
Abstract
Background
Computed tomographic angiography (CTA) may require a non-contrast enhanced dataset for the diagnostic workup. By using dual-energy acquisition, it is possible to obtain a virtual non-contrast-enhanced (VNC) dataset, thereby possibly eliminating the non-contrast acquisition and reducing the radiation dose.
Purpose
To compare image quality of VNC images reconstructed from arterial phase dual-energy CTA to true non-contrast (TNC) images, and to assess whether VNC images were of sufficient quality to replace TNC images.
Material and methods
Thirty consecutive patients with suspected abdominal aortic aneurysm, aortic dissection, or subacute control after EVAR/TEVAR were examined with dual-energy CT (DECT). The examination protocol included a single-energy TNC, DECT arterial phase (80 kV/Sn140 kV), and single-energy in venous phase of the aorta. A VNC dataset was obtained from the DE acquisition from arterial phase scans. Mean attenuation and image noise were measured within regions of interest at three levels in the aorta in TNC and VNC images. Comparison of the TNC and VNC images for artefacts was made side-by-side. Subjective evaluation included overall image quality on a 4-grade scale, and quantitative analysis of algorithm-induced artefacts by two experienced readers.
Results
For all cases, the aortic attenuation was significantly higher at VNC than at TNC. Image noise measured quantitatively was also significantly higher at VNC than at TNC. Subjective image quality was lower for VNC (mean = 3.1 for VNC, 3.7 = for TNC) but there were no cases rated non-diagnostic.
Conclusion
VNC images based on arterial phase CTA have significantly higher mean attenuation and higher noise levels compared to TNC.
Introduction
Computed tomography angiography (CTA) is commonly used for imaging of acute and chronic aortic disease. Endovascular aneurysm repair (EVAR) may require life-long follow-up by CTA to diagnose complications such as endoleaks or stentgraft migrations. For EVAR follow-up, a triple phase examination protocol including non-contrast medium (unenhanced) phase and contrast medium (enhanced) early and delayed venous phase acquisitions is the mainstay for follow-up (1,2), inducing a substantial radiation dose to the patients, although there is no generally accepted consensus as to which imaging strategy would be most advantageous. One method to reduce radiation dose would be to use a two-phase (unenhanced and split-bolus mixed arterial and venous phase) protocol instead of a three-phase (unenhanced, arterial and venous phase) protocol. Javor et al. has used a single acquisition with split contrast bolus with timing acquisition in both venous and arterial phases when replacing TNC images with VNC images (3).
Dual-energy CT (DECT) utilizes the different attenuation properties between materials or tissues for different X-ray energies. The differences are more pronounced in materials with high atomic numbers, such as iodine and calcium, due to their strong photoelectric effect causing high attenuation at lower photon energies. Water and muscle have similar attenuation at different photon energies and can therefore function as reference materials (4,5). The DE technique has several applications for clinical imaging and can allow reduction of the iodine contrast medium dose, as well as the radiation dose (6,7).
Imaging of arteries may benefit greatly from DECT. Using contrast-phase acquisition with two different X-ray tube peak voltages, where the lower peak voltage enables greater conspicuity of vessel attenuation, contrast medium can be reduced significantly with preserved image quality (8,9). The differences in atomic number between calcium and iodine make them readily separable with use of DE techniques. Using post-processing algorithms, it is possible to identify and remove bone structures, and also identify and remove the iodine content, and thereby obtain a reconstructed image comparative to an unenhanced dataset, virtual non-contrast (VNC) images, without having to do true non-contrast (TNC) acquisitions (10,11).
It has not been well established if the VNC is of acceptable quality to replace the TNC in aortic CTA (12).
The purpose of this study was to assess whether VNC images reconstructed from arterial phase DECTA were of sufficient quality to replace TNC images to reduce the radiation dose to the patients.
Material and Methods
Patient population
Basic characteristics of the study patients.

Median values (2.5 and 97.5 percentiles) are given unless otherwise stated.
CT parameters and radiation dose
CT scanning parameters of true non-contrast (TNC) acquisition and virtual non-contrast (VNC) reconstructions.

The examination was performed in the supine position in cranio-caudal direction at breath-hold from the thoracic aperture to the groins. All scanning parameters regarding the non-unenhanced phase for TNC analyses and the early arterial enhanced phase for VNC analyses are listed in Table 2. Individual contrast media volume and injection rates were calculated based on contrast media dose per kg body weight (maximum dose weight = 80 kg) at a dose of 340 mg I/kg and median volume of 80 mL (range = 38–99 mL). The early arterial-phase scan was acquired after initiation of the intravenous injection of contrast media (Omnipaque 300 mg I/mL, GE Healthcare, Oslo, Norway) with a fixed injection time of 15 s followed by a 50-mL saline chaser at 4 mL/s. Bolus-tracking with a threshold of 120 HU at the level of the renal arteries was used.
For both acquisitions, effective dose (ED) was calculated from the dose-length product (DLP) registered by the CT scanner and multiplied by the mean of the ED/DLP conversion factor for chest/abdomen/pelvis (0.186 mSv/(mGy×cm)) based on the IRCP 103 tissue weighting factors (13). The effective dose of a biphasic unenhanced and enhanced protocol was compared with a single-phase protocol, i.e. the arterial phase only.
True and virtual non-contrast image reconstruction
TNC images were reconstructed with a slice thickness/increment of 5/5 mm. The VNC dataset was obtained by a patented algorithm based on the dataset from the two X-ray tubes with different X-ray energies. A specific dual-energy post-processing workstation with a patented algorithm (Syngo MMWP version VA 20; Siemens Healthcare, Forchheim, Germany) was used for image analysis, generating VNC images from the arterial-phase acquisition.
Quantitative image quality analysis
Comparison of attenuation and noise between TNC and VNC images was made by drawing circular regions of interest (ROI) within the aortic lumen at the levels of the hemidiaphragms, the renal arteries, and the aortic bifurcation on a PACS workstation (IDS7, Sectra Imtec AB, Linköping, Sweden). The ROIs were made as large as possible while avoiding calcifications, plaques, and stent material. Mean attenuation and image noise (one standard deviation) in Hounsfield Units (HU) were registered.
Subjective image quality analysis
Subjective evaluation was done in two steps. First, the TNC and VNC images were evaluated side-by-side for artifacts such as residual contrast medium, subtraction of calcifications, or stent structures. Four months later, the second evaluation was done, in which the subjective image quality was scored at a fixed window setting (level/width = 200/650 HU) in randomized order by two senior consultant interventional radiologists (JW with ten years of CTA experience and LL with nine years of CTA experience) blinded to patient information and examination protocol on a PACS workstation using the viewing and scoring software ViewDEX v2.0 (Viewer for Digital Evaluation of X-ray images) (14,15). Image quality was evaluated for overall image quality, signs of residual contrast medium, possible subtracted calcifications, and stent structures. A four-point scale was used for overall diagnostic quality (4 = excellent, 3 = good, 2 = moderate but sufficient for diagnosis, and 1 = non-diagnostic). The specific artefacts were scored as yes/no.
Statistical analysis
Statistical analysis was performed using statistical software SPSS software (version 24.0; SPSS Inc., Chicago, IL, USA). The Mann–Whitney U test was used to compare differences between the TNC and the VNC datasets regarding vascular attenuation, noise, and radiation dose. The Wilcoxon signed-rank test was used to compare subjective evaluation of image quality. A P value < 0.05 was considered significant. Inter-observer agreement regarding overall image quality was assessed using intra-class correlation coefficient (ICC).
Results
VNC images were compared to images from an actual unenhanced dataset (TNC) in 30 consecutive patients examined for suspected acute aortic disease or for elective EVAR follow-up. All examinations were successful without any adverse events. Although the 80-kVp dataset had a limited FOV of 33 cm, the entire aorta and the iliac arteries were within the FOV in all cases.
Radiation data
Radiation parameters of true non-contrast (TNC) acquisition and virtual non-contrast (VNC) reconstructions.

Median values (2.5 and 97.5 percentiles) are given unless otherwise stated.
CTDIvol, volume computed tomographic dose index; mGy, milligray; mSv, millisievert.
Quantitative image quality
Attenuation (HU) and image noise (1 SD, HU) of the aortic lumen of true non-contrast (TNC) acquisition and virtual non-contrast (VNC) reconstructions.
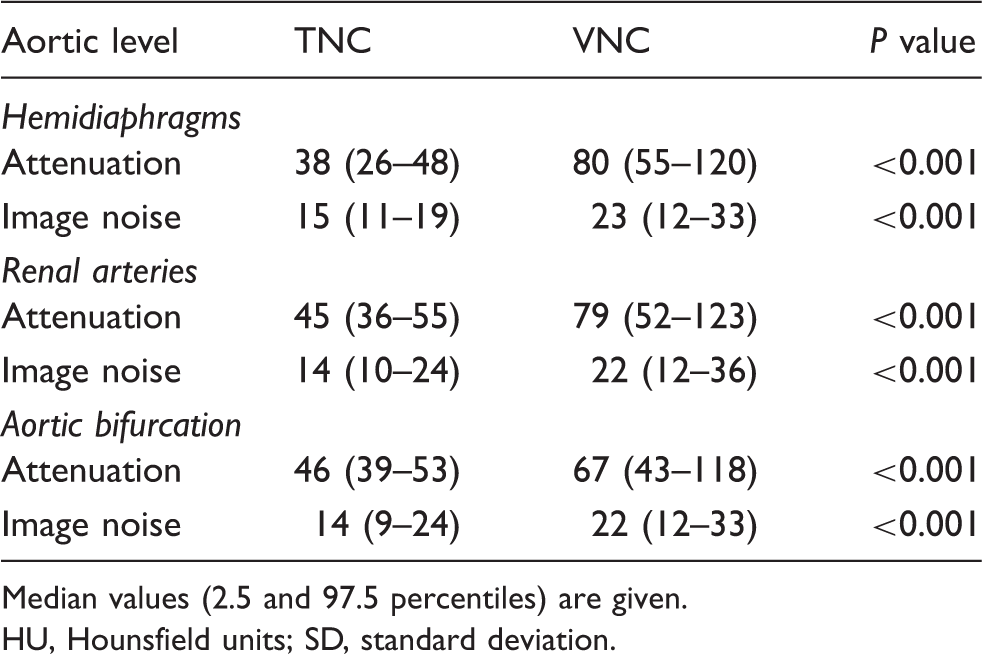
Median values (2.5 and 97.5 percentiles) are given.
HU, Hounsfield units; SD, standard deviation.
When comparing VNC images to the TNC images, side-by-side artifacts in major thoracic vessels were seen in VNC images (Fig. 1, Pulsation). Removal of minor arterial wall calcifications was seen in 22 out of 30 VNC images. In all cases, the removed calcifications were in the range of 1–3 mm and located at the aortic or iliac wall (Fig. 1, Calcification). Partially removed stent structures were seen in the VNC images in two cases. The removed stent structures were part of a renal stent and an aortic stent graft, respectively (Fig. 1, Stent). In five cases, incomplete elimination of the aortic contrast medium attenuation was seen in the VNC images (Fig. 1, Contrast medium) where three of the patients were women and two were men. These five patients had BMI of 26, 24, 33, 26, and 33 kg/m2. One of these patients was operated with fenestrated EVAR and four were referred to the study because of suspected aortic rupture. No obvious reason could be found during retrospective investigation.
Pulsation: Attenuation artifacts in main thoracic vessels in the VNC image. Calcification: Elimination of the small calcifications in the aortic wall in the TNC image. Elimination of the renal stent in the VNC image. Stent: A partly removed renal stent. Contrast medium: Incomplete elimination of the contrast media in the VNC image on the right in the abdominal aorta.
Subjective image quality
All TNC images were rated good or excellent (the mean image quality score was 3.6 for reader 1 and 3.7 for reader 2). All VNC images were rated moderate to excellent (the mean image quality score was 3.0 for reader 1 and 3.2 for reader 2). There was a significant (P < 0.001) difference in subjective image quality between TNC and VNC datasets. For the overall image quality, the inter-observer agreement was moderate with an average ICC value of 0.743.
Discussion
This prospective study based on 30 consecutive aortic DECT scans was carried out to compare the image quality of TNC to VNC images including attenuation and noise, as well as estimating the potential reduction in radiation dose. Throughout the study, we used a standardized DECT protocol to maintain image quality at a constant level.
Several authors have reported acceptable quality VNC images as acceptable replacements for the TNC images in the abdominal aorta (16,17) while in our study we found aortic attenuation was considerably higher in all VNC images compared to TNC images throughout the acquisitions. The difference was more pronounced in the proximal part of the aorta and less pronounced in the distal part of aorta and the iliac arteries. This attenuation difference between TNC and VNC was more pronounced in our material than has previously been reported (11,12,16). There are several possible explanations to this difference. We used tube voltages of 80/Sn140 kVp compared to 100/Sn140 kVp in previous studies (12,16). Compared to the study of Toepker et al. (16), in which a total of 110 mL Iomeron 400 mg I/mL contrast medium was used, we used only 80 mL Omnipaque 300 mg I/mL contrast medium.
In the thoracic aorta, close to the heart incomplete elimination of contrast media was seen, maybe caused by the pulsating movement of the aortic and pulmonary artery walls leading to a minimal spatial difference between tube A and tube B, thereby affecting the output of the VNC algorithm. This may be of clinical relevance if mistaken for a dissection or an intramural hematoma. Five moderate ratings were caused by such artefacts in the thoracic aorta. This could possibly be avoided by using electrocardiogram (ECG) gating. In 'two patients, a partial subtraction of stents occurred in the VNC images, resulting in diagnostic uncertainty, and rating as suboptimal image quality.
In 24 of 30 cases, some structures were removed by the VNC algorithm; in 22 cases, there were minor calcifications in the aortic wall. Subtraction of calcium from DECT data represents an in-built technical limitation of the VNC algorithm (18). This finding could represent an important limitation when the presence of calcification in aortic thrombus plays an important role in endoleak recognition. In two cases, minor parts of stents were partially subtracted which can be misinterpreted as a fracture or damage of the stent, the problem seen in some previous studies (19). One moderate rating was seen in a patient with a BMI of 35 kg/m2, resulting in grainy images and limited coverage of the abdominal circumference showing the 80-kVp ring all over the abdomen interfering with evaluation. Dose modulation by CareDose 4D was not fully compensated in patients with high BMI resulting in more image noise.
The present study is subjected to several limitations. The number of patients was relatively small and patient population was heterogeneous in terms of age and study indication.
In conclusion, VNC images based on arterial phase CTA have significantly higher attenuation values at the aorta and higher noise levels compared to TNC. According to our study, VNC images are not suitable as replacements for TNC images generally but can be considered when radiation dose reduction is definitely desirable or when no TNC acquisition is available.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.