
Abstract
We describe a case of nontuberculous mycobacteria infection in the thyroid gland in a 54-year-old woman who had painful thyroid enlargement. Ultrasonography showed ill-defined hypoechoic lesions without increased vascularity in both upper lobes of the thyroid gland. Fine needle aspiration biopsy was performed, and pathology showed granulomatous inflammation with necrotic debris that the pathologist suspected was subacute granulomatous thyroiditis or tuberculosis of the thyroid gland. Nontuberculous mycobacteria infection was confirmed after right hemithyroidectomy. Antimycobacterial therapy was initiated as the treatment of choice. Nontuberculous mycobacteria in the thyroid gland appear to be rare. In clinical practice, however, it should be considered as a differential diagnosis of a painful thyroid mass. For accurate diagnosis, clinical and radiological features plus histological examination are required.
Keywords
Introduction
Nontuberculous mycobacteria (NTM) are a group of ubiquitous, low-grade pathogens that typically infect the cervical lymph nodes, skin, soft tissues, and lungs. 1 The symptoms and the severity of infection depend on the presence of underlying disease and the infected patient’s immunity. 2 NTM-related infection of the thyroid gland is very rare, and its disease entity has not been well described to date. 3 Computed tomography (CT) and sonographic findings of NTM infection of the thyroid gland are rare; therefore, only a few reports to date have been documented. We report here the radiologic findings of a 54-year-old woman with NTM infection involving the thyroid gland.
Case presentation
A 54-year-old woman visited our hospital with a palpable mass accompanied by pain in her right thyroid gland. She had found a lump several months previously. She had no underlying disease, and no significant findings were found on her complete blood count, blood chemistry, or electrolyte profile. The patient underwent ultrasonography to evaluate the thyroid mass. The patient complained of extreme pain when compressing the right thyroid gland with an ultrasound probe. Ultrasonography revealed ill-defined hypoechoic lesions without increased vascularity in both upper lobes of the thyroid gland (Fig. 1). No sonographic abnormalities were observed in the bilateral cervical lymph nodes. The patient had caught a cold a month previously, and we suspected subacute thyroiditis in consideration of sonographic features. Fine needle aspiration biopsy (FNAB) was performed at the upper pole of the right thyroid gland. Pathology showed granulomatous inflammation with necrotic debris that the pathologist suspected was subacute granulomatous thyroiditis or tuberculosis of the thyroid gland. The patient underwent surgical removal of the right thyroid lobe for a final diagnosis. For further evaluation, chest plain radiography, CT, and NTM-polymerase chain reaction (NTM-PCR) were performed. Chest plain radiography showed no abnormal findings in both lungs. CT image showed enlargement and heterogeneous attenuation in both lobes of the thyroid gland, especially in the right lobe (Fig. 2). NTM-PCR showed positivity, and the final pathologic report described chronic granulomatous inflammation, consistent with NTM infection of the thyroid gland (Fig. 3). The patient was initially treated with antimycobacterial medication.

(a) A 54-year-old woman with a palpable mass and pain in the right side of her neck. Ultrasound shows ill-defined hypoechoic lesions in the anterior aspect of the right lobe of the thyroid (white arrows). (b) Color Doppler sonogram shows only minimal vascularity at the periphery of the hypoechoic lesion.
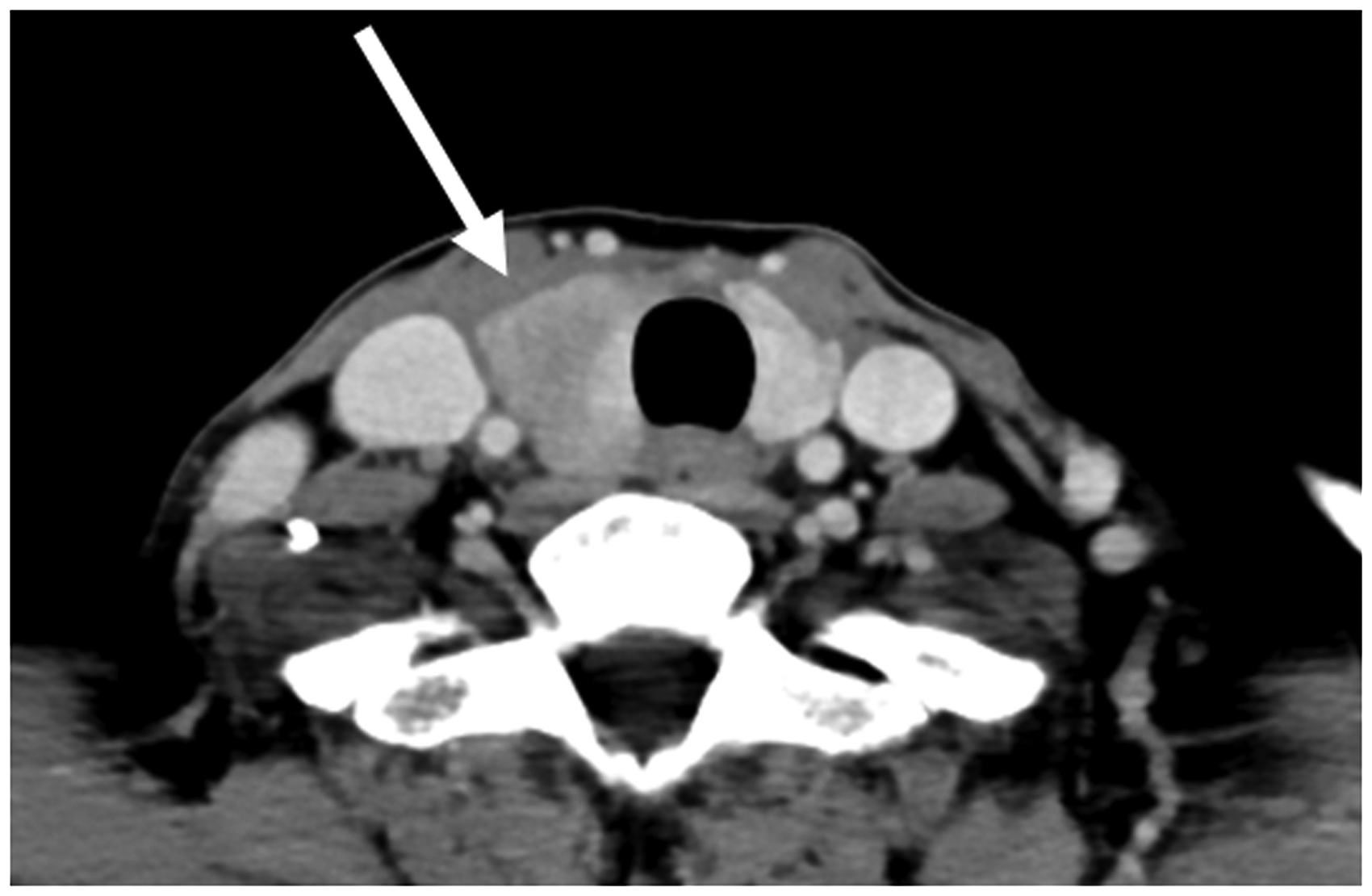
Head and neck computed tomography image shows heterogeneous attenuation in both lobes of the thyroid gland and enlargement in the right lobe (white arrow).

The non-caseating granulomatous inflammation is involving the entire thyroid parenchyma. (a) The thyroid follicles are destroyed and distorted by inflammatory cells (HE, ×100). (b) A multinucleated giant cells (black arrow) is noted within granuloma (HE, ×200).
Discussion
Generally, NTM disease most commonly involves the lung but can also involve skin, soft tissue, and cervical lymph nodes. NTM infection of the thyroid gland is a very rare occurrence that only one other case has been found in the literature. In a previous case report, a four-year-old girl had a firm neck mass with stiffness for a month. 3 A thyroid scan showed poor uptake of radioactivity in the entire right lobe of the enlarged gland and adequate uptake in the left upper pole with increased uptake in the left lower pole. A needle biopsy of the left lower pole demonstrated acute and chronic inflammation with giant cells. The Gram stain showed no bacteria, and special stains did not prove acid-fast organisms or fungi. Mycobacterium chelonae, one type of NTM, grew in the cultures of this tissue. She was initially treated with kanamycin and ethionamide but eventually underwent subtotal thyroidectomy. The postoperative course was marked by transient hypoparathyroidism. Two years after her surgery, her serum thyroxine, calcium, and phosphorus levels normalized. 3 In contrast to this case report, the radiologic presentation of our case was helpful for a differential diagnosis of NTM thyroiditis. The sonographic finding suggested ill-defined hypoechoic lesions in the anterior aspect of both lobes of the thyroid gland. Contrast-enhanced CT showed an enlarged right lobe of the thyroid gland with heterogeneous attenuation. Long-term antimycobacterial medication was the treatment of choice. 4 An example of the four-year-old girl was in 1975, and since then, the method of radiologic examination, including the development of ultrasound technology, has improved significantly.
Painful thyroiditis generally includes subacute, inflammatory, or infectious, traumatic, and radiation thyroiditis. Subacute granulomatous thyroiditis is the most common cause of a painful thyroid gland thought to be caused by viral infection of the thyroid gland. The most commonly implicated viruses include enterovirus, coxsackievirus, mumps, measles, rubella, influenza, parvovirus B19, adenovirus, and many others.5,6 Although subacute thyroiditis is often associated with a viral infection, sometimes no infective agent has been identified. Subacute thyroiditis is characterized by neck pain, tenderness, and/or symptoms of thyrotoxicosis. The classic pattern revealed by a thyroid function test is hyperthyroidism, followed by hypothyroidism, and then recovery.7,8 Typical sonographic findings of subacute thyroiditis include focal or multifocal poorly defined hypoechoic areas in one or both thyroid lobes similar to our case. Infectious or inflammatory thyroiditis includes all forms of infections, which may be either acute or chronic. It is usually caused by bacterial infections such as Staphylococcus, Streptococcus, and Enterobacter. However, fungal, mycobacterial, or parasitic infections may be the cause. Patients complain of a tender mass or swelling over the thyroid gland and fever. A thyroid function test in a patient with acute infectious thyroiditis is usually normal, but thyrotoxicosis may be present.6,9 On sonography, the infected portion of the thyroid gland appears enlarged and shows heterogeneous echogenicity with a superimposed anechoic or hypoechoic mass, in the setting of abscess formation. 10 The abscess usually tends to demonstrate peripheral hypervascularity without interval vascularity. There was no definite difference in ultrasonographic findings among pathogens.
Tuberculosis of the thyroid gland is also an extremely rare disease. The frequency of thyroid tuberculosis has been reported as 0.1–0.6% in surgically resected specimens and thyroid lesions subjected to FNAB11,12 The clinical manifestation is often subacute, but it can be asymptomatic or acute in cases of abscess or thyroiditis. Thyroid function is usually in the normal range. Symptoms of thyrotoxicosis due to tuberculous thyroiditis generally occur at the beginning of glandular involvement. The differential diagnosis depends on the presence of localized pain. If pain exists, subacute thyroiditis cannot be excluded. Ultrasonography usually represents multifocal, a heterogeneous and hypoechoic mass with ill-defined margins. 13 An abscess is anechoic and may show internal echoes. Contrast-enhanced CT can assist in localizing the lesion. The diagnosis is made only by FNAB or after histopathological examination of the surgical specimen when the FNAB is negative. Treatment includes antituberculous drugs combined with surgical removal of the affected sites of the thyroid gland. 14
In our case, ultrasonography revealed ill-defined hypoechoic lesions in the anterior aspect of both thyroid lobes which were similar as subacute thyroiditis. Sonographic features of subacute thyroiditis were heterogeneous diffusely or focally marked hypoechoic areas with the characteristic features like “lava flow”, involving bilateral lobes. 15 The image of thyroid cancer is usually different from the typical image of diffused hypoechoic areas in subacute thyroiditis. Well-known sonographic findings of thyroid cancer include as follows: solidity, hypoechogenicity, taller-than-wide in shape, lobulated or irregular in margin, microcalcifications. However, some features of the ultrasound image of thyroid cancer may be similar to subacute thyroiditis, such as poorly defined margin, hypoechogenicity, and the absence of internal vascularity.16,17 Therefore, FNAB should be performed on all patients suspected of subacute thyroiditis, especially when the diagnosis is confusing.
In conclusion, NTM of the thyroid gland is an extremely rare disease that is difficult to diagnose. However, it should be considered as a differential diagnosis of a painful thyroid mass. For accurate diagnosis, histological examination is essential in addition to clinical and radiological features.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.