
Abstract
Background
Although initial studies of neuroendovascular intervention did not review benefit over intravenous thrombolytics (iv r-tPA), recent studies have suggested otherwise. Elderly patients (age ≥80 years) are typically excluded from clinical trials.
Purpose
To examine the utility of mechanical thrombectomy based on patient outcomes.
Material and Methods
All stroke-alert activations at our health system from January 2011 to June 2014 were examined. All patients aged ≥80 years who had undergone mechanical thrombectomy were identified. Clinical characteristics included physiologic imaging findings, use of intravenous thrombolytics, baseline and postoperative National Institute of Health Stroke Scale (NIHSS), thrombolysis in cerebral infarction scores (TICI), and discharge destination.
Results
Mean NIHSS on presentation was 18.2 (range, 6–31), and 13.3 (range, 3–30) post thrombectomy. Three (16.6%) patients received iv r-tPA, two (11.1%) had symptomatic intracranial hemorrhage. Eight (44.4%) died, eight (44.4%) were discharged to nursing homes, and two (11.7%) were discharged to inpatient rehab and subsequently home. Favorable outcome was achieved in five (27.7%) patients. Fourteen (77.7%) patients had physiologic imaging prior to intervention. Three (75%) of four patients who did not have physiologic imaging prior to thrombectomy died. Thirteen (66.6%) patients had TICI 3 recanalization.
Conclusion
Our study showed that although there remains a role of mechanical thrombectomy in the treatment of acute ischemic stroke in very elderly patients, it is associated with significant higher morbidity and mortality compared to younger patients, but should remain a very viable treatment option when quality of life is the most important consideration.
Keywords
Introduction
As the treatment of acute ischemic stroke evolves, mechanical thrombectomies are being utilized for patients that have failed intravenous thrombolytics, or are not candidates due to unknown time of symptom onset. Although initial studies of neuroendovascular intervention did not review benefit over intravenous thrombolytics (iv r-tPA) (1,2), recent studies have suggested otherwise (3–5). This is likely due to improved study design, better patient selection, and the use of third generation stent retrievers, resulting in improved revascularization (6).
Very elderly patients (age ≥80 years) are largely excluded from clinical trials. The literature addressing this important patient population only comprised a recent analysis of anterior circulation ischemia from the RECOST study (7), and a retrospective cohort study for patients from the national database (8). In general, older patients also tend to have more severe strokes (9), less penumbra (from internal data), or relatively faster conversion to ischemic core due to decreased cerebrovascular reserve (10). Our study targets this neglected cohort of patients – the very elderly – and examines the utility of mechanical thrombectomy based on patient outcomes.
Material and Methods
Study design
Representative stroke trials and the age of patients represented.

Variables and outcome of interest
Clinical characteristics included physiologic imaging findings, use of intravenous thrombolytics, baseline and postoperative National Institute of Health Stroke Scale (NIHSS), thrombolysis in cerebral infarction scores (TICI), and modified Rankin Scale (mRS). Outcomes were considered favorable if the mRS was ≤2 at 3 months. In addition, discharge destination was also considered.
Statistical analysis
Statistical analysis was carried out using commercially available software (SPSS V.18, IBM Corporation, Armonk, NY, USA). All categorical data were analyzed with a chi-square test. Quantitative data with normal distributions were expressed as mean ± standard deviation. Two sample t-tests were used to analyze continuous variables with a normal distribution. A P value ≤ 0.05 was considered statistically significant.
Results
Baseline demographics with descriptive and univariate statistics for 18 study patients dichotomized by outcome.
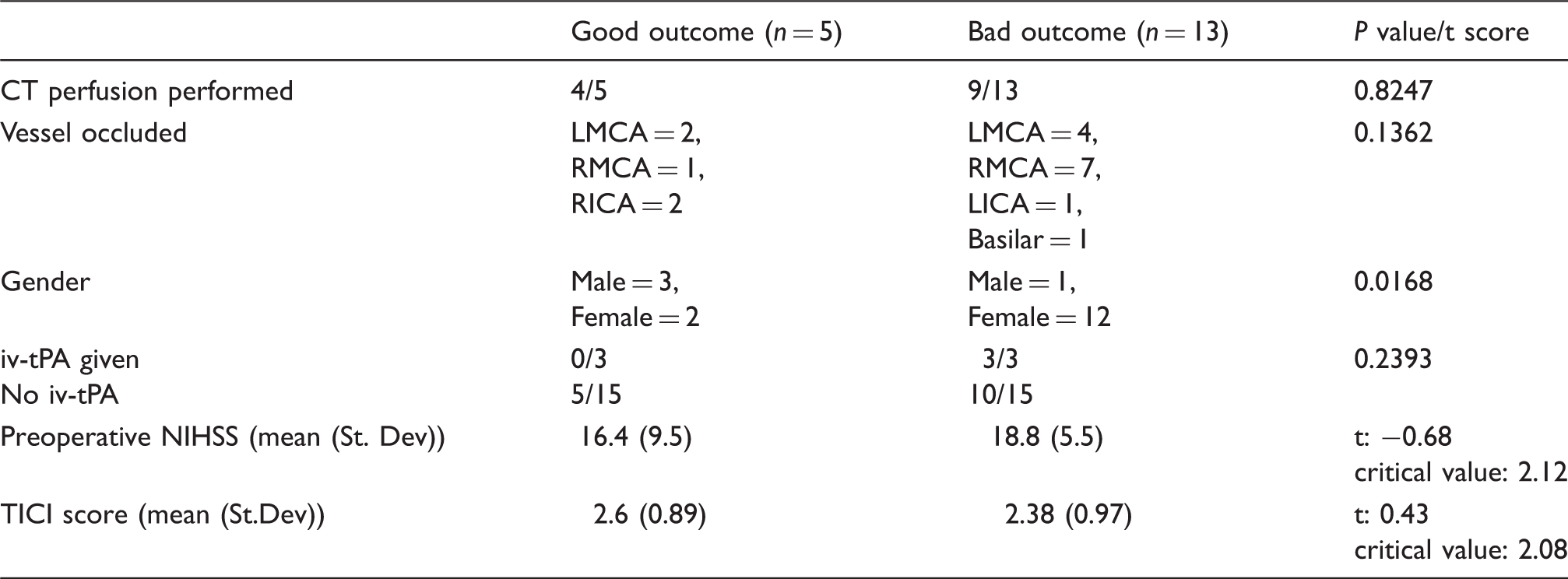
Each variable was tested independently for its association with good or poor outcomes (Table 2). Female gender was the only variable associated with poor outcome (P = 0.016). Interestingly, presenting NIHSS (t = −0.68, critical value = 2.12), use of preoperative CT perfusion (P = 0.82), administration of i.v. r-tPA (P = 0.23), site of vessel occlusion (P = 0.13), and postoperative TICI revascularization score (t = 0.42, critical value = 2.08) were not significantly associated with outcome, either good or poor.
Discussion
Mechanical thrombectomy has been increasingly utilized for treatment of acute ischemic stroke. Despite ongoing debates and conflicting evidence regarding its efficacy, mechanical thrombectomies increased six-fold from 2004 to 2009 (12). A review generated from the Center for Disease Control in 2009, stated that elderly patients (age ≥65 years) represent 66% of all acute stroke hospitalizations in the United States. Over half of these occurred in the very elderly (age ≥85 years) (13). Besides acute ischemic stroke, other areas of endovascular treatment such as aneurysmal subarachnoid hemorrhage in patients aged >80 years have also been recently studied (14).
Clinicians are increasingly faced with having to make the decision on whether to offer mechanical thrombectomy to those with large vessel occlusion whom either failed intravenous thrombolytics or are not a candidate due to various factors, and their hesitancy can be seen as only 0.2% of these patients received mechanical thrombectomy nationwide which is only one-third of the combined data when including their younger counterparts (13). Currently, no definitive recommendations are available that address who should or should not undergo this treatment. Support for intervention is based on recommendations derived from subgroups of larger studies, or based on anecdotal clinical experience (15). This study is the first of its kind to address this clinical gap.
In part, the debate pertaining to the efficacy of mechanical thrombectomy arose from randomized control trials such as the IMS-III and SYNTHESIS EXPANSION, which did not show a clinical benefit of mechanical thrombectomy over intravenous thrombolytics. However, the reliability of this evidence has been questioned with the published data from such trials as MR CLEAN, ESCAPE, and EXTEND-IA (1,2,4,5,16). Discrepancies between studies could be attributed to older generation thrombectomy devices, improving surgeon skill set, and an ill-defined patient selection process.
As expected, very elderly patients were found to have higher in-hospital and perioperative morbidity and mortality, with an independent association of poorer outcome in females as compared to males. Despite careful and strict patient selection criteria, very elderly patients still continue to have significantly poorer outcomes independent of penumbra on CT perfusion and despite improved TICI revascularization score post-thrombectomy. Interestingly, age is only responsible for 1.3% variation in functional outcome according to one study (17) if the patient survives the initial stroke. In fact, quite frequently, those patients with non-dominant hemisphere stroke gave their own consent to mechanical thrombectomy as they do not want to live with a significant disability.
There is no easy answer for this challenging clinical problem. The results of this study indicate that in patients aged over 80 years, death or functional impairment was found in over 70% of post-thrombectomy patients at 3 months. On the other hand, the 27.7% good outcome in this patient population should play a significant role in the decision-making when the alternative of not providing mechanical thrombectomy may result in almost universal bad outcome. We hope these data help to guide clinical decision-making and potentiates a realistic discussion between interventionalists and families about mechanical thrombectomy as a treatment option.
In conclusion, mechanical thrombectomy should remain a very viable option to patients when the quality of life is their most important consideration, particularly the very elderly.
Footnotes
Acknowledgements
The authors thank Beverly Walters and Vickie Gordon for their contributions in organizing and editing the manuscript. They also thank Omar Qahwash for his contribution and support in providing data for this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is funded by Providence Hospital Medical Education, and has received no external source of funding.