
Abstract
Mammography, as the primary screening modality, has facilitated a substantial decrease in breast cancer-related mortality in the general population. However, the sensitivity of mammography for breast cancer detection is decreased in women with higher breast densities, which is an independent risk factor for breast cancer. With increasing public awareness of the implications of a high breast density, there is an increasing demand for supplemental screening in these patients. Yet, improvements in breast cancer detection with supplemental screening methods come at the expense of increased false-positives, recall rates, patient anxiety, and costs. Therefore, breast cancer screening practice must change from a general one-size-fits-all approach to a more personalized, risk-based one that is tailored to the individual woman’s risk, personal beliefs, and preferences, while accounting for cost, potential harm, and benefits.
This overview will provide an overview of the available breast density assessment modalities, the current breast density screening recommendations for women at average risk of breast cancer, and supplemental methods for breast cancer screening. In addition, we will provide a look at the possibilities for a risk-adapted breast cancer screening.
Introduction
Breast cancer is the most common female cancer and the second leading cause of cancer death, with one in 37 women dying from the disease (1). According to the American Cancer Society, the incidence of breast cancer was estimated to be about 252,710 new cases of invasive breast cancer and 63,410 new cases of non-invasive (in situ) breast cancer in 2017 (1). Population-based screening programs using mammography have been implemented to detect breast cancer at an early stage and, consequently, have contributed to the reduction in mortality (2,3). Although there is agreement that full-field digital mammography (FFDM) is the current screening examination of choice, there is currently no broad consensus on the age at which to start screening or what screening intervals should be, with different recommendations being issued by different national breast cancer screening programs. In general, screening mammography has a good sensitivity and specificity of 81–87% and 98–92%, respectively, for breast cancer diagnosis in women aged 40–79 years, and a breast cancer detection rate of 4–5 breast cancers per 1000 examinations (4). However, it has been shown that screening performance is influenced by age at screening, as well as mammographic breast density. There is a strong body of evidence that screening mammography is less sensitive in women aged 40–49 years, and/ or with heterogeneous or extremely dense breast tissue, thus limiting the applicability and usefulness of screening in those groups (4). The decreased sensitivity is caused by the so-called “masking effect” of breast cancer, which is caused by an overlap with normal breast tissue and is most pronounced in extremely dense breast parenchyma (5–8). Although the “masking effect” is an important contributor to decreased screening performance, it should be noted that breast density has also been identified as a strong and independent risk factor for the subsequent development of breast cancer (9–13). The association between increased density and cancer risk opens new avenues for risk prediction and stratification, as well as the development of tailored breast-screening strategies. This overview will provide an overview of the available breast density assessment modalities, the current breast-density screening recommendations for women at average risk of breast cancer, and supplemental methods for a tailored breast cancer screening. In addition, we will provide a look at a risk-adapted breast cancer screening.
Breast density
Breast density, or the amount of fibroglandular tissue in the breast, is defined as the relationship of fat to epithelial and connective tissue by the total breast area. On mammography, fatty components appear radiolucent, whereas fibroglandular components, consisting of epithelial and stromal tissue, appear radiopaque. A wide variability of breast tissue composition exists among women, which is also subject to change during life and is influenced by hormonal fluctuations during the monthly cycle (14–17). According to the American College of Radiology (ACR), 50% of women in the United States belong to the high density group, with 40% being categorized as heterogeneously dense (ACR category C) and 10% as extremely dense (ACR category D) (6). Epidemiological studies have shown global disparity between different ethnic groups, with Caucasian and black women showing the highest incidence rates of breast cancer and an almost similar breast cancer occurrence (18). Asian women historically have had a lower incidence of the disease (19), but with increased adaptation to Western ways of living, the incidence has been rising constantly (20). In contrast to the lower breast cancer risk of the Asian population, studies have found an approximately 2–4% higher percentage grade of breast density compared to Caucasian women (21–23). Recent data from a comparative analysis showed that due to population differences in body height, weight, and parity, postmenopausal Asian women showed lower density volumes of 3.0 cm3 compared to postmenopausal Caucasian women (24). In addition to the age and hormonal changes during the menstrual cycle, breast density is also significantly influenced by body mass index (BMI) and number of childbirths. In a large twin study, Nguyen et al. showed that the number of childbirths was associated with a decreased mammographic breast density and corresponded to a breast cancer risk reduction of 4% per live birth (25). In another recently published study, childbirth status as well as elevated BMI showed a connection with lower breast density, regardless of age (26). The increase in weight and BMI through menopause due to fat storage in the breast and an associated decrease in breast density has also been observed by Wanders et al. (27). However, the decrease in breast density caused by weight gain seems to be contradictory to the observation of a higher breast cancer risk with a higher BMI in postmenopausal women (13,28). Hopper et al. demonstrated, in a longitudinal prospective study, a negative association between breast density at the ages of 47–50 years compared to BMI measured at the ages of 7–15 years and concluded that adolescent BMI is negatively associated with breast cancer risk (29), which is in line with other published data (30,31). In addition, lower BMI values or a moderate reduction of body weight resulted in postmenopausal breast cancer risk reduction up to 50% (32,33). Conclusive data have shown that an increased breast density is a strong independent imaging biomarker for increased breast cancer risk (10,12,34,35). After age and genetic factors, such as BRCA status, a linear increase in breast density, which means that women with a Breast Imaging Reporting and Data System (BI-RADS) category of D are associated with a four- to sixfold increase in the risk of breast cancer compared to women in the lowest density group, BI-RADS A (36). Health authorities have recognized the relevance and impact of breast density in screening and, in some countries, supplemental screening methods for women with dense breasts (ACR categories C and D) have been introduced (37–39). In this context, it also stands to reason that breast density may be used for individual risk assessment and tailored screening strategies (10,12,34,35).
Breast density assessment
Subjective qualitative assessment
The assessment of breast density is usually performed based on the mammographic appearance of the amount of fibroglandular tissue relative to fatty tissue on mammography. There is, at the moment, no recommendation or criteria for standardized breast density assessment (40,41). Various methods of breast density classification exist, ranging from the early classification systems of Wolfe (42) and Tabár (43) to the most commonly used BI-RADS classification of the ACR (6). The BI-RADS lexicon classifies breast density on mammography according to four categories, which are mainly assessed qualitatively by subjective visual estimation of the reporting radiologist. The current fifth edition of the BI-RADS atlas, which was updated in 2013, defines the four breast density categories as: ACR-A = the breasts are almost entirely fatty; ACR-B = there are scattered areas of fibroglandular density; ACR-C = the breasts are heterogeneously dense, which may obscure small masses; and ACR-D = the breasts are extremely dense, which lowers the sensitivity of mammography (6). Women classified as either ACR-A or -B are considered to have non-dense breasts, whereas women with ACR-C or -D are considered to have dense breasts. The fifth edition of the BI-RADS lexicon saw a change from a percentage categorization of total breast density to descriptive categories and identification of coalescent areas on the mammogram, acknowledging the possible masking of underlying breast masses (Fig. 1) and the potential benefit of supplemental screening (44). Several studies showed that this subjective visual estimation of breast density on mammography is prone to error, with great inter- and intra-observer variability (45–48). Although it has been demonstrated that training and experience can improve inter- and intra-observer variability (47,49,50), it is evident that subjective qualitative breast density assessment is not equipped to provide a reliable and reproducible objective assessment of breast density as a risk factor.
Image example of the four descriptive breast density categories for mammography defined by the fifth edition of the ACR BI-RADS atlas: ACR-A = the breasts are almost entirely fatty; ACR-B = there are scattered areas of fibroglandular density; ACR-C = the breasts are heterogeneously dense, which may obscure small masses; and ACR-D = the breasts are extremely dense, which lowers the sensitivity of mammography.
Objective automated quantitative assessment
To overcome this limitation, efforts have been made to develop automated quantitative technologies for breast density measurement. There are computer-aided semi-automated and fully automated measurement approaches that allow either a two-dimensional (2D) or three-dimensional (3D) assessment of breast tissue structures. Cumulus™, the so-called gold standard of mammographic assessment of breast density, which has been validated by epidemiological studies, allows the estimation of the percentage area of dense breast tissue from mammographic images (51)—with higher reproducibility—compared to BI-RADS visual assessment (36). The limitation of Cumulus™ is that breast density measurements are derived from 2D mammography and this method still requires some user interaction, which renders it prone to bias. Recently, other 3D mammography-based breast density measurement systems have become available. Highnam (52) and van Engeland (53) introduced fully automated approaches, Quantra (46,54,55) and Volpara (46,48,54,55), which allow mammography-based, volumetric, quantitative breast density measurements. However, although these approaches are fully automated, breast density calculations based on mammography may vary due to differences in tissue compression and breast positioning (56). What all these assessment methods have in common is a positively association between breast cancer risk and breast density (57,58). However, data from Kontos et al. (59) discussed how the differences in quantitative breast density measurements are influenced by processed or raw mammographic images, as well as specific features of image acquisition, physical properties, and vendors.
Breast cancer screening
Summary of recommendation guidelines for breast cancer screening in average-risk women.

Summary of recommendation guidelines for breast cancer screening in high-risk women.
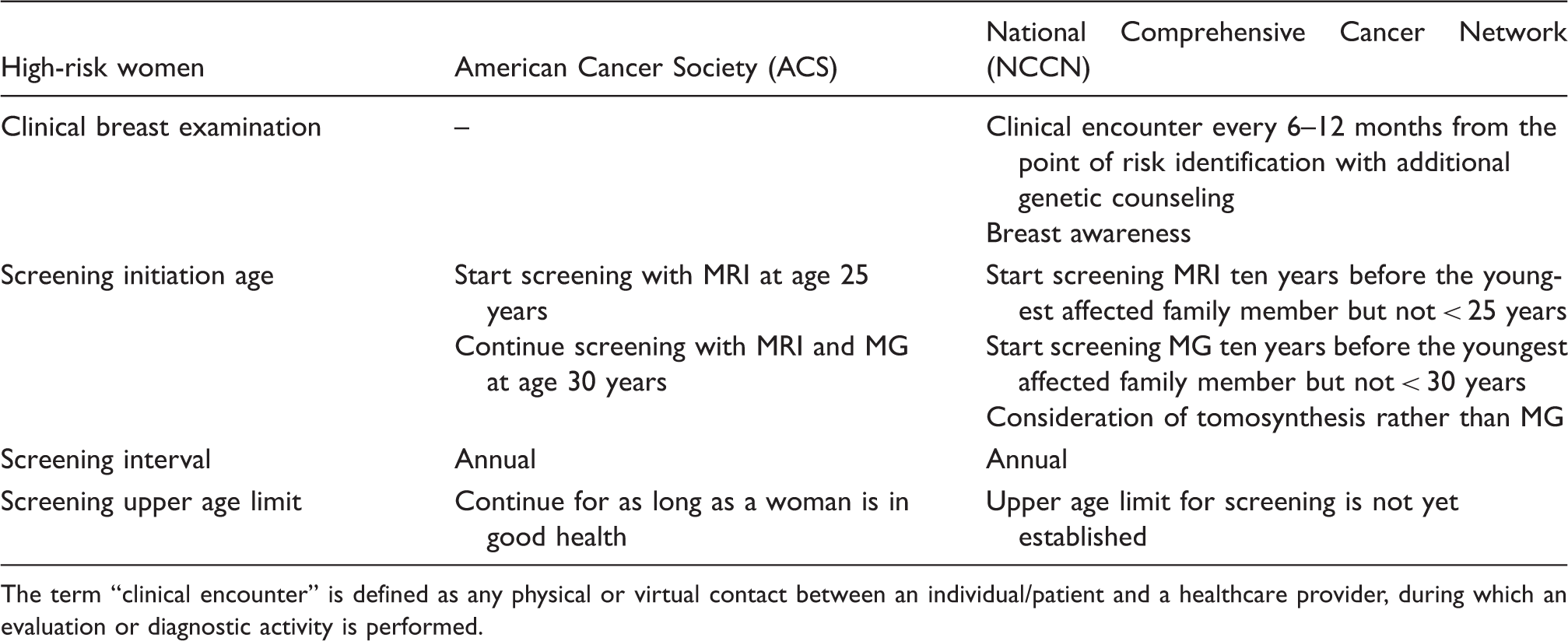
The term “clinical encounter” is defined as any physical or virtual contact between an individual/patient and a healthcare provider, during which an evaluation or diagnostic activity is performed.
Frequent over-diagnosis, false-positive results, increased costs, and patient anxiety are major points of criticism of any mammography screening program. Nelson et al. (66) performed a data analysis of screening FFDM in women aged 40–89 years and showed that the highest rate of false-positive diagnoses (121.2/1000) and recommendations for additional breast imaging (124.9/1000) were found in women aged 40–49 years. In a systematic review, they reported higher cumulative false-positive rates for mammography and biopsies with annual screening, compared to a two-year interval, for women aged 40–49 years, women with dense breasts, and for women under combined hormone substitution (67). Estimated over-diagnosis rates of up to 54% were reported in a series of 29 studies and were in the range of 11–22% in RCTs (67). Further, they found higher levels of anxiety, distress, and breast cancer-specific worry in women with false-positive diagnoses. In contrast, Pitman et al. (68) demonstrated a benefit of screening mammography for women aged 40–49 years, supporting the current ACS screening recommendations. Women with almost exclusively dense breasts in this age group had 18.8% of all screening-detected breast cancers and > 60% were invasive at the time of detection.
Another issue fueling the debate about the benefits of screening mammography is interval cancers. Interval cancers are defined as symptomatic or palpable breast cancers that present less than two years after a normal screening mammography (69). Interval cancers are often related to high breast densities, with a greater than 17-times risk compared to women with non-dense breasts (9,70,71). In a study by Webb et al. (69), the investigators showed greater interval cancer rates with significant breast cancer mortality, especially in younger women aged < 40 years (60%) or in the age range of 40–49 years (47%), who more often presented with dense breasts, but who had not participated in a screening program. However, for older women under screening, interval cancer rates do not exceed 28% (69). These findings highlight that a one-size-fits-all screening approach is not appropriate and that risk-adapted breast screening strategies that use supplemental screening, when indicated, are warranted.
Supplemental screening modalities
The aim of supplemental screening is to improve early breast cancer detection in women where traditional mammography screening has limitations. With increasing public awareness of the implications of increased breast density as a risk factor for breast cancer and its impact on the sensitivity of screening mammography, more women demand supplemental screening (72). However, there is great uncertainty and controversy about the potential beneficial effect of supplemental screening with regard to further reducing breast cancer mortality, since there is no evidence and it is unclear whether it is cost-effective. In the following sections, supplemental screening modalities that can may be offered to women, including digital breast tomosynthesis (DBT), breast ultrasound (US), and magnetic resonance imaging (MRI) of the breast, will be described and discussed.
Digital breast tomosynthesis
To overcome the inherent limitations of FFDM, with respect to coalescent parenchymal areas and superimpositions at higher density grades, DBT, or 3D mammography, has been implemented in breast imaging. Meanwhile, there are several prospective population-based trials available that have shown improved cancer detection and reduced recall rates when tomosynthesis is added to mammography. In the STORM-1 trial that evaluated the efficacy of tomosynthesis in combination with FFDM, Ciatto et al. showed an improved cancer detection rate from 5.3 to 8.1 cancers per 1000 screening examinations as well as a reduction in false-positive recalls by 17.2% (73). In addition, Bernardi et al. demonstrated similar results in the STORM-2 trial, with a cancer detection rate of up to 8.5 cancers per 1000 screens, when FFDM is combined with DBT, and up to 8.8 cancers per 1000 screens, when a synthesized 2D mammographic image is reconstructed and then combined with DBT. However, the results also showed an increase in the percentage of false-positive readings with 3.97%, 4.45%, and 2.42%, respectively (74). Other prospective population-based studies reported a significantly higher cancer detection rate with the possibility to detect more invasive cancers, when tomosynthesis was combined with FFDM (75). In this study, a detection rate for invasive and in situ cancers of 8.0 per 1000 screening examinations was reported when tomosynthesis was added to FFDM, compared to 6.1 per 1000 for mammography alone. Skaane et al. reported also a slight reduction in false-positives for the combined use, 53.1% vs. 61.1% (75). The Malmö Breast Tomosynthesis Screening Trial (MBTST), another prospective, population-based study revealed on the other side an increase of false-positive rates when breast cancer screening was carried out with tomosynthesis alone (1.7%), when tomosynthesis was combined with mammography (1.5%), and for mammography alone (1.1%), the latter of which was attributed to the appearance of stellate distortions (76). In addition, none of the studies investigated the cost-effectiveness of DBT as a supplemental screening modality to a great extent or evaluate the impact on a population-based screening program. However, with the improvements in the image-processing techniques of DBT and the possibility to synthesize 2D image projections from 3D acquisitions, DBT is likely to replace FFDM as a primary screening tool in the near future (77).
Breast ultrasound
US is a ubiquitous, available, cost-effective, and reliable imaging modality that does not use ionizing radiation. The reported cancer detection rate of US, in combination with FFDM, yields 3–4 additional cancers per 1000 screening examinations (78–80). However, the increased cancer detection rate of supplemental US screening comes at the expense of increased false-positive recall rates, costs, and patient anxiety (81). In a multicenter RCT that investigated screening with FFDM and US, Berg et al. (78) reported an increased cancer detection rate of 11.8 cancers per 1000 women, compared to FFDM alone (7.6 detected cancers per 1000 women) at the expense of a false-positive rate of up to 8.1% with US alone, and of up to 10.4% for combined FFDM and US. Other data by Berg et al. (80), using a RCT with a triennial observation of women with higher-density breast categories, yielded a cancer detection of 32 cases by US only, nearly as much as with FFDM only (33 cancers). Supplemental US after mammography yielded an additional cancer detection of 5.3 per 1000 women in the first year and 3.7 cancers per 1000 women in each of the next two years, with an average additional cancer detection rate of 4.3 per 1000 screened women (80). Similar results with respect to additional cancer yield—3.2 (79), 3.4 (82), and 7.1 (83)—and false-positive rates of 4.7% (79) and 3.3% (83) were reported by retro- and prospective studies. The Japan Strategic Anti-Cancer Randomized Trial (J-STAT) investigated the efficacy of additional US in a large nationwide screening program for breast cancer, with a significantly higher breast cancer detection rate, a lower number of interval cancers, and the detection of additional cancers, compared to mammography alone, in women aged 40–49 years (84). In addition, Austria started a nationwide biannual mammography screening program offering additional US for those with density categories C and D. Initial results are expected to be presented soon (39). To overcome the observer-dependency of hand-held supplemental screening US, automated, 3D, whole-breast US (ABUS) has been introduced (85–87). A recently published study by Wilczek et al., where ABUS was used in addition to mammography, yielded an increased cancer detection rate of 6.6 per 1000 screening exams in contrast to 4.2 cancers detected with mammography alone. Initial results suggest that ABUS can provide 3D volumetric imaging (86,87), and thus, may be a valid option in this setting to enable the detection of additional breast cancers that are invisible on mammography (88).
Breast magnetic resonance imaging
Another supplemental screening modality that can be offered is MRI. MRI is a radiation- and compression-free 3D imaging modality and, currently, is the most sensitive test for breast cancer detection (89–92). According to international guidelines, annual screening with dynamic contrast-enhanced MRI is recommended for women with an estimated lifetime risk of breast cancer of >20% (38,80,93,94). Per ACS screening, breast MRI may be recommended for women with heterogeneous or extremely dense tissue as a supplement to mammography (94). In a multicenter trial of women at high genetic risk for inherited breast cancer, the reported diagnostic performance of MRI showed an overall sensitivity of 91% and a specificity of 97%. Sensitivity increased up to 93% if MRI was a supplement to mammography or sonography (93). Data from Berg et al. (80), on an asymptomatic screening collective of women with at least one other risk factor in addition to heterogeneous or extremely dense breasts, showed a sensitivity of 100% if mammography was combined with US and MRI; however, the specificity in this study for the combined use of all three modalities was reportedly at least 65%. In a triple-modality screening study of high-risk women, Riedl et al. (38) showed the superiority of MRI over mammography and US for early breast cancer detection, with no influence of age, breast density, or breast cancer risk status. The reported MRI sensitivity and specificity were 90% and 89%, respectively. Sensitivity was further increased when MRI was combined with mammography or if all three modalities were used together (95%) (95). However, specificities and positive predictive values were lower in younger women and in higher density categories (38).
Currently, there are no data available on supplemental screening with MRI in women with higher breast density categories. The Dutch DENSE trial is investigating the effectiveness and cost-effectiveness of screening with mammography and MRI compared with those of screening with mammography alone in women with extremely dense breasts (95). The study has finished enrollment and results are eagerly anticipated to better define the role of MRI in this patient population. At this time, the value of supplemental breast MRI screening in women with higher breast density categories remains unclear and the ACS guidelines do not recommend for or against screening MRI in women with the risk factor of a higher breast density (94,96,97).
Although MRI of the breast is the most sensitive test for breast cancer detection, its application as a screening tool for women at an average risk of breast cancer is limited by costs, availability, as well as reading and examination time. However, the introduction of abbreviated imaging protocols, with scan times of approximately 3 min has sparked the discussion about whether to also offer MRI screening also to women at average risk for breast cancer (98,99). Although initial results for abbreviated MRI as a screening tool are promising, there is currently not enough data to recommend breast MRI screening for the average population.
New avenues for risk-adapted screening
In addition to breast density as an individual risk factor for breast cancer, there are several other risk factors that increase the risk, such as genetic predisposition, number of affected first-degree relatives, chest radiation therapy at a young age, ethnicity, lifestyle factors, and previous personal history of breast malignancies exist (18). To date, there are no recommendations for risk-adapted screening available. Implemented population-based screening programs aimed at detection breast cancer detection at an early stage using mammography, as a cornerstone technique, have resulted in an effective decrease in breast cancer mortality of up to 49% (2,3). Breast cancer risk estimation tools, such as the Gail and Tyrer-Cuzick models, have been introduced with the purpose of identifying women at risk of developing a future breast cancer (100–102). The Gail model from the National Cancer Institute, which is based on the general population, is an eight-question tool using age, hormonal factors, benign disease, and number of first-degree relatives who have already been diagnosed with breast cancer to estimate the relative risk of developing invasive breast cancer (103). In the Tyrer-Cuzick model, similar risk factors from the Gail approach are used in conjunction with personal and genetic factors, including the BRCA1/2 genes for risk assessment of invasive breast cancer (102). However, it has been demonstrated that mammographic density seems to be a stronger risk factor, and the combination of breast density with either the Gail or the Tyrer-Cuzick model resulted in a better breast cancer risk assessment (104). Moreover, the process of screening for breast cancer remains controversial, with a number of recommendations from various national Breast Cancer Screening Programs concerning the starting points and the intervals for screening. A potential model for risk-adapted screening could include an initial risk stratification that incorporates family and personal history, breast density assessed with mammography, and, potentially, also lifestyle risk factors, such as obesity (105) and alcohol (106). Thereafter, women would be classified into three categories—low risk, intermediate risk, and high risk—and would undergo screening tailored to their individual risk.
Based on risk stratification, patients would then be offered risk-adapted screening with different imaging modalities, as depicted in Fig. 2. Low-risk women could continue to be screened with FFDM, or, when available, DBT with synthesized mammography annually, bi-annually, or triennially based on their national recommendations. Intermediate-risk women could undergo additional supplemental screening with US. High-risk women, who constitute a minority of women, would be offered MRI and MG only when a benefit has been demonstrated (e.g. BRCA 2 carrier) (107).
Model for risk-adapted screening.
The use of mammography screening in female populations has helped to lower the rates of breast cancer-related mortality in the general population. However, the sensitivity of mammography for breast cancer detection is decreased in women aged 40–49 years and in women with higher breast densities. In addition, there is evidence that breast density is also a strong independent risk factor for breast cancer. With increasing public awareness of the implications of a high breast density, there is an increasing demand for supplemental screening in these women (72). Currently potential supplemental screening modalities include DBT, US, and MRI of the breast, among which MRI is the most sensitive method available. However, the improvements in breast cancer detection with supplemental screening methods come at the expense of increased false-positives, recall rates, patient anxiety, and costs. Therefore, the approach to breast cancer screening will soon change, while we need further evidence to demonstrate the show of cost-effectiveness of supplemental screening. Such screening strategies would be tailored to the individual woman’s risk, personal beliefs, and preferences, while accounting for cost, potential harm, and patient-relevant outcomes. New strategies are warranted, and it can be expected that breast density and its assessment will play a huge role in the development of these strategies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Austrian Nationalbank “Jubilaeumsfond” Project No. 16219 and the 2020 – Research and Innovation Framework Programme PHC-11-2015 No. 667211-2.