
Abstract
Background
In congenital clubfoot, the lower leg is very thin and the calf muscles are hypoplasic. However, there are few studies reporting real muscle volume.
Purpose
The purpose of this study is to assay the muscle volume in congenital clubfoot using 3DCT and to quantify the degree of the hypoplasia.
Material and methods
From January 2015 to December 2016, nine consecutive patients, seven male and two female, with unilateral congenital clubfeet were recruited for CT scans. Axial transverse sectional CT scans were acquired from the delineation of the fibular head to the tibial plafond. From the data, we rendered the entire muscle in 3D for muscle volume assay, and further segmented the posterior musculature for comparison between the normal and affected sides.
Results
The whole muscle volume on the normal side was 291.23 cm3 (181.23–593.49) and that on the affected side was 225.08 cm3 (120.71–429.08), for an affected side to normal side ratio of 0.79 (0.72–0.9), which was significantly smaller (p < .01). Posterior muscle volume on the normal side was 175.81 cm3 (103.72–376.32) and that on the affected side was 106.52 cm3 (58.3–188.39). The ratio of posterior muscle to whole muscle on the normal side was 0.62 (0.46–0.75), and that on the affected side was 0.48 (0.4–0.55), such that the affected side was significantly smaller (p < .01)
Conclusion
This study contributes quantitative data supporting the longstanding observations that the posterior calf muscles are significantly smaller on the affected side compared to the normal side in congenital clubfoot, and further underscores the importance of the extending the excursion of these muscles.
Keywords
Introduction
In congenital clubfoot, the lower leg is very thin and the calf muscles are hypoplasic. This was described by Ponseti, but the cause is not well understood. 1 In unilateral cases, growth on the affected side is poor compared to the normal side and the hypoplasia pathology seems to affect the gastrocnemius, soleus, peroneal, tibialis posterior, flexor hallucis longus and flexor digitorum longus muscles.2–5 However, there are few studies reporting real muscle volume. The purpose of this study is to assay the muscle volume in congenital clubfoot using 3DCT and to quantify the degree of the hypoplasia.
Material and methods
From January 2015 to December 2016, nine consecutive patients, seven male and two female, with unilateral congenital clubfeet were recruited for CT scans. Six patients were affected on the right side and three on the left. None had neuromuscular disease, paralysis or other underlying conditions. All patients had received Ponseti method treatment within 3 months of birth. Three of the cases were relapse cases after initially successful treatment. Average age was 4 years old (1–8 years). This study was approved by our institution’s ethics review board and informed consent for use of anonymized data in medical research was obtained from parents of all patients.
Axial transverse sectional CT scans were acquired from the delineation of the fibular head to the tibial plafond. From the data, we rendered the entire muscle in 3D for muscle volume assay, and further segmented the posterior musculature for comparison between the normal and affected sides. The posterior musculature was defined as all muscle mass posterior to a coronal plane intersecting the posterior edges of the tibia and fibula on each CT image (Figure 1(a)–(c)). The CT scans were acquired using the Aquilion One 320 multislice CT (TOSHIBA medicals), and the analysis was performed with Aze Virtual Place Workstation (Canon). For the delineation of muscle tissue, the workstation threshold was set at 0-100 HU. A paired t-test was utilized to identify changes between the time points, with significance set at p ≦ .01. (a) Area of measurement/from the delineation of the fibular head to the tibial plafond. (b) 3DCT/3D reconstruction of delineated muscles. (c) Definition of the posterior muscle/posterior muscle group defined as all-muscle mass posterior to a coronal plane intersecting the posterior edges of the tibia and fibula on each CT.
Results
Patient demographics and muscle volume.
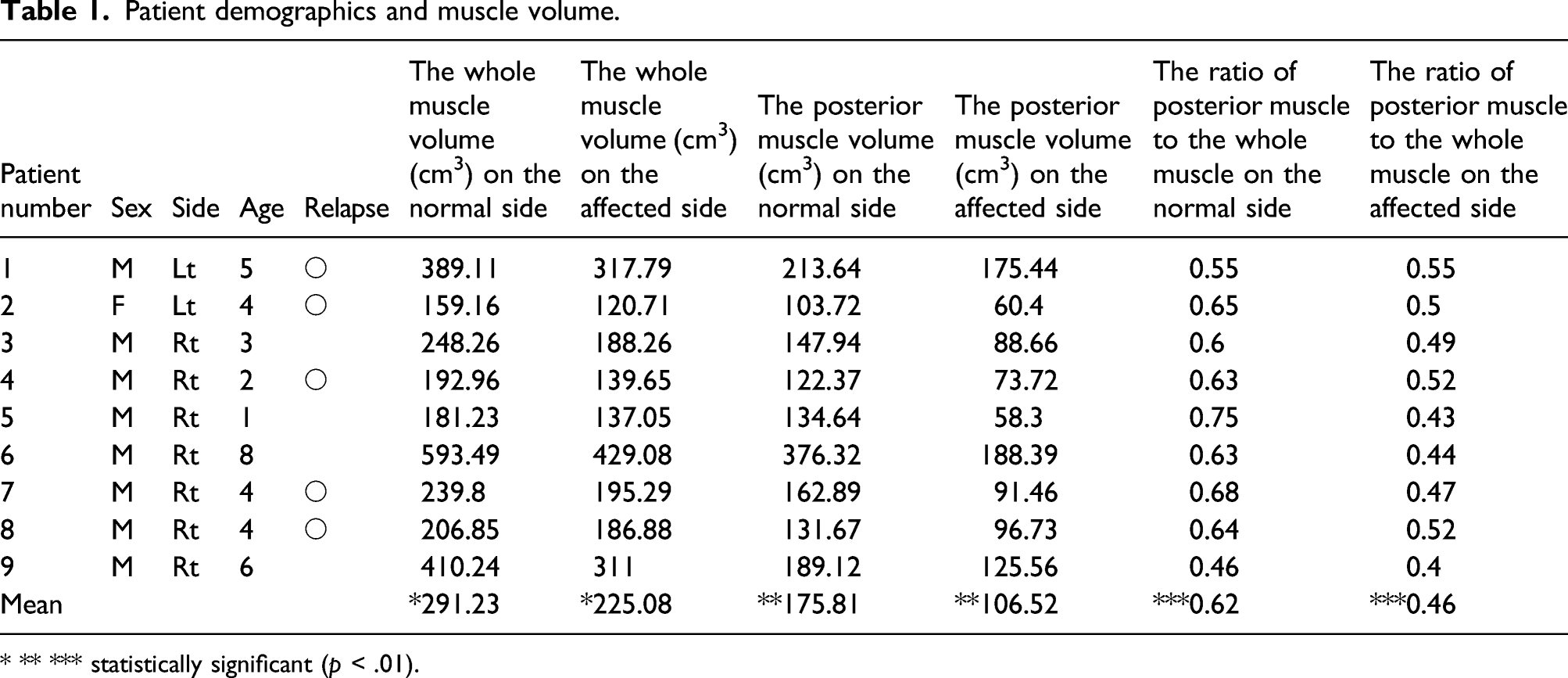
* ** *** statistically significant (p < .01).
Discussion
Much remains unknown regarding the causes of idiopathic congenital clubfoot. In recent years, considerable investigation has been conducted regarding the genetic factors but many questions remain.6–9 However, thin hypoplastic lower leg muscles are consistently observed. 1
Shimode et al. 10 measured tibia length and calf girth in a congenital clubfoot cohort and reported that tibia length and calf circumference were smaller in patients that had received surgery.
A number of studies have effectively used MRI in the investigation of congenital clubfoot pathology.2–5,11–17 Moon et al. used MRI for their investigation of treatment-resistant clubfoot and found muscle atrophy of the lower leg. Their investigation also revealed that extensive soft-tissue abnormalities were more prevalent in patients with treatment-resistant clubfoot, and particularly, a significantly greater difference was seen in intra-compartment fat area between the affected and unaffected limbs, compared with treatment-responsive clubfoot. 5 However, the use of MRI with small children frequently requires sedation. In this study, we used CT for our evaluation of muscle. We could not find any literature reporting clubfoot muscle quantification using CT. We were able to measure muscle volume by extrapolating the data to 3D and found lower leg muscle volume as a whole to be 20% less, and posterior muscle volume to be 40% less in the affected side when compared to the normal side. These findings confirmed underdevelopment in the muscles of the affected lower extremities in congenital clubfoot and that hypoplasia is particularly marked in the posterior flexors of the lower leg. Where hypoplasia is present in the soleus or gastrocnemius, not only is muscle volume decreased but the muscle excursion also decreases. In effect, this also shortens the excursion of the Achilles tendon. This would support the consensus that the underdevelopment and atrophy of the calf muscles contribute significantly to hindfoot varus and equinus in congenital clubfoot. This would also help explain the efficacy of Achilles tendon elongation often used in the Ponseti method of conservative clubfoot treatment.
In this study, no significant difference was found in the comparison between relapse cases to non-relapse cases, but there were very few cases so this needs to be revisited in a larger study.
In this study, we used CT scans which can be acquired more quickly than MRI scans and with no need for sedation, but radiation exposure is a drawback. Optimization of technical parameters for CT scan acquisition, and tracking metrics for dose management are important ongoing efforts. 18 In addition to the above-mentioned, the small number of subjects and the need for advances in radiation exposure reduction, study limitations include the inability to divide and measure each muscle individually due to the small size of these muscles in children with congenital clubfoot. We would also like to measure the strength of these muscles. In the future, more dynamic biomechanical analysis is needed.
In conclusion, this study contributes quantitative data supporting the longstanding observations that the posterior calf muscles are significantly smaller on the affected side compared to the normal side in congenital clubfoot, and further underscores the importance of the extending the excursion of these muscles.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.