
Abstract
Hepatocellular carcinoma (HCC) is the commonest primary tumor of the liver and carries a poor prognosis when diagnosed late or left untreated. Treatment relies heavily on the stage of the tumor when diagnosed. Extrahepatic metastasis is known to occur; these are mainly reported via autopsy studies or isolated case reports. Knowledge of extrahepatic metastasis is crucial in order to avoid unnecessary surgery. We report a rare case of a patient at our center, diagnosed to have HCC, who underwent treatment successfully, only to come back with extrahepatic metastasis to the skeletal muscles.
Introduction
Hepatocellular carcinoma (HCC) is diagnosed in half a million of the world’s population annually, including 20,000 new cases in the United States alone (1). Liver cancer is the fifth most common cancer in men and the seventh most common cancer in women. In developing countries, the highest rate of HCC is where Hepatitis B virus (HBV) infection is endemic – in the regions of South East Asia and sub-Saharan Africa. Katyal et al. described the incidence of extrahepatic metastasis in a retrospective review of 403 consecutive patients with HCC, imaged with computed tomography (CT). They found that the most common sites for extrahepatic metastasis included the lung, abdominal lymph nodes, and bone (2). Multiple skeletal muscle metastasis (without osseous involvement) with concomitant bilateral adrenal metastasis is an extremely rare occurrence. To our knowledge, this has not been reported before.
Case report
A 54-year-old man with underlying chronic HBV infection was diagnosed with HCC, for which he underwent a right hemi-hepatectomy the same year and was disease free until four years later. During the remission period, serial alpha feto-protein (AFP) levels and bi-annual abdominal sonography were normal. He presented to us with an abrupt onset of constitutional symptoms: poor appetite and weight loss of 6 kg within a month. There were additional complaints of abdominal distension and altered bowel habits. Upon thorough clinical examination, he was found to be cachexic. Multiple abdominal wall superficial masses were present. These masses were located at the left hypochondrium (10 × 8 cm), right lower abdomen (5 × 5 cm), and central lower abdomen (3 × 4 cm). These palpable masses were located away from the previous surgical scar. Although within normal range, there was slight elevation of the serum AFP level to 7.47 ng/mL from a baseline of 3–5 ng/mL previously (normal range = 0–8 ng/mL).
CT of the abdomen showed absence of lesions in the remaining left lobe of the liver. However, there were heterogeneous masses located at the adrenal glands, right psoas muscle, bilateral erector spinae, left gluteus maximus, and right gluteus intermedius muscle in addition to the superficially located masses, noted to be within the anterior abdominal wall muscles (Fig. 1). A core biopsy was taken at the left rectus abdominis muscle, with histopathological findings positive for hepatic marker (Hep Par 1); suggesting a metastatic lesion likely originating from the previously diagnosed HCC. A conservative approach was undertaken. He unfortunately deteriorated further and died six months later.
Contrasted axial CT images at various levels showing heterogeneously enhancing masses located at: (a) bilateral adrenal glands; (b) bilateral erector spinae muscles; (c) right psoas muscle; and (d) left rectus abdominis muscle.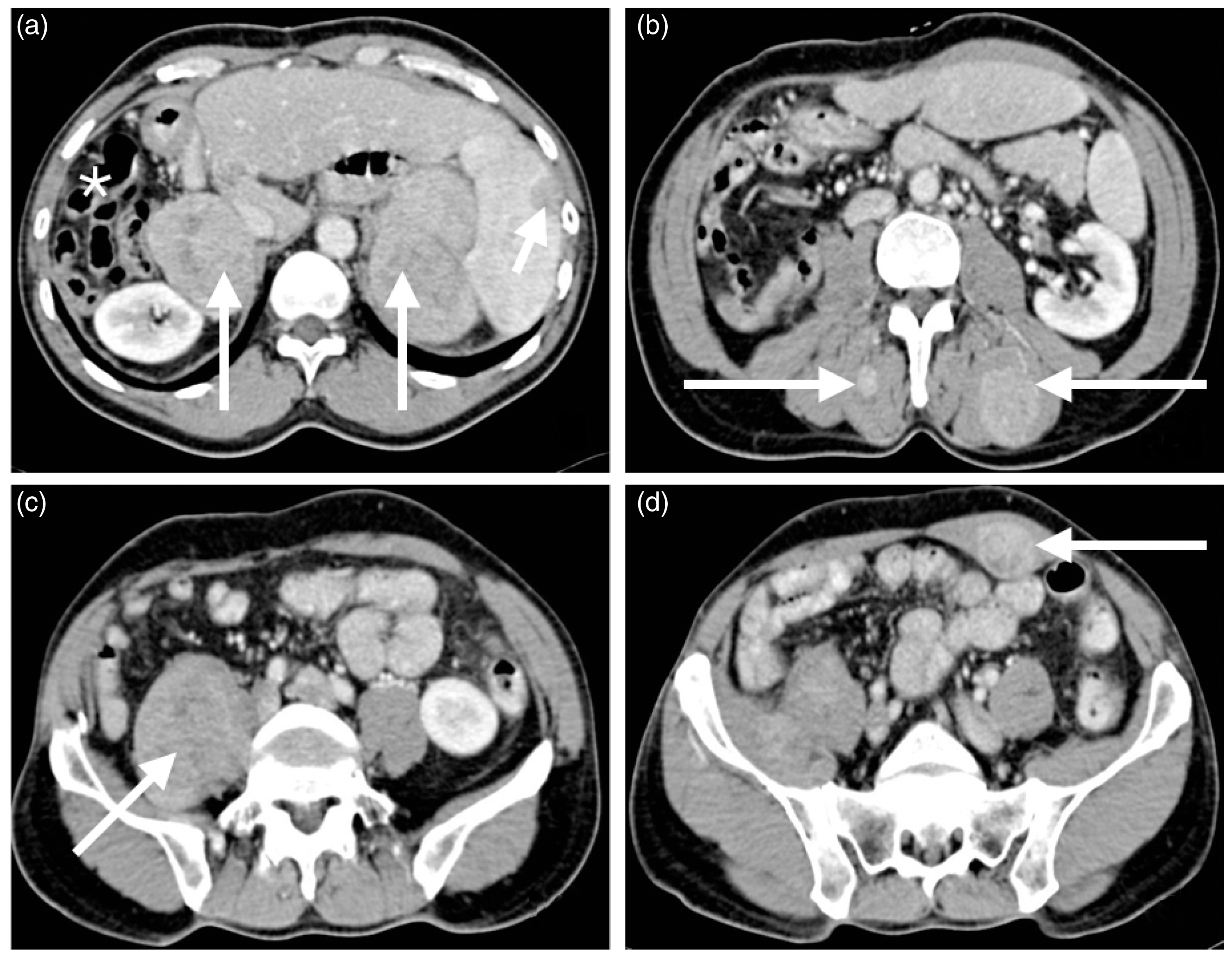
Discussion
Helal et al. in their study reported a total of nine cases (soft tissue [n = 7] and adrenal glands [n = 2]) out of a series of 47 patients diagnosed with extrahepatic metastasis at initial presentation (3). Other unusual musculoskeletal sites of extrahepatic metastasis have also been reported in the literature. These include reports by Subramaniam et al., Furumoto et al., and Wu et al., who reported extrahepatic metastasis to the left iliacus, intercostal muscle, and psoas muscle, respectively (4–6). Adrenal gland involvement was reported to occur in up to 8.8% of patients by Uchino et al. (7) and in 11% by Katyal et al. (2) in their studies.
Imaging plays an important role in the diagnosis, to stage the disease pre- and postoperatively, and even in therapeutic interventions such as endovascular procedures and loco-regional treatment. Radiologically, we noticed the skeletal muscle lesions to be slightly more enhanced in the arterial phase, with no washout during the porto-venous phase (Fig. 2). With the advent of new imaging modalities, molecular imaging, in particular positron emission tomography (PET) fused with CT, plays a more central role in the diagnosis of equivocal lesions. A meta-analysis by Lin et al. showed that 18F-FDG (18F fluorodeoxy glucose) PET/CT is useful to diagnose and stage extrahepatic HCC and proves invaluable in ruling out recurrent HCC (8).
Contrasted axial CT images in different acquisition phases (plain, arterial, and porto-venous phases) focused on the lesions at bilateral erector spinae muscles showing: (a) plain study shows the lesions to be hypodense; (b) marked enhancement relative to the plain scan noted during the arterial phase; and (c) no washout noted during the porto-venous phase.
Cutaneous and muscle metastasis following surgery or via needle seedling post biopsy has been known to occur. However, as shown by a meta-analysis (9), the risk is low, being 2.7% overall, or 0.9% per annum. This was unlikely in our case for two reasons: the superficial anterior abdominal wall lesions were located away from the surgical scar site; and it was four years after the primary operation. A study by Yang et al. suggested three patterns of recurring post-curative surgery in HCC (10). Pattern 1 is defined as the first intrahepatic recurrence followed by extrahepatic spread after repetitive intrahepatic recurrence, pattern 2 as simultaneous recognition of intrahepatic as well as extrahepatic metastasis, and pattern 3 as extrahepatic recurrence without intrahepatic involvement. What likely happened in our case was pattern 3. In any case, prognosis is poor once extrahepatic metastasis have developed.
Treatment in these cases remains controversial. To date there is no exact treatment regimen addressing metastatic lesions located in the skeletal muscles and bilateral adrenals. There is also no standard treatment strategy dealing with metastatic lesions without an intrahepatic component. Treatment modalities include a combination of surgery, chemotherapy, irradiation, TACE (trans-arterial chemoembolization), and percutaneous ablation. Uchino et al. showed that treatment for extrahepatic metastasis was only considered for those patients with Child-Pugh Class B and above, and even when pursued, complete remission is not guaranteed (7). In our case, due to the multi-focal nature of the extrahepatic metastasis, a conservative approach was undertaken.
In conclusion, HCC, being the commonest primary liver malignancy, proves a disease burden worldwide. Extrahepatic metastasis, albeit rare are known to occur. Post-surgical monitoring via clinical, biochemical, and imaging methods are indispensable and help in prevention or early detection of recurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.