ± 0.6 vs. 3.2 ± 0.5, p = 0.073) and overall image quality (3.6 ± 0.6 vs. 3.4 ± 0.7, p = 0.110) (Table 2) (Figs. 4 and 5).
Qualitative scores between the two reviewers.

DWI: diffusion-weighted imaging; EPI: echo-planar imaging; TSE: turbo spin echo.
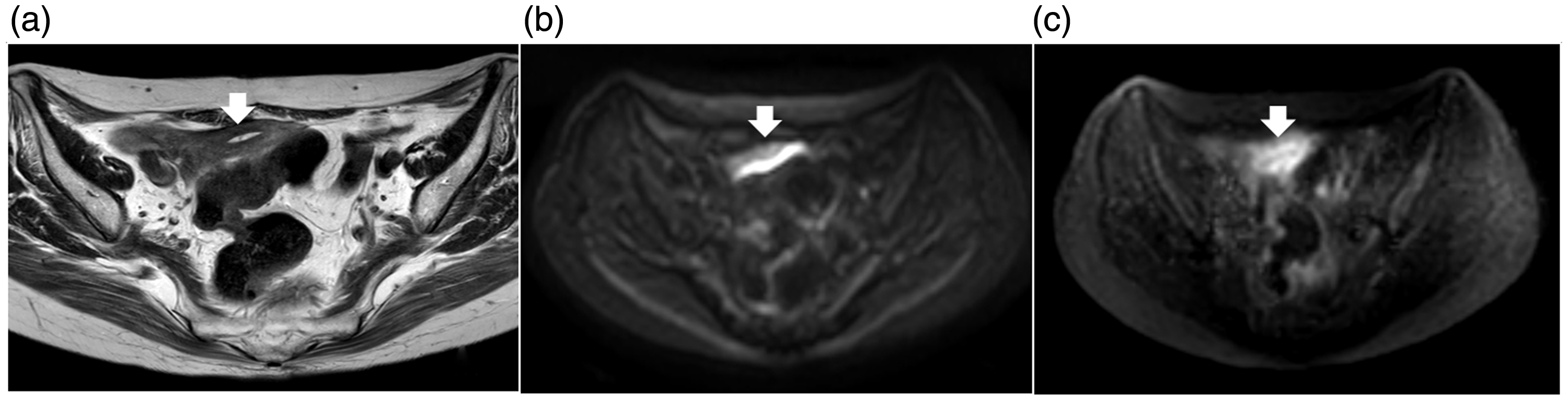
A 64-year-old female with uterus cervical cysts. (a) T2WI, (b) EPI-DWI, (c) TSE-DWI. A uterus (arrow) is difficult to identify on the EPI-DWI image (b), whereas it is detectable on the TSE-DWI (c). The distortion at the air interface is obviously seen on EPI-DWI in comparison to that on TSE-DWI.

A 68-year-old female with uterus cervical cancer. (a) T2WI, (b) EPI-DWI, (c) TSE-DWI. Intestinal gas is causing artifact (arrow) to a uterine cervical cancer (arrow head) on the EPI-DWI image (b). Intestinal gas is not causing artifact to a uterus cervical cancer (white arrow head) on the TSE-DWI (c).
The median kappa statistics between the two reviewers were moderate: EPI-DWI 0.540 (95% confidence interval (CI), 0.398–0.681) and TSE-DWI 0.492 (95% CI, 0.341–0.643). The average Kendall r correlations were significantly positive (EPI-DWI: r = 0.665, p < 0.001; TSE-DWI: r = 0.648, p < 0.001).
Discussion
We found that TSE-DWI on the female pelvis by 3T MRI produces less distortion, and higher CR than EPI-DWI, though TSE-DWI required a longer acquisition time than EPI-DWI to obtain equivalent spatial resolution images. In qualitative analysis, the scores for ghosting artifacts were higher with TSE-DWI than EPI-DWI, but image contrast and overall image quality had no significant differences between the two DWI sequences. Therefore, based on our findings, in the female pelvis by 3T MRI, TSE-DWI obtained a stronger signal with less distortion than EPI-DWI, but the contrast and image quality were almost the same as EPI-DWI.
DWI assesses random microscopic movements of water molecules and other small molecules elicited by thermal collisions, which means that rapid image acquisition minimizes the effects of bulk movements such as vessel pulsation. 6 The EPI sequence is a type of gradient echo sequence that represents the fastest MR image acquisition method (<100 ms/slice). It uses rapid phase oscillation and frequency gradients that generate multiple gradient echoes. 7 As each echo is acquired with a different echo time, blurring artifacts occur in the phase encoding direction due to loss of the signal from later echoes because of T2∗ decay. This tends to result in low spatial resolution of images obtained with a short acquisition time. Also, there are no RF refocusing pulses in the EPI sequence, leading to accumulation of phase errors for spinning protons that produce position errors in the phase-encoding direction and result in significant distortion. These effects are particularly prominent in anatomical regions with air-tissue interfaces.
The TSE sequence is another rapid imaging method in which multiple echoes are acquired with each excitation, 8 and it can also be used for DWI. Blurring of images can occur as with the EPI sequence. However, there is less severe blurring with TSE than EPI sequences because the T2 relaxation time is much longer than the T2∗ relaxation time and magnetic field inhomogeneity is reduced by the RF refocusing pulses. In addition, these RF pulses prevent accumulation of phase errors and image distortion. Previous reports have suggested that a decrease of the SNR and a long acquisition time are disadvantages of TSE-DWI.8,9 However, recent commercial TSE-DWI sequences for 3T MRI have modified the RF pulse shape to reduce the echo space, which is expected to result in faster scanning with a higher SNR and less blurring.
Our findings in this study suggested that the CR of TSE-DWI was superior to EPI-DWI for imaging of the female pelvis, because of less geometric distortion and signal loss due to propagation of susceptibility artifacts in the phase encoding direction. 10 These distortions increase with longer gradient echo times and mimic encoding of spatial information during image reconstruction. TSE-DWI uses an RF refocusing pulse for each measured echo, which reduced susceptibility artifacts on images of the female pelvis. However, in qualitative analysis, though the ghosting artifacts of TSE-DWI showed significant improvement compared to that of EPI-DWI, image contrast and overall image quality had no significant differences between the two DWI sequences. In the female pelvis by 3T MRI, though TSE-DWI required an acquisition time twice as long as EPI-DWI to obtain images of equivalent spatial resolution, it is a clinical disadvantage of TSE-DWI.
However, in this study, TSE-DWI (5:29 min) required twice longer acquisition time than EPI-DWI (2:08 min) to obtain equivalent spatial resolution images which is the clinical disadvantage of TSE-DWI. The female pelvis by 3T MRI may also reduce quality of DWI due to intestinal peristalsis. Therefore, though TSE-DWI required a longer acquisition time, TSE-DWI is useful when EPI-DWI cannot obtain good images due to intestinal artifacts in female pelvis by 3T MRI.
Reproducibility of ADC values is important for comparison of different imaging techniques. Therefore, we compared the ADC values between EPI-DWI and TSE-DWI, revealing a statistically significant difference in ADC values. However, the ADC values of malignant lesions were significantly lower than those of the uterus and benign lesions with both sequences, which was similar to the results of previous studies.2–4,9,10 Image noise can significantly influence the calculation of diffusion parameters, with the parameters showing lower values as noise increases. 11 The CR was higher with TSE-DWI compared to EPI-DWI. Thus, ADC measurements of the female pelvis obtained with TSE-DWI might be more accurate than those obtained with EPI-DWI. The chief disadvantage of TSE-DWI is a longer acquisition time compared with EPI-DWI. TSE sequences include an RF refocusing pulse in read/out, so this method will necessarily take longer than EPI. 12 However, our findings suggest that the TSE-DWI sequence may be particularly useful for improving image quality with 3T and higher-field MR systems.
Our study had some limitations. First, it was a single-center study and the patient population was small. We did not evaluate diagnostic accuracy because we focused on comparing the image quality between different acquisition protocols. Therefore, our findings and conclusions should be interpreted as preliminary and need to be confirmed by further investigation. Second, we cannot extrapolate data acquired with a 3T scanner to 1.5T systems. Susceptibility artifacts are less problematic with 1.5T scanners because these scale directly with the magnetic field strength, suggesting that the advantages of TSE-DWI over EPI-DWI may be smaller when images are acquired at 1.5T. However, distortion of female pelvic images was much lower with TSE-DWI than EPI-DWI. Third, different scanning parameters were employed for the two DWI sequences. Theoretically, it would have been better to use identical parameters. However, we used clinically applicable sequences and performed imaging within a limited time in the routine clinical setting.
In conclusion, based on our findings, TSE-DWI on the female pelvis by 3T MRI produces less distortion and higher CR than EPI-DWI, but there is no difference in contrast and image quality. When an EPI-DWI sequence does not provide an adequate image due to artifacts, a TSE-DWI is useful although it requires a longer acquisition time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.