
Abstract
Objective:
To describe a method to retrieve cellular and tissue elements of oral squamous epithelium obtained by abrasive methods and to conduct investigations by cytohistology.
Method:
We developed a special gelatine pocket suitable for paraffin embedding of sparse material obtained from brush biopsies (BBs). This was subjected to combined evaluation of a cytological (smear) and histological examination of the ‘tissue sections’ – referred as cytohistology. Four diagnostic categories were applied for evaluation. Other special diagnostic methods were also applied in addition to recording dysplasia.
Results:
A total of 51, 755 BBs from suspicious lesions of the oral mucosa (mostly oral potentially malignant disorders – OPMD) were evaluated for the presence of carcinoma or dysplasia; in all, 1.7% were positive, 78.2% were negative for any epithelial atypia, 16.8% atypical and 3.3% inadequate. All BBs also had cytohistological evaluation. A ‘positive’ diagnosis by cytohistology was a reliable indicator of dysplasia or carcinoma, requiring further incisional/excisional biopsy. In the ‘atypical’ category, a variety of lesions were found, about half being dysplasia or carcinoma. This category challenges the clinician for further clinical, therapeutic and/or excisional examination. In ‘negative’ cases with persistence of the lesion, a re-examination in 1-year sequence is recommended.
Conclusion:
Cytohistology of material derived by abrasive methods allows earlier detection of dysplasia/carcinoma. A number of additional oncological and non-oncological findings make this method a valuable non-invasive diagnostic procedure for oral mucosal lesions.
Introduction
The American Academy of Oral Medicine (AAOM) recommends non-invasive, visual and tactile oral mucosal examination as part of the standard initial and recall evaluation by oral healthcare providers. 1 In a recent review of 16 oral cancer screening studies in Europe, compiled by Warnakulasuriya, 2 only 7 studies provided diagnostic confirmation by an adequate ‘second examination by a specialist’; for majority of cases, detected by screening, follow-up data were not available. Based on the evidence of 24 critically reviewed retrospective studies, Warnakulasuriya and Ariyawardana 3 identified advanced age, female sex, lesions exceeding 200 mm2, lesions of non-homogeneous type (e.g. erythroleucoplakia) and higher grades of dysplasia as determinants of malignant potential. Based on these criteria, highly suspicious lesions are surgically treated in most centres, but for the rest, the oral healthcare provider is still left with the highly unsatisfactory option to ‘watch and wait’.
In contrast, a gynaecologist discovering a worrisome lesion on the vulva or cervix uteri would apply standardized investigations by highly effective cytological screening: the so-called Pap test. Large-scale non-invasive cytological screening of cell smears from the cervical region, initiated by Georgios Papanicolaou, has been successfully applied to identify precancerous lesions. This has led to a reduction in mortality of cervical cancer considerably up to 70% in countries participating in cervical screening since the last century. 4,5
There have been many efforts and trials to employ exfoliative cytological methods for oral mucosal lesions. 6 However, initial results in the last century were disappointing due to high false-negative rates. Today improved retrieval of cellular and tissular material and advanced morphological methods have led to revival of cytological and cytohistological non-invasive methods to be utilized for investigating oral mucosal lesions rather than adopting the watch-and-wait option of oral healthcare providers. Application of cytohistology could change the current ‘watch-and-wait option’ to ‘watch and wait but with a twist’ implying some promising perspectives. 1
Oral mucosa versus the cervical mucosa
There are several morphological differences between the oral and the cervical epithelium responsible for the failure of application of exfoliation cytology to study oral mucosal pathologies. Several problems are encountered in the application of exfoliative cytology to study the oral mucosa.
These include: lack of a transformation zone as in uterine cervix; strongly cohesive nature of keratotic oral squamous epithelium; lack of sufficient single cellular elements in an abrasive sample; cell clumps and residual cellular/tissue material retained on the brush.
These problems demand site-specific solutions. Several solutions have been adapted by various investigators to overcome these limitations related to morphology of the oral squamous epithelium, ways of collecting samples and for further examination of harvested material. For sample collection, instead of using a spatula, abrasive retrieval methods were developed. 7 These include various curette techniques, ‘shaver-histology’ and ‘micro-deprider with tissue trap’, which allow scraping of the mucosa – termed ‘microhistology’’. 8 and the use of conventional gynaecological cytobrushes or conventional toothbrushes. 9,10 Furthermore, special brushes with hard bristles (e.g. Focal point ®, Oral CDx ®) are commercially available. The Oral CDx® brush has been employed for collection of most of the specimens examined in our laboratory and is referred to in the literature as ‘brush-biopsy’ (BB). 11 -16 ”
It is estimated that from a cervical cytology specimen more than 80% of the cells collected on the brush cannot be retrieved and go into the garbage. In an oral specimen, mostly larger cell clumps are harvested – which are traditionally a nuisance to professional cytologists. Solutions adapted were to develop liquid-based cytology which dissolved the cell clumps, but this leads to loss of the cell content and was unusable for cytology reporting in our laboratory. 17,18 However, quantitative cytology has been reported on liquid-based samples. 19 We adopted the cell block method, which allows the examination of tissue by the so-called cytohistology. 20
The cell block method
The cell block method has been adopted to replace routine cell smears when abundant cell-rich material can be found in body fluids such as in pleural effusions or ascites fluid. In these samples, abundant cell-rich material (often more than 10 µl pure cells) can be gained for embedding in a paraffin block following centrifugation. 21 -24
Specimens obtained from any surface epithelium contribute to a much lower harvest of cells. Furthermore, due to loss of cells in the process of dehydration and scattered distribution of cells following sectioning, the paraffin block method has not been feasible. Scraping of larger particles from the filter paper or the glass slide has sometimes been tried but leads to cellular damage. With liquid-based preparations as well as with the conventional cell block method, important diagnostic cellular elements and tissue particles are lost or are incompletely recovered.
The gelatine paraffin block method
For processing cellular and tissue material harvested using a brush or any other instrument, enveloping of the material gained by centrifugation is essential for acquisition and embedding of sufficient material. This step enables cutting of thin sections by conventional microtomes for diagnostic purposes. For this reason, we developed a special ‘pocket’ of gelatine (Figure 1), which contains the cells – like meat surrounded in a dumpling, ravioli or German Maultasche – often referred to as ‘Reutlinger dumpling’. The simple process has been patented but is available to all interested pathology laboratories. The cells and tissue fragments are dyed with methylene blue prior to embedding, and when cutting the paraffin block by step section, the presence of the cells and tissue at the correct level of the block can be readily identified. Using this method, the harvested material is nearly completely available for diagnosis (Figures 2 and 3).

Empty gelatine pocket: the collagen-rich fine granular gelatine is stained amphophilic.
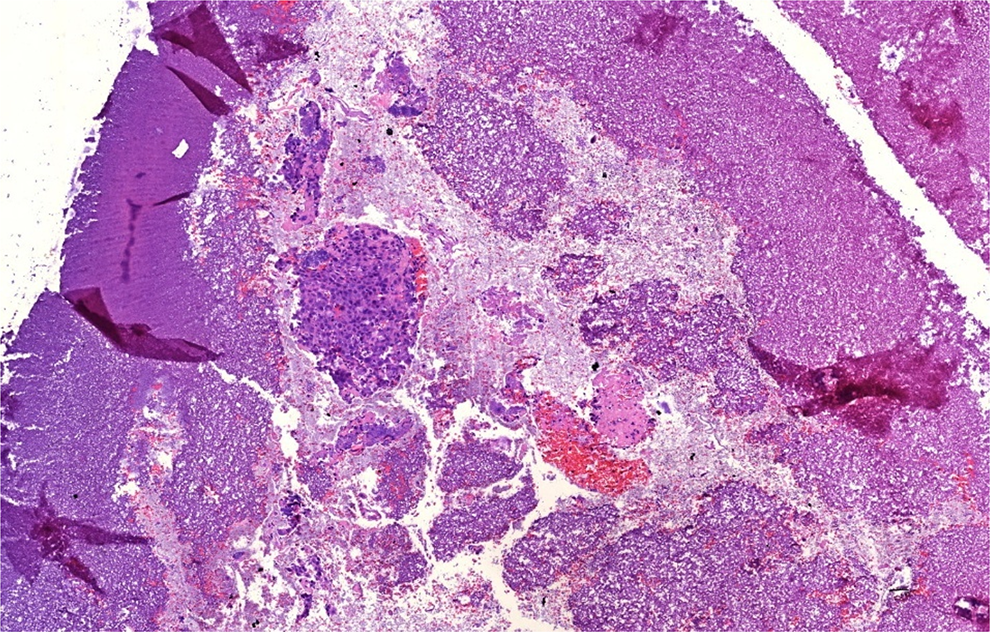
Gelatine pocket with tissue material from the brush. Markedly atypical tissue fragments from a carcinoma (‘positive’). Cutting artefacts of the gelatine mantle on both sides.

Fragments of a squamous cell carcinoma from a BB in a gelatine pocket (‘positive’). BB: brush biopsy.
Cytohistology
Other laboratories have employed various methods to prepare cell smear material collected from body surfaces for a cell block procedure. Figure 4 shows the four diagnostic categories used in reporting. Boon 25 reported a combined diagnostic approach termed ‘cytohistology’ using a cell block method, and the method is adapted by several others. 20,26 -28 Cytohistology has advantages beyond that of a cell smear, as additional diagnostic techniques – computer-assisted diagnoses, DNA cytometry, application of special stains, for example, for infectious agents and modern immunhistochemical and molecular pathological methods can also be applied (Figures 5 to 7). Cytohistology is thus a combination of cytodiagnostics and histological diagnosis on sections cut from a cell block.

Distribution of diagnostic categories of samples from OPMDs in 51,755 BB specimens processed by cytohistology. OPMD: Oral Potentially malignant disorder; BB: brush biopsy.

Immunohistochemistry of cytohistological specimens. High proliferative activity in a carcinomatous tissue fragment demonstrated by MIB1-antibody.

Immunohistochemistry of cytohistological specimen. Epithelial cytoplasmatic expression of the gamma 2 chain of laminin 5 as a sign of increased remodelling in a carcinomatous tissue fragment.

Immunohistochemistry of cytohistological specimens. Demonstration of podoplanin in carcinoma cells signalling metastatic potential.
Our objective is to report on our experience on cytohistology on a large sample of oral specimens.
Materials and methods
All oral specimens harvested by abrasive cytological methods between 2003 and 2017 were examined in our institute by cytohistology, that is, cytological examination of the cell smear and histological examination of cell block sections, gained by the aforementioned gelatine paraffin block method. In almost all cases, the Oral-CDx-Brush (CDx laboratories, Suffern, New York, USA) was used to obtain the BB. Less than 1% of the specimens were sent using other collection devices (cotton swabs, cervical brushes, etc.). The different anatomical sites of BBs and their frequency are given in Table 1. According to the clinical question posed and depending on the quantity and quality of the cellular and tissue material, conventional cytohistology and various additional advanced methods of diagnosis were employed. Standard stains used in all cases for cell smears was the Papanicolaou stain (PAP stain) and for cell block slides, we applied haematoxylin and eosin stain (H & E) and Periodic acid-Schiff (PAS) staining.
Anatomical sites of 7069 BBs evaluated by cytohistological evaluation.
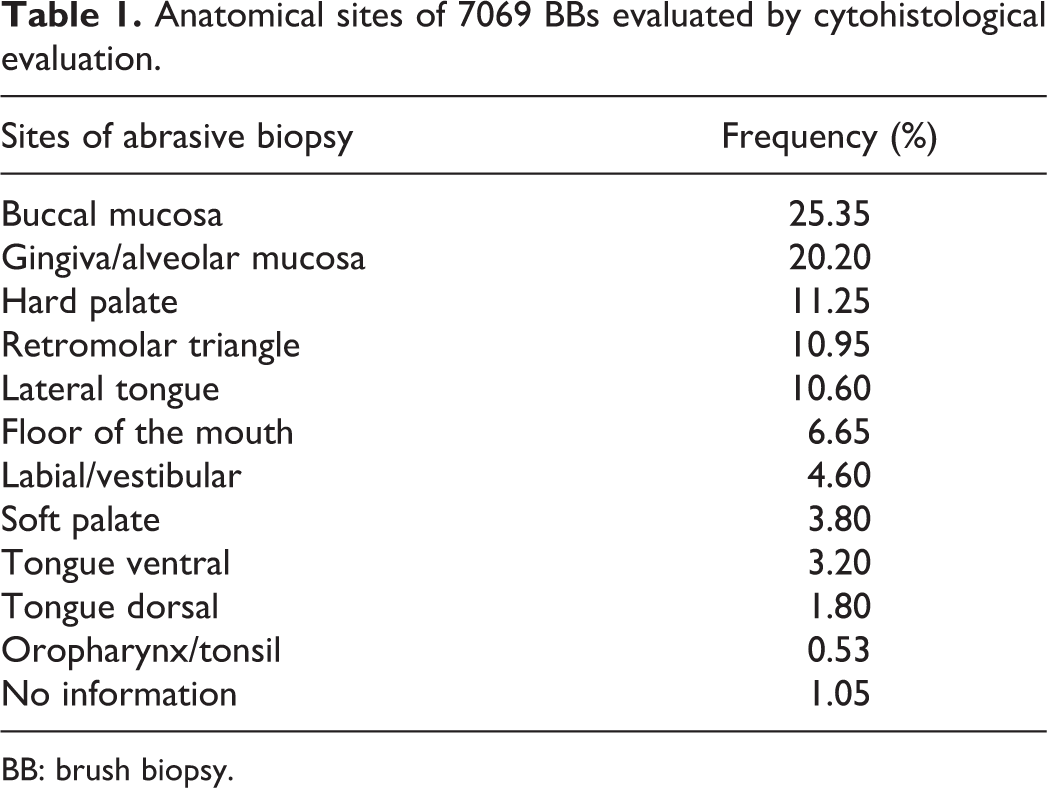
BB: brush biopsy.
The clinical question raised by referring clinicians for more than 99% of cases was to inquire about the presence or absence of dysplasia or malignancy. The standard diagnostic categories reported in every case were as follows: (i) positive for dysplasia or carcinoma, (ii) negative for epithelial atypia, (iii) atypical and (iv) inadequate. Final diagnoses were agreed by two pathologists using a double-headed microscope, and consensus was reached on every case.
For the assessment of malignant potential, advanced procedures used were immunohistochemical staining for Ki67, gamma 2 chain of laminin 5, P16, podoplanin (D2-40) and S100 A7. These were undertaken as routine procedures in our laboratory. For inflammatory lesions, differentiation of the cellular elements was undertaken according to the cytological or histological observations – differentiation of T- and B-cells (CD3/CD20), CD68, S100 and other standard immunohistological procedures were also employed (data not reported here).
In many cases, additional or alternative clinical diagnostic options were required. Most often Lichen planus had to be affirmed or ruled out. If it seemed reasonable, the following tests were undertaken: in case of lichen planus, CD20, CD3, CD68, CK 19 for basal cells, gamma 2 chain of laminin 5 as a marker for squamous epithelial cell remodelling 29 and Ki67 for proliferative activity; in case of suspected Candidiasis, if the PAS stain on the cell blocks slide was negative, restaining of the cell smear with PAS was done. In addition to the above-mentioned standard, categories concerning cancer or precancer when indicated the report included ‘additional findings’.
The following criteria were assessed and marked in the report if relevant and commuted as to their potential relevance: Epithelial changes: hyperkeratosis, basal cell degeneration, basal cell clusters, loss of polarity of basal cells, nuclear pyknosis, koilocytosis, desquamation of larger cohesive epithelial elements, ground-glass nuclei, multinuclear cells. Signs of epithelial regeneration. Inflammatory and stromal changes: inflammation (purulent, lymphocytic predominance), necrosis, granulation tissue. Erosion, ulcer when larger epithelial segments were found. Infectious agents: bacterial elements, especially filamentous bacteria, candida or other mycotic elements. The diagnoses ‘candida mycosis’ was given if penetration of epithelial cells by candidal organisms could be documented in the cell block sections.
Finally, an estimated semiquantitative scoring of the diagnostic quality of the cell smear and the histological slide of the cell block was reported separately on a scale of 1–10. The score took into account representativeness of cellular/tissue elements for the anatomical site, artefacts, quality of staining, state of preservation (fixation) and was semiquantitativety scored as 0 (no material) to 10 optimal (complete epithelial fragments). A score below 5/5 was considered inadequate or was questionable for representativeness.
Results
From 2003 to 2017, a total of 51,755 specimens obtained from various lesions of the oral mucosa harvested by abrasive methods were evaluated.
The clinical appearances reported by referring clinicians were 55% white lesions, 20% mixed white–red lesions, 15% red lesions and 10% erosions or ulcerations. The anatomical localizations of the specimens are listed in Table 1.
Concerning the standard question of concern to the clinicians whether dysplasia/malignancy could be present, the results were as follows: 40,472 cases were negative (78.2%), 880 cases positive (1.7%), 8695 cases atypical (16.8%) and in 1708 cases, the material was inadequate (3.3%) (Figure 4).
Compared with the evaluation of data obtained from only the cell smear, an increase of 8.6% of atypical/positive diagnoses was obtained by the addition of cytohistology. For candidiasis, there were 3% more candidal mycoses identified by cytohistology. This amounted to 5% of the cases positive for candida in the total sample, as reported earlier. 30 Most of these criteria were only diagnosable in the cell block material. The frequency of important additional findings reported to the clinician is given in Table 2.
Additional findings by cytohistology in the four diagnostic categories.a

BB: brush biopsy.
a2516 of 7069 BBs had important additional findings when evaluated by cytohistology.
Table 3 provides a comparison of results from BB against scalpel biopsy for specimens supplied by one of the clinical centres as reported earlier by Casparis et al. 31 Of the 263 BB samples received from this single centre, 56 also had scalpel biopsy diagnoses. In this analysis, all 7 ‘positive’ and 29 ‘atypical’ BBs were compared with scalpel biopsies (Table 3). Ten patients with atypical cellular changes were not biopsied, because either there was no longer any apparent mucosal change or the patients had refused scalpel biopsies. The pathology results from scalpel biopsy showed that all seven positive BBs were reported to demonstrate epithelial dysplasia and that three were oral squamous cell carcinomas (OSCCs). Of the atypical BBs, 17.2% were confirmed in the grade of mild dysplasia; 6.9% graded as moderate dysplasia; 3.4% were graded as severe dysplasia; and 6.9% were diagnosed as OSCC. Furthermore, scalpel biopsies were performed on 17 of the negative BBs and in all 3 inadequate BBs. Two of the 17 negative BBs were false negatives – one showed mild dysplastic features and the other was moderately dysplastic. Among one of the three inadequate biopsies, a squamous cell carcinoma was found in the scalpel biopsy.
Cytohistology results from BBs compared with histology diagnoses from scalpel biopsies.a

BB: brush biopsy.
a Data for 56 consecutive BB specimens received from one maxillofacial centre. Cytohistological reporting compared with scalpel biopsy diagnoses (adapted from by Casparis et al. 29 ); 56 specimens obtained by BB were classified by cytohistology as negative, atypical, positive and inadequate. These four groups are compared with scalpel biopsy diagnoses (adapted from by Casparis et al. 29 ).
The data from 56 cases (received from one maxillofacial clinic) with results from BBs and scalpel biopsies (Table 3) were statistically compared. The analysis achieved a sensitivity of 90% (confidence interval (CI) 69–97%) and a specificity of 44.1% (CI 29–61%). The PPV was 47.2%, and the negative predictive value (NPV) was 88.2%.
Additional subtyping of cancer and precancer
Due to the availability of additional histological sections in addition to negative/atypical/positive diagnoses in many cases, a more specific diagnoses or a tentative diagnosis could be given, particularly when whole epithelial particles were present (scores 8–10). This was undertaken often with the standard stains and in a few cases by DNA cytometry or with the use of immunohistochemical markers (Figures 5
to 8): Grade of dysplasia. Malignancy highly probable. Verrucous carcinoma suspected (due to keratin plugs, euploidy, confirmed by excision in three cases). Mucous forming adenocarcinoma possibly salivary gland origin (one case, confirmed as metastasis of a gastric carcinoma). White sponge nevus (white lesions in a 17-year-old male with spongiotic epithelial fragments with no atypia, diploid DNA cytometry), the suspected cytohistological diagnosis was clinically confirmed. Salivary gland lesions: pleomorphic adenoma, sialademoma papilliferum (differential expression of CK13 and 19; Figure 9). Peripheral ameloblastoma (typical inverse polar palisading and reticular stratum; Figure 10). Ectopic tonsillar tissue on the mandibular crest with ‘mucous’ discharge (atypial cells p16 positive, confirmed by excision).
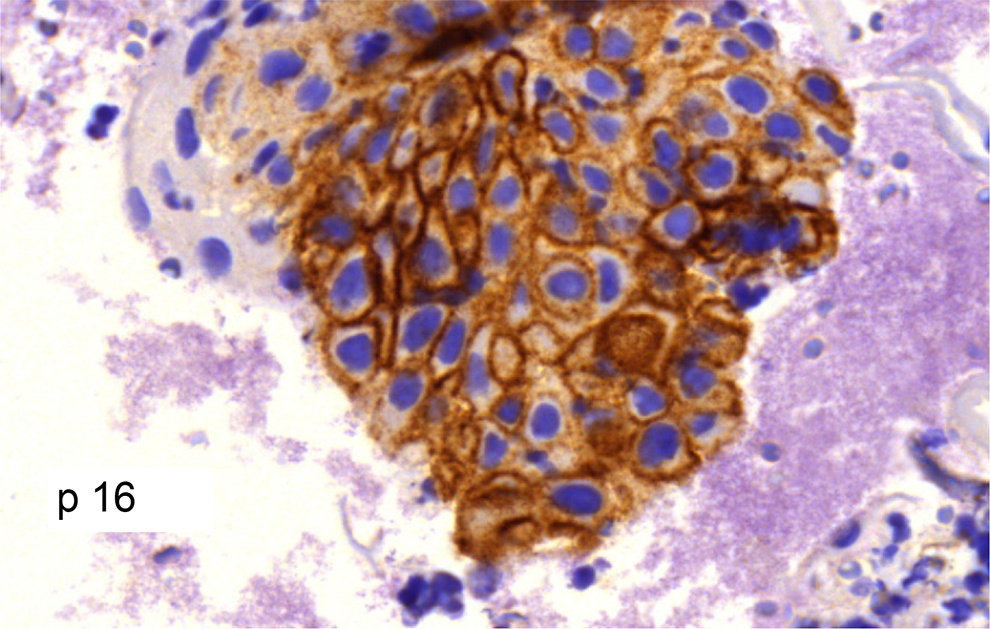
Immunohistochemistry of cytohistological specimen. Positive reaction for p16 in a carcinoma pointing to an association with human pillomaviruses of high risk.

Rare tumour entity in a cytohistological specimen. Fragments of a sialadenoma papilliferum. Typical biphasic differentiation of secretory and squamous epithelium.

Rare tumour entity in cytohistological specimens. Fragments of a peripheral ameloblastoma. Typical inverse-polar epithelial differentiation.
Non-oncological findings
Some inflammatory cells can be considered normal as they are regular constituents of normal oral mucosa. Marked inflammation was reported in 13% of the cases. This feature may arise from clinically unclear lesions such as erosions, ulcerative, pustular or bullous lesions. In two cases, granulomas were found; in one patient, sarcoidosis (Morbus Boeck), hitherto unknown, was clinically confirmed. Erosive and ulcerative lesions often showed signs of epithelial regeneration, and clinical controls were recommended. Candidamycosis was diagnosed in 5% of the cases.
Koilocytosis was a frequent finding, but by itself non-diagnostic for human papillomavirus-associated lesions and was often also found in Candidiasis. Ground-glass nuclei or multinuclear cells, suggestive of herpes virus lesions were present in less than 1% and confirmed by immunohistochemistry.
Mucodermatoses
Bullous oral lesions were readily diagnosable if the BB contained parts of the blister (score 8–10), but BBs were of little diagnostic use for this question (except for lichen planus).
In addition to dysplasia/malignancy, the clinicians posed the question of lichen planus in 25% of cases, especially in BBs from the buccal mucosa. Basal cell clusters, basal cell degeneration, lymphocytic predominance and harvesting of larger cohesive epithelial elements with basal cell destruction were suggestive of this diagnosis.
If relevant particles of the ‘blister’ were contained in the cytohistology, inflammatory lymphoid destruction of basal cells with strong expression of gamma 2 chain of laminin 5 and focal loss of proliferation were present, a confirmative diagnosis could be made and was confirmed in all cases by clinical findings.
Four cases of mucodermatoses discovered were incidental findings: Pemphigus vulgaris (Tzanck cells, epithelial fragments without basal cells; Figure 11). Benign mucous membrane pemphigoid (epithelial fragments with basal cells, no inflammation). Lupus erythematodes (similar to herpetic lesions but negative for herpes by immunohistochemistry). Chronic ulcerative stomatitis (CUS) – cytoplasmatic demonstration of immunoglobulins in basal cells.

Mucodermatosis in a cytohistological specimens. Dissociated epithelial fragments with formation of ‘Tzanck’ cells, typical of pemphigus.
These diagnoses were confirmed by the clinicians – enabling us to undertake what has been suggested as synoptic reporting. 32
Discussion
Adjunctive tests are used in addition to conventional visual and tactile examination to assist in the detection and evaluation of potentially malignant disorders 33 or for suspected squamous cell cancers of the oral cavity. These techniques have been reviewed recently. 34,35 Of the several adjunctive tests evaluated by different studies and reported in the literature, Lingen et al. 34 concluded that cytological testing applied for suspicious lesions appears to have the highest accuracy among various adjuncts (sensitivity: 0.92; 95% CI: 0.86–0.98; specificity: 0.94; 95% CI: 0.88–0.99). However, these studies reviewed were of low-quality evidence.
The term ‘brush biopsy’ is not clearly defined scientifically. Although most studies use this term, the actual test they are performing should be denoted as ‘brush cytology’, as their report is based on a cytological smear. Only an additional cell block allowing the use of histological sections in our view justifies the term ‘biopsy’. As in every cytological and histological examination, also in cytohistology, the diagnostic yield is largely determined by the quality of the abraded cells and tissue elements. With a large number of clinicians submitting BB material to our laboratory, the quality of the specimens was not necessarily standardized. As no other studies on cytohistology (with cell block) on oral brush specimens have been undertaken, it is difficult to compare our data with the results from other studies. The most closely related results gained by computer-assisted smear evaluation (CDx) were published by Carroll 15 on 75,652 specimens. Kerr 1 scoring the quality of methods for all early recognition of oral cancer or precancer techniques gave this method a score of 8, being the best available among adjunctive techniques evaluated so far. None of the adjunctive techniques scored 9 or 10 on his scale.
The so-called ‘brush controversy’
36
-40
is focused on rare false-negative and false-positive cases that can be encountered when using this method. It addressed mainly problems of cellular harvesting by the clinician and overconfident diagnosis by the pathologist and does not pertain to our additional diagnostic certification by cytohistology. Mehrotra
41
has examined the factors contributing to discordant data between BBs and histopathology reporting and provided the following explanation: ‘Within a given oral lesion, dysplasia may be multifocal and unless the two biopsies happen to sample the same part of the dysplastic lesion, the results may well be discrepant. Most importantly, the histologic diagnosis of dysplasia is not easily reproduced amongst oral pathologists and therefore a discrepant result between brush biopsy and scalpel biopsy may in fact even represent a false negative or false positive scalpel biopsy result.’
Follow-up for cancer and precancer
Negatives and false negatives
The main limitation in the analysis of specimens received in our laboratory was related to the lack of follow-up information from referring centres. It was impossible to contact all the clinicians or patients and to initiate a review of tens of thousands of patients. There were five spontaneous reclamations concerning carcinomas in previously reported ‘negative’ cases. In four cases, a different location to the original BB and subsequent development of carcinoma could be ascertained; in one case, specimen reported by us was not optimal (score 6/6) but was graded ‘negative’, but actually should have been classified as ‘questionable’.
The recommendation to follow-up every persistent negative lesion once a year by BB should exclude any significant risk to the patient of a false negative reporting. Considering a more than 10-year long evolution of malignant transformation, 42 this seems feasible. The option of BB avoids the repeated necessity of undertaking scalpel biopsies in negative cases.
Of the 204 ‘negative’ results on BBs received from the dental clinic of the University of Zürich (Switzerland), 17 were rebiopsied and 1 mild and 1 moderate dysplasia have been reported. Among the negative group, there were no severe dysplasias or carcinomas. Further details on our Zurich sample can be found in an earlier publication. 31
Atypical and positive cases
Two studies with follow-up information of patients who underwent BBs were published earlier – one from the University of Zürich 31 and one from the University of Berlin – Charité 43 (Table 3). Data were available for each of the four categories. In all ‘positive cases’ reported by cytohistology, a later scalpel biopsy found dysplasia (mostly severe) or invasive carcinoma. In other words, none of the seven positive BBs that required scalpel biopsies were false positive, meaning that the sensitivity would be 100%. Therefore, the diagnosis of ‘positive’ by our method is a reliable indicator for urgent necessity for further action – scalpel biopsy or excision.
In a comparable study, Hohlweg-Majert 44 reported four positive cases in which carcinoma was not found but do not state whether dysplasia was present or not, in the BB.
A problem lies with the ‘atypical’ cases making up roughly 15% of cases. Approximately half of these may actually contain dysplasias or even carcinomas.
The spectrum of lesions found in excisional biopsies compiled from the earlier cited studies 31,43 is listed in Table 4. The supposedly ‘normal’ findings in six cases have not been reviewed and checked for validity or representativity of the histology.
‘Atypical’ and ‘positive’ cases – confirmed diagnoses with follow-up.a

BB: brush biopsy.
a Pooled data of two follow-up studies of BBs with cytohistological evaluation of the Departments of Oral Surgery/Maxillofacial Surgery of the University of Berlin (Charité; 31) and the University of Zurich (Switzerland; 29). ‘Atypical’ and ‘positive’ categories in 196 cases, available information on 101 cases.
Candidamycosis is by far the most important infection as it may be the cause of a white and red mucosal lesion and represents mostly reversible cellular changes difficult to distinguish from precancerous atypia/dysplasia. Long-standing candida infections by itself may play a role in malignant transformation.
Kerr 1 listed requirements for an acceptable non-invasive test for potentially malignant or oral lesions: availability, easy use, acceptable to patients, immediate results, inexpensive, separation of risk/no risk and help in the selection of the site of biopsy. The cytohistological method we offer fulfils most of Kerr’s criteria, and the only setback is that the sequential multimodal approach requires some time and thus does not give immediate results. This may be acceptable in view of the many years that malignant transformation requires.
Speight et al., while discussing the need for improving screening tests for oral cancer, emphasize the need for more accurate adjunctive tests. 45
Improving accuracy and reporting
The pitfalls of oral cytology and ‘brush biopsy’ are well known 46,47 : Only superficial cells are harvested, ulcerative/necrotic lesions and infectious lesions may not yield many squamous cells, fixation is compromised and most smears show mechanical and stain artefacts. These factors lead to a high rate of cytology reports marked as ‘inadequate’. However, by employing cell block cytohistology, the rate of inadequate reports could be minimized; and in our study, inadequate reports were limited to 3.3%.
During reporting the most important problem encountered by the pathologist is distinguishing reactive atypia from true dysplastic features. Rarely there are interpretational errors especially when architectural feature of a reactive nature are present in the cellblock sections.
The accuracy of diagnosis can be considerably enhanced by DNA measurements and nuclear morphometric analysis on the cytological smear
48
done by us in exceptional cases. Immunohistochemistry in suspicious cases with representative epithelial elements in the cell block. Using these additional techniques we were able to give specific diagnoses in many cases.
In our evaluation, we used the nomenclature used by the CDx Laboratories.
A refined grading system was suggested by Afrogh et al.
49
: normal reactive (inflammatory reactive, repair, radiation- and chemotherapy-induced) atypical changes atypical changes probably reactive low-grade squamous intraepithelial lesions atypical, probably high grade high-grade intraepithelial lesions invasive squamous cell carcinoma.
This classification in our opinion requires a thorough clinical–pathological evaluation and is not entirely suitable for submitted specimens. The category ‘atypical’ is a clear indication for the clinician sending in the specimen that further clinical and/or histological examinations are necessary. Edwards 32 postulated for a synoptic reporting a subtle morphological examination and consideration of the overall clinical presentation. This implies careful clinical examination, correct interpretation of the cytohistology report and experience is essential for the patient management. This includes carefully taking into account the ‘additional findings’ in the cytohistological report, that is, candidamycosis, inflammation, erosion, which may require treatment and further control. In suspicious cases, re-BB or scalpel biopsy/excision are warranted if no regression can be observed in 6–8 weeks.
A problem of the cytohistological diagnostic system generally is the question of lack of control. Histology (on larger specimens) is often referred to as the ‘gold standard’ in cancer diagnostics. This, however, may be debatable. It is an everyday experience that a ‘positive’ Pap smear certified by many experts often lacks a correlation in the subsequent conisation specimen. Holmstrup et al. 50 demonstrated in 101 oral lesions that a comparison of the degree of dysplasia in biopsies with that of the whole lesion examined in step sections showed considerable variations, with concordant diagnosis only in 49% of the lesions. Lee et al., 51 in a similar study of 200 leukoplakic lesions, stated an agreement rate between incisional biopsy and resection specimen of only 56%.
The published literature does not compare ‘false-positive’ cases by different methods of investigations. Such studies may expose reasons for discordant data and allow us to understand any limitations of the technique or reporting faults. What has been researched has been in essence the ‘interobserver variations’. The interobserver concordance among six experts in 120 oral scalpel biopsy specimens with the question of dysplasia was only 50.5%. Moreover, for the question ‘presence of dysplasia: yes or no’ the concordance among experts was 81.5%. 52 Speight et al. 53 have recently demonstrated how the use of a defined protocol and taking a face-to-face consensus review resulted in a substantial increase in diagnostic agreement.
The detection of infectious diseases of the oral mucosa is not the primary aim of cytology or cytohistology in this study. However, a number of bacterial, parasitic, fungal and viral agents can be diagnosed; in the setting of cancer and precancer screening, only a few of these infectious diseases are relevant: herpes virus and human papillomavirus associated cellular changes, and rarely cytomegalovirus; more or less ubiquitous filamentous bacteria (actinomyces) only in the context of ulcerative/ erosive lesions with tissue/cell-invasion; black-hairy tongue may be identified by massive bacterial harvest.
Carroll 15 in her series of 75,652 BBs was able to give a specific histological diagnosis of surface lesions and sometimes also of submucosal odontogenic and non-odontogenic jaw lesions. These include Fordyce spots (ectopic sebaceous glands, lymphoid cysts, ectopic lymphoid/tonsillar tissue, salivary gland tumors (mucoceles, pleomorphic adenoma, sialadenoma papilliferum, peripheral amelobastoma (stellate reticulum), pigmented lesions (melanotic macule, amalgam tattoo), herpes virus lesions (cave: aneuploid!).
There are further applications of the abrasive cytohistology for the diagnosis of mucocutaneous lesions of the oral mucosa especially for pemphigus vulgaris (Tzanck cells), but so far this was not the mainstream purpose of the procedure, as the evaluation of this service was aimed at potentially malignant disorders. 33
Conclusion
Cytohistology combines the advantages of cytology and histology, with the possibilities to apply the whole spectrum of advanced diagnostic techniques. Being non- or minimally-invasive, it can be repeated without limitations and offers a valuable addition to the diagnosis of oral mucosa lesions – especially targeted for cancer screening of the oral and oropharyngeal mucosa.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.