
Abstract
Susceptibility weighted imaging (SWI) combined with the FLAIR sequence provides the ability to depict in vivo the perivenous location of inflammatory demyelinating lesions – one of the most specific pathologic features of multiple sclerosis (MS). In addition, in MS white matter (WM) lesions, gadolinium-based contrast media (CM) can increase vein signal loss on SWI. This report focuses on two cases of WM inflammatory lesions enhancing on SWI images after CM injection. In these lesions in fact the CM increased the contrast between the parenchyma and the central vein allowing as well, in one of the two cases, the detection of a vein not visible on the same SWI sequence acquired before CM injection.
Introduction
Susceptibility weighted imaging (SWI) is a gradient echo sequence that provides additional information in the evaluation of various neurological diseases by enhancing the susceptibility contrast in the brain (1). In particular, susceptibility based magnetic resonance imaging (MRI) techniques are an invaluable tool to depict in vivo brain parenchymal veins (2,3).
SWI is usually accomplished by using T1-weighted (T1W) rapid acquisition gradient echo three-dimensional (3D) sequences, where both magnitude and phase images are saved. After phase image processing, a mask is created using phase data and it is subsequently multiplied by the magnitude images to produce the SWI (4).
In SWI, small veins are usually visible as a consequence of the combined effect of T2* signal loss and phase accumulation, instead contrast in the brain parenchyma mainly depends on T2* weighting.
As white matter (WM) lesions in multiple sclerosis (MS) typically develop around small parenchymal veins, MRI susceptibility contrast has been mainly used to characterize veins within inflammatory demyelinating WM lesions (5), a finding that may improve the diagnostic accuracy for MS (2).
It has been recently shown that intravenous injection of paramagnetic gadolinium-based contrast media (CM) has the possibility to improve the detection of small veins inside MS WM lesions, by using T2*-weighted magnitude and phase images (2).
In this report we present the cases of two WM lesions enhancing after CM injection from two different patients, one with a definite and the other one with a possible MS diagnosis. In both cases SWI was applied to investigate the effect of CM on intralesional vein detection when the lesion itself appears visibly contrast enhancing on the same sequence.
Case report
Case 1
A 52-year-old woman with a 7-year history of relapsing focal neurological deficits was admitted to the Neurological Department in order to establish a diagnosis. The patient had never been treated with immunosuppressive or immunomodulatory drugs. During the diagnostic workout, the patient underwent brain MRI examination on a 1.5T scanner (Magnetom Siemens Aera, Erlangen, Germany). The acquisition protocol included precontrast media injection (pre-CM) fluid attenuated inversion recovery (FLAIR), pre- and postcontrast media injection (post-CM) SWI, and 3D T1W MPRAGE. Post-CM SWI and subsequently the MPRAGE were executed 1 min after contrast administration. On pre-CM FLAIR images, a focal hyperintense WM matter lesion was detected in the left peritrigonal region (Fig. 1). The hyperintense lesion was also visible on the pre-CM SWI that showed in addition a small faint hypointense round shaped area in the center of the lesion attributable to a vein (Fig. 1b). After CM administration the lesion appeared hyperintense, visibly contrast enhancing, not only on the MPRAGE (Fig. 1c) but also on the post-CM SWI while the hypointense central area, previously barely visible on the pre-CM SWI, appeared now enlarged (Fig. 1d).
Left peritrigonal focal WM lesion (arrows) appearing hyperintense on (a) the axial pre-CM FLAIR and (b) the axial pre-CM SWI. In addition SWI shows a small faint hypointense area in the lesion center (magnified view) that can be ascribed to the presence of a central vein. (c) The lesion appears visibly contrast-enhancing on the axial post-CM MPRAGE and (d) the axial post-CM SWI. The hypointense vein (already visible on the precontrast SWI) here appears enlarged and the contrast between the small hyperintense contrast-enhancing lesion and its hypointense central vein, appears increased (magnified view).
Case 2
A 34-year-old woman with a diagnosis of relapsing remitting MS, currently under treatment with Fingolimod, underwent a brain MRI examination on a 1.5T scanner (Philips Achieva, Best, The Netherlands). The acquisition protocol included pre-CM FLAIR, pre- and post-CM T1W axial SE, and SWI. Post-CM SWI and subsequently the T1W SE were executed 1 min after CM administration. In this patient, an occipital periventricular WM lesion was detected (Fig. 2). Before CM injection, the lesion was hyperintense on both FLAIR and SWI, although the pre-CM SWI did not reveal any hypointense structure within the lesion area (Fig. 2a and b). After CM administration the lesion appeared hyperintense, visibly contrast-enhancing, on both T1W SE (Fig. 2c) and SWI. In addition, the post-CM SWI showed a linear shaped area of signal hypointensity in the center of the lesion previously not visible on the pre-CM SWI (Fig. 2d).
Occipital periventricular WM lesion (arrows) appearing hyperintense on (a) the sagittal pre-CM FLAIR and (b) the pre-CM axial SWI (magnified view). (c) The lesion appears visibly contrast-enhancing on the post-CM axial T1W SE and (d) the post-CM axial SWI. The post-CM SWI shows a linear shaped area of signal hypointensity in the lesion center, a parenchymal vein, which is not visible on the pre-CM SWI (magnified view).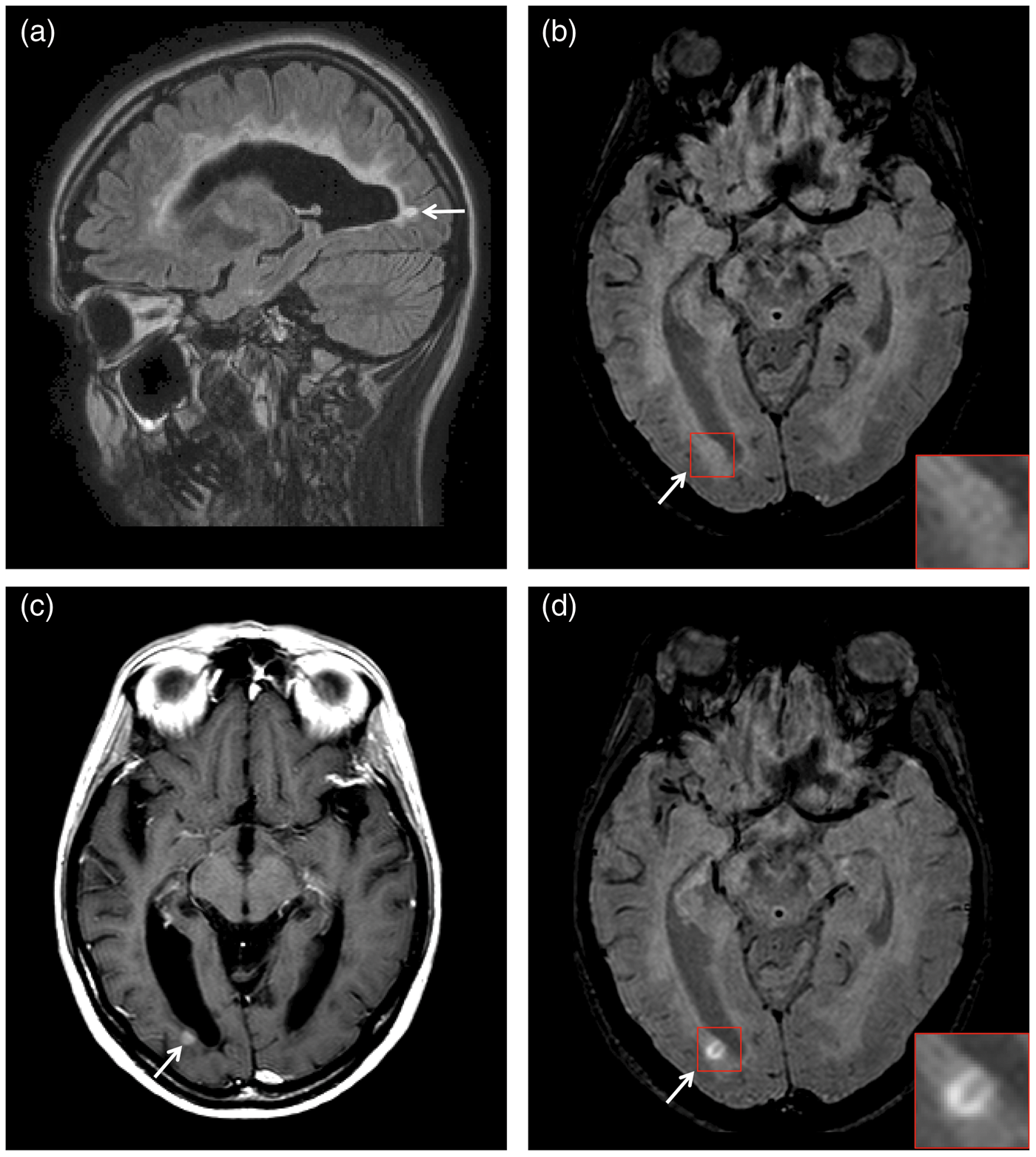
Discussion
This study describes inflammatory brain WM lesions in two patients (one with an established and the other with a probable MS diagnosis) where SWI have been applied to better characterize in vivo the pathophysiology of these lesions. In the first case, the pre-CM SWI identified a focal WM hyperintense lesion, with a corresponding central area of signal loss that can be ascribed to the presence of a central vein. This kind of signal pattern has already been described and it is currently under discussion whether SWI can be used in clinical practice to improve the differential diagnosis between MS and other inflammatory diseases (2,6). However, in this case, CM administration remarkably improved the contrast between the hypointense central vein and the surrounding hyperintense lesional parenchyma. Indeed the central vein appeared on the post-CM SWI as a more intense and enlarged area of signal loss surrounded by a slightly enlarged hyperintense area due to the subtle contrast enhancement of this lesion. Furthermore, as the perivenous location of WM lesions has been largely shown to be the most specific histopathological feature of MS (7), the presence of a central vein within the majority of brain WM lesions in this patient oriented us toward an MS diagnosis.
In the second case, the pre-CM SWI could not clearly identify a central vein within the lesion, which was visible on the SWI only after CM administration. In both cases the observed improvement of contrast intensity between the hypointense vein and the surrounding hyperintense lesional parenchyma was most probably determined by two distinct effects of paramagnetic CM: the more intense signal loss of intra veins water molecules (2), and the higher signal intensity in the contrast enhancing WM tissues, due to the shortening of T1 (8). The combination of these effects, the first obtained from phase, the second from magnitude data, increases the contrast between the central vein and the lesional parenchyma, allowing, in the second case, the detection of a central vein only on the SWI acquired after CM administration.
While the effect of gadolinium based contrast media on vein signal loss has been widely investigated (2,6), to our knowledge there are no reports describing the importance of tissue T1 shortening in vein detection after CM administration. This last effect can be observed only in contrast-enhancing lesion, where blood brain barrier disruption, due to the ongoing inflammatory process, allows CM to enter the lesion parenchyma (8).
In conclusion, gadolinium seems to improve the visibility of veins inside multiple sclerosis WM lesions when using SWI, and this appears to be remarkably conspicuous when the lesion itself is visibly contrast enhancing on the same SWI sequence.
Footnotes
Conflict of interest
None declared.