
Abstract
Background
The presence of malignant cells in bone biopsies is considered gold standard to verify occurrence of cancer, whereas a negative bone biopsy can represent a false negative, with a risk of increasing patient morbidity and mortality and creating misleading conclusions in cancer research. However, a paucity of literature documents the validity of negative bone biopsy as an exclusion criterion for the presence of skeletal malignancies.
Purpose
To investigate the validity of a negative bone biopsy in bone lesions suspicious of malignancy.
Material and Method
A retrospective cohort of 215 consecutive targeted non-malignant skeletal biopsies from 207 patients (43% women, 57% men, median age 64, and range 94) representing suspicious focal bone lesions, collected from January 1, 2011, to July 31, 2013, was followed over a 2-year period to examine any additional biopsy, imaging, and clinical follow-up information to categorize the original biopsy as truly benign, malignant, or equivocal. Standard deviations and 95% confidence intervals were calculated.
Results
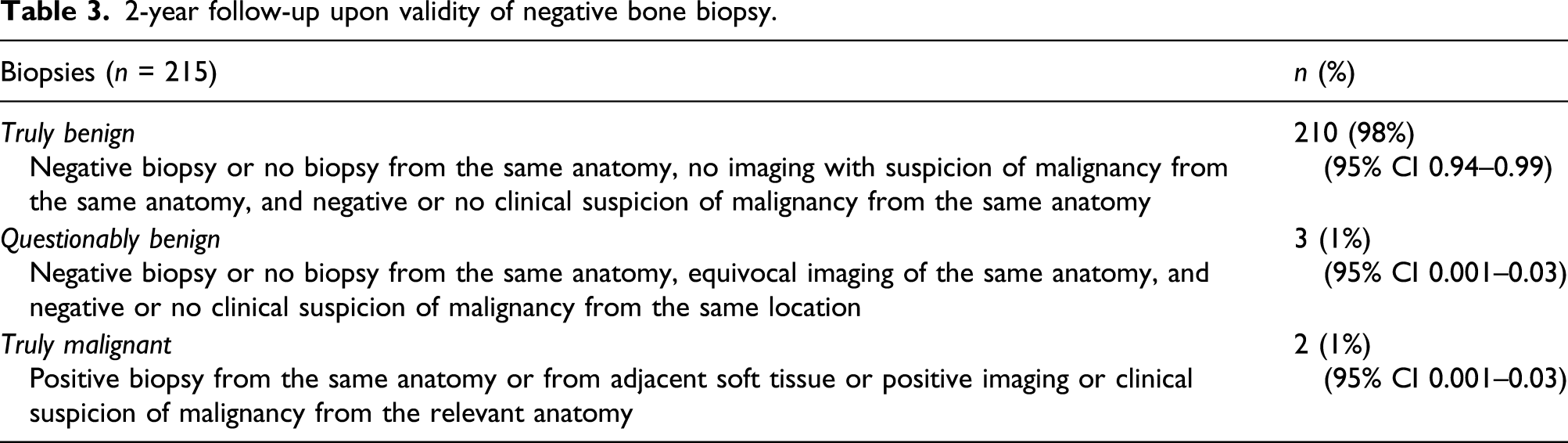
210 of 215 biopsies (98%; 95% CI 0.94–0.99) showed to be truly benign 2 years after initial biopsy. Two biopsies were false negatives (1%; 95% CI 0.001–0.03), and three were equivocal (lack of imaging description).
Conclusion
Our study documents negative bone biopsy as a valid criterion for the absence of bone metastasis. Since only 28% had a confirmed diagnosis of prior cancer and not all patients received adequately sensitive imaging, our results might not be applicable to all cancer patients with suspicious bone lesions.
Introduction
Metastases account for the majority of malignant bone lesions. 1 Of the metastatic lesions, 85% originate from the breast, lung, prostate, kidney, and thyroid, and in 25–30% of cases, they are the first manifestation of malignancy. 2 Approximately 70% of breast and 90% of prostate cancer patients eventually develop skeletal metastases, which represents the third most frequent metastatic site behind the lung and liver, the most frequent metastatic site among men, and the second most frequent metastatic site among women.3–8
Early diagnosis and treatment of skeletal metastases are crucial because the impact on patient morbidity, including bone pain, fractures, hypercalcemia, and spinal cord compression, is significant and associated with considerable use of healthcare resources.3,9–13 Only 20% of breast cancer patients remain alive 5 years after the discovery of bone metastasis. 13
A prompt multimodal management approach depends on early diagnosis, which is most often based on a combination of imaging, clinical information, blood samples, and, to a lesser extent, bone biopsies. 14 Up to 30% of patients have skeletal metastases from an unknown primary neoplasm despite a thorough history, physical examination, appropriate laboratory testing, and advanced imaging technology. 2 In such situations, only extensive histopathological investigations of bone specimens from biopsies can reveal the primary malignancy, and bone biopsies are generally considered the gold standard, that is, error-free reference standard, for verification of the presence or absence of skeletal malignancy.2,3,9,13,15 Nevertheless, bone biopsies are rarely performed, even in diagnostic test accuracy trials, and an insufficient reference standard has been identified as a major error source in biomedical research.15–21
When a bone biopsy documents presence of malignant cells, it is considered the gold standard for verification of cancer. 15 However, a negative biopsy can be a false negative, as observed with unrepresentative tissue sampling, especially in cases of benign bone lesions.22–26 Such diagnostic errors can have serious consequences and can also supply misleading results in diagnostic accuracy studies. 27 To the best of our knowledge, the validity of a negative or benign bone biopsy for exclusion of skeletal metastases remains to be documented.
The aim of our study was to investigate whether targeted bone biopsies described as non-malignant or benign identified in a population with a suspicious focal bone lesion are in fact truly benign after 2 years of follow-up.
Material and methods
Subjects
A computer search of pathology samples (hereafter named biopsies) representing consecutive bone material registered by SNOMED (Systematized Nomenclature of Medicine) T10* and T11* codes for skeletal cytology and histology biopsies from January 1, 2011, to July 31, 2013, was performed, providing a retrospective cohort of 409 consecutive targeted bone biopsies from 395 patients, who had undergone imaging (X-ray, CT, MRI, bone scintigraphy, or PET/CT) within 6 months of the biopsy. From these data, we extracted all skeletal biopsies categorized as benign or non-malignant, resulting in a total of 215 biopsies from 207 patients (43% women, 57% men, median age 64, and range 94).
Definitions and data collection
Based on the unique Danish Central Personal Registration system, which supplies each inhabitant with a personal ID number, in combination with databases that include diagnostic codes for each ID number, it is possible for researchers to follow patient groups with selected diagnoses for a longer period.
A 2-year follow-up for each of the 207 patients representing 215 non-malignant bone biopsies was conducted by two independent readers who reached consensus. The follow-up included a careful computer search on each patient identified by the unique Danish social security number in the pathology database for any additional biopsy, in the imaging system (EasyViz, Karos Health Inc., Waterloo, ON, Canada) for any imaging of the relevant structure, and finally, in the Electronical Patient Journal charts (EPJ - Clinical Suite, CSC Scandihealth A/S) for any relevant journal notes in order to categorize the original biopsy as truly benign, malignant, or equivocal.
The criteria for a biopsy defined as truly benign after 2 years of follow-up were (1) negative biopsy from the same anatomy or no biopsy from the same anatomy, (2) no imaging with suspicion of malignancy from the same anatomy, and (3) no clinical suspicion of malignancy from the same anatomy. A biopsy was considered malignant if one of the following criteria applied: (1) positive biopsy from the same structure or from adjacent soft tissue, (2) any positive imaging of the structure, or (3) clinical suspicion of malignancy from the relevant anatomy, for example, persistent symptoms or blood tests leading to additional diagnostic tests. Biopsies not classified as true benign or true malignant based on follow-up were categorized as equivocal. This category also included patients with post-biopsy imaging that was indeterminate for malignancy.
Statistical tests
Descriptive statistics included calculation of standard deviations and 95% confidence intervals (95% CI).
Approval
This retrospective observational study did not require ethical approval or informed consent in accordance with national legislation. The Danish Data Protection Agency approved the study and gave permission to access medical files for the purpose of the study.
Results
Characteristics of bone biopsies at the time of inclusion in the study
Types of prior history of cancer.

Surgical interventions accounted for 163 of 215 (76%) biopsies. The majority of these interventions (75/163, 46%) represented surgical resection from the anatomy in question, whereas samples acquired during alloplastic surgery, osteosynthesis, and spondylodesis accounted for 35, 24, and 21 biopsies (21, 15, and 13%), respectively. Fluoroscopy-assisted biopsy accounted for 40% of the nonsurgical biopsies and only 10% of the total biopsies, whereas CT-guided biopsies only accounted for 4% of the total biopsies. The remaining data represented vertebroplasty, arthroscopically acquired material and autopsies.
Among the 215 biopsies, the indication was suspected malignancy for 84 (39%), no indication was given for 5 lesions (2%), and a possible benign lesion was specified as an indication for 126 (59%) of the lesions. Removal of benign lesions such as cysts, enchondromas, non-ossifying fibromas, osteochondromas, and osteoid osteomas can be indicated in cases of discomfort, imminent fracture risk, or cosmetic problems, and in connection with removal, samples can be sent for pathological evaluation as well as samples taken in cases of slight uncertainty.
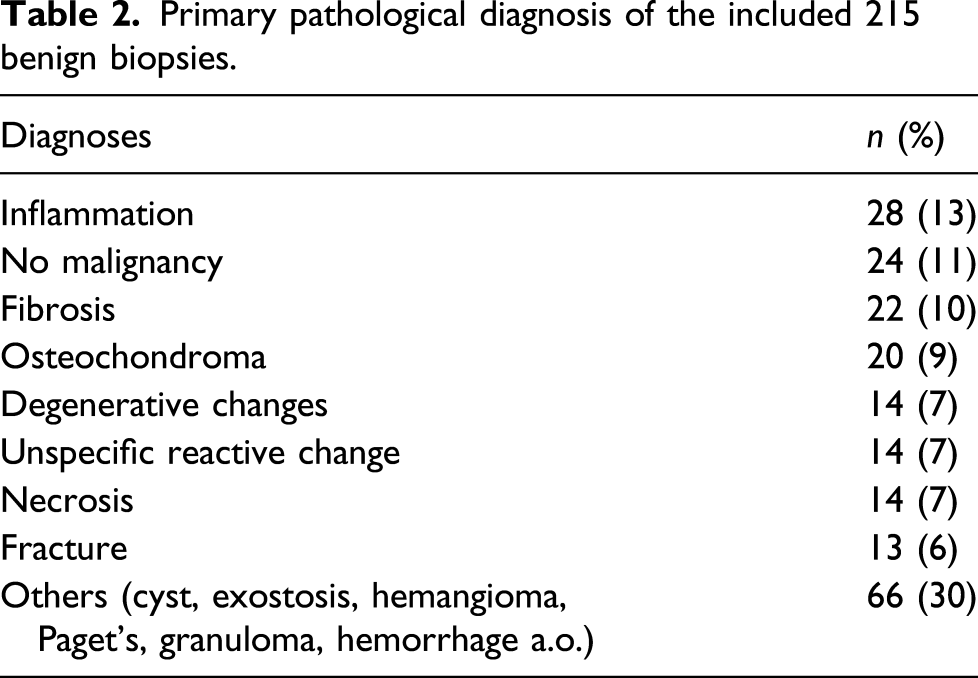
Primary pathological diagnosis of the included 215 benign biopsies.
True and false negative findings
2-year follow-up upon validity of negative bone biopsy.
Follow-up
Pathology
Pathological samples during the 2-year follow-up.
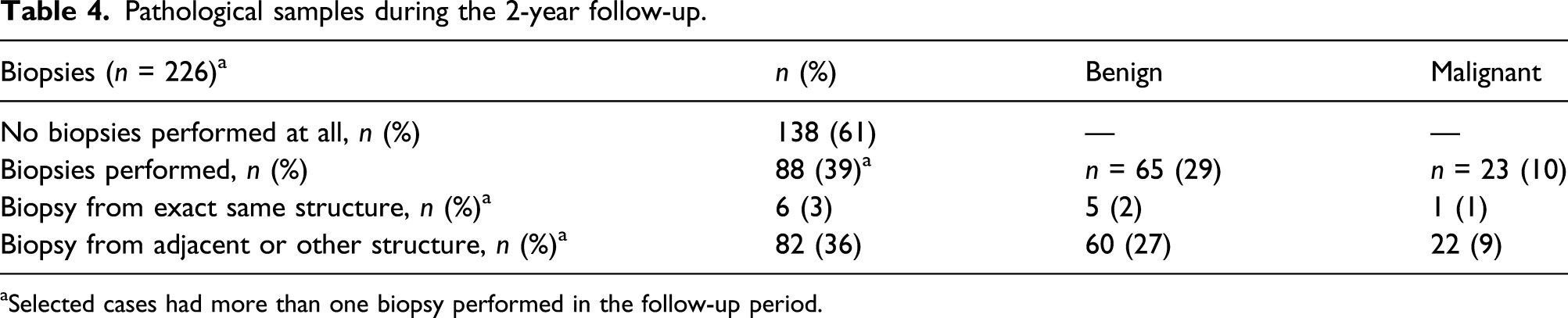
aSelected cases had more than one biopsy performed in the follow-up period.
In the first case, the primary biopsy was performed in March 2011 in connection with a percutaneous spinal decompression of L4 and was described as benign. A second biopsy was performed in April of the same year under general anesthesia, and this time, the biopsy was described as malignant (multiple myeloma). Imaging and notes in the journal persistently described the focal change in L4 as suspicious for malignant process. The patient died 3 years later in 2014. In the second case, the primary biopsy was acquired via CT-guided imaging in March 2013 from the ala of the right iliac bone and was described as benign, but doubt based on imaging was raised with respect to the representativeness of the tissue. A second CT-guided biopsy was performed in September 2013 and was once again described as benign, but doubt based on imaging and symptoms was persistently raised with respect to the representativeness of the sample. A third CT-guided biopsy including adjacent soft tissue was performed in May 2014, and this soft tissue sample demonstrated malignant cells from urinary bladder cancer. The patient died within the 2-year follow-up period.
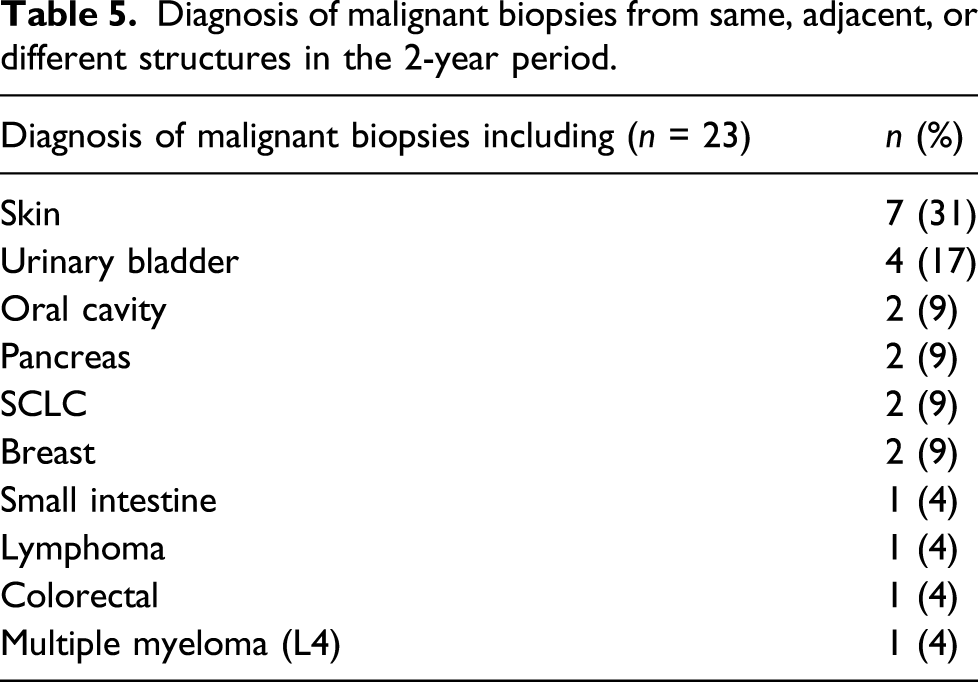
Diagnosis of malignant biopsies from same, adjacent, or different structures in the 2-year period.
Imaging
Imaging at the 2-year follow-up.
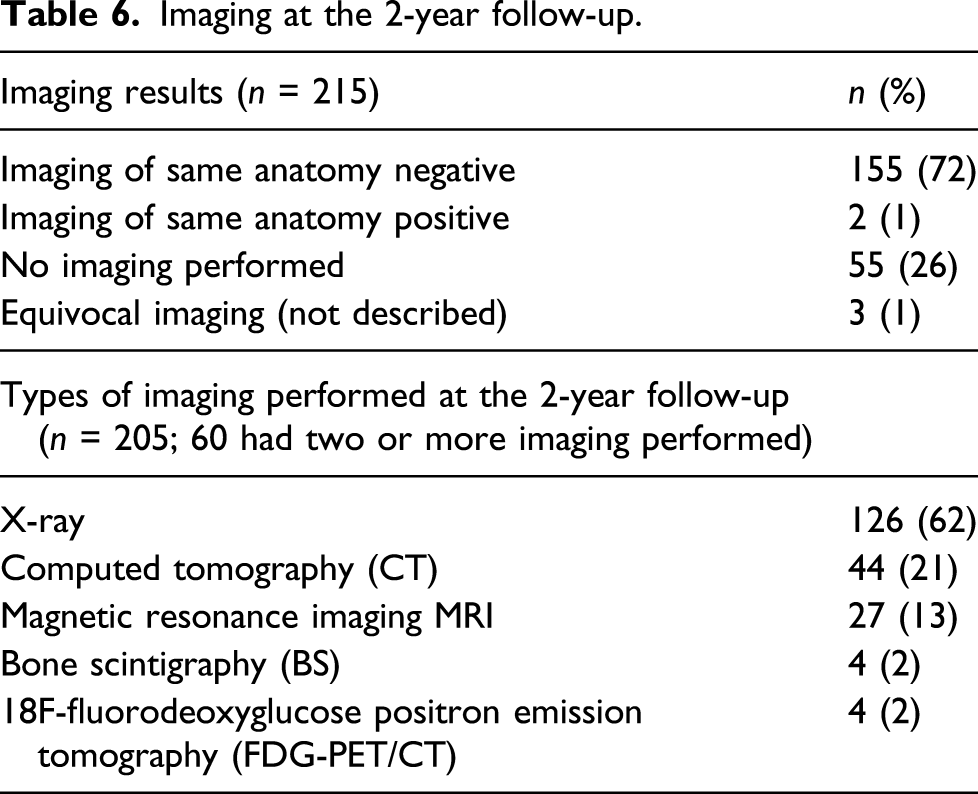
Out of the 59 biopsies taken from 57 patients with prior cancer diagnosis, 9 (15%) did not have any imaging performed in the follow-up period at all. Twenty-one had only one imaging performed, out of which X-ray represented 9 (15%). Twenty-two received 2 different imaging modalities and 7 received 3, meaning that 70% received at least one sensitive diagnostic imaging modality.
Clinical
According to clinical follow-up, 189 biopsies (88%) were not suspected to harbor a malignant condition in the same anatomy as the initial bone biopsy. In 24 (11%) biopsies, no journal notes were recorded in the period data. In the two lesions for which additional imaging and biopsies were described as malignant, the journal notes initially described the lesions as suspicious for malignancy. Later notes described the diagnosis of malignancy as confirmed by imaging and pathology.
Discussion
Based on a 2-year follow-up examination of available additional biopsies, imaging, and clinical information on 215 consecutive negative bone biopsies from 207 patients, we documented that 98% (210 biopsies) were indeed true negative after 2 years, proving a high validity of negative bone biopsies as an expression of the absence of skeletal metastases. Three cases were questionably benign due to equivocal imaging (no description), and only two were actual false negatives. We believe that we have proven a negative biopsy to be a valid marker of exclusion of the presence of skeletal metastases, which has not been previously documented, to the best of our knowledge.
The most frequent pathological inclusion diagnoses in our study were inflammation, no malignancy, fibrosis, osteochondroma, and degenerative changes, in accordance with other findings indicating that our material is representative. 28 Forty-six percent of the biopsies in our study were taken from extremities, whereas only 29% came from the spine, which is to be expected based on the knowledge that the spine, pelvis, ribs, and ends of long bones are preferred destinations of metastases because of their high red marrow content, whereas extremities are more often the seat of benign lesions.5,29,30
In many instances, benign bone tumors and tumor-like lesions of the bone can be diagnosed solely through conventional X-rays and require no biopsies for clarification. In our study, a benign lesion was specified as an indication for biopsy in 59% of cases, the majority of which were performed as a routine component of surgery. This result is in accordance with the findings of Scheitza et al., who demonstrated that only 21% of their biopsies were performed for actual confirmation of a benign diagnosis. In all other cases, biopsies were performed as a routine component of surgery, which can be indicated in cases of discomfort, imminent fracture risk, or cosmetic problems, and in connection with such surgery, samples can be sent for pathological evaluation. 31
Surgical biopsies accounted for 76% of our biopsy material, whereas CT-guided biopsies and fluoroscopy-assisted biopsy accounted for 4 and 10%, respectively. Open biopsy has been the conventional “gold standard” procedure for obtaining adequate and representative samples of tissue for diagnosis of musculoskeletal lesions, with a reported accuracy rate of 98%. 24 Recent results demonstrate that in carefully controlled situations in which the musculoskeletal radiologist works in a team approach with the orthopedic oncologist and orthopedic pathologist, the results from percutaneous biopsy can be highly effective and accurate. Additionally, most tumor treatment centers advocate for core biopsy performed under CT guidance, with a measured diagnostic yield ranging between 70 and 89%, a reported accuracy between 61 and 98%, and fewer biopsy complications than open surgical biopsy, even in sclerotic bone lesions.32–34 Other studies claim that the disadvantage of the CT-guided biopsy method is that metabolically active lesions without distinctive morphologies might not be reliably assessable by CT-guided biopsy and the false negative biopsy rate of such lesions might be substantially higher, with one series documenting that 18% required open biopsy after needle biopsy.22,32 The high percentage of surgical biopsies in our study might have contributed to the quality of samples and therefore to the low incidence of false negative results.
Spinal biopsies accounted for 29% of our material, and non-spinal biopsies accounted for 71%. Hau et al. demonstrated that the anatomical site has a significant effect on the accuracy of CT-guided biopsy, with non-spinal sites exhibiting greater accuracy (75%) than spinal sites (61%). Hau also showed that lesion size, type of margin, and gender did not influence the success or failure rates of the biopsies. 22 Because we only encountered two false negative and three equivocal lesions, our data set is too small to support those findings, but the high number of non-spinal lesions might have contributed to our high bioptic diagnostic accuracy even though only 4% of our material was obtained in CT-guided biopsies.
Two biopsies (1%) showed to be false negatives in repeated biopsies performed due to imaging (CT and MRI) that persistently described the lesions as positive. Monfardini et al. showed that 8 out of 10 false negatives, CT-guided biopsies had positive PET scans, and 6 out of 10 had positive MR scans, leading to the conclusion that a negative biopsy result in cases of suspicious PET and/or MR findings should be carefully evaluated and considered for a second sampling. 24
A meta-analysis made by Cheng and Alavi concludes that 18F-FDG PET significantly outperforms iliac bone marrow biopsy in the detection of bone marrow infiltration in the initial staging of patients with Hodgkin’s lymphoma and therefore should be used as a first-line study. 35 It has been recognized that bone marrow biopsy is associated with a high false-negative rate in early cases of Hodgkin’s lymphoma 36 probably because the biopsy is taken from a standard anatomy without any prior suspicion of a focal lesion as opposed to the lesions identified in our study. Furthermore, the meta-analysis defines the tests under investigation as their own reference standard, as do the studies included, which might explain the significant interstudy heterogeneity in the sensitivity data of PET or iliac bone biopsy. This study underlines our statement of the importance of an error-free reference standard.
The bone matrix response to metastatic deposits is known to depend on the primary cancer type. 3 Osteolytic matrix response, characterized by destruction of normal bone, is present in multiple myeloma, renal cell carcinoma, malignant melanoma, non-small cell lung cancer, non-Hodgkin’s lymphoma, thyroid cancer, and the great majority of breast cancers. Osteoblastic metastases, characterized by deposition of new bone matrix, are present in Hodgkin’s lymphoma, prostate cancer and small cell lung cancer and mixed metastases, where the patient has both osteolytic and osteoblastic lesions, is present in gastrointestinal cancers and 15–20% of breast cancers. 3 In our cohort, 59 biopsies were taken from patients with prior cancers, out of which approximately 50% would cause mainly osteolytic, 25% mainly osteoblastic, and 25% mixed metastatic bone response in case of bone metastases. Seventy percent received at least one diagnostic imaging modality sensitive for all three types. 20
Our study has two main important implications. Primarily, we consider our findings important for future diagnostic, prognostic, and treatment purposes because false negative samples can lead to delayed diagnosis and consequently increased morbidity and mortality; bone biopsy from a suspicious lesion in patients with a known primary cancer has shown benign pathology in 21%.3,9,10,24,28 Our result also has important implications for the validity of scientific studies of treatment efficacy and diagnostic accuracy using biopsy as reference, as underlined by STARD (The Standards for Reporting of Diagnostic Accuracy), which considers biopsy as the gold standard for demonstration or exclusion of bone metastases. 21 Our study documents that a negative sample can be considered truly negative and proves biopsy as a valid gold standard for the absence of metastases.
Our study also contains limitations. The first limitation is the retrospective nature of the data, including selection of patients and the lack of uniform and systematized follow-up including standardized re-biopsy from the same anatomy. Second, the pathologists did not perform a blind evaluation of the specimen and were aware of the patient’s history, as in a normal clinical setting, which is known to have a possible effect on the final diagnosis. 24 Since only 28% had a confirmed diagnosis of prior cancer, our results might not be applicable to all cancer patients with suspicious bone lesions. Finally, the most frequently performed imaging modality in the follow-up period was X-ray (62%). A rather low X-ray sensitivity (33%) for diagnosis of skeletal malignancies has been demonstrated, and thus, this type of examination might have missed possible positive lesions and a subsequent repeated biopsy. 20 However, all samples were described as negative and 88% of the clinical follow-up did not raise any suspicion of malignancy, and thus, this impact might be limited.
In conclusion, we believe that our results show that it is reasonable to assess a negative bone biopsy as an indication of the absence of bone metastasis in the structure in question. These results offer value not only to diagnosis, morbidity, and mortality of metastatic bone disease but also to the accuracy of future treatment and diagnostic scientific studies. Prior cancer type, biopsy method, and site of the lesion should be taken into consideration, and possible repeated biopsy should be considered in cases of imaging that persistently describes the lesion as positive.
Footnotes
Acknowledgments
The authors acknowledge Michael Gade, Department of Nuclear Medicine, Clinical Cancer Research Center, Aalborg University Hospital, Aalborg, Denmark, for providing data collection assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.