
Abstract
Objectives:
To quantify endocytosis of keratinocytes (EK) in oral squamous cell carcinoma (OSCC) and correlate it with different clinical and histopathological parameters. Further, the expression of cluster of differentiation 68 (CD68) and lysozyme was studied in tumor cells to corroborate this phenomenon.
Materials and method:
EK per high-power field (HPF) was calculated on hematoxylin and eosin-stained sections and correlated with clinical and histopathological parameters. CD68 and lysozyme were studied in tumor cells using immunohistochemistry.
Results:
The mean EK per HPF was higher in stage IV (4.450 ± 2.241) than stage III (3.333 ± 1.543) OSCC (p = 0.1978). Although there were more EK in N2 stage (4.362 ± 0.3405) as compared to N0–N1 (3.462 ± 0.4178), the results were statistically insignificant. Statistically significant difference in mean EK was observed in all the grades of OSCC: well versus moderate (p = 0.0052), moderate versus poor (p < 0.0001), and well versus poor (p = 0.0001). There were significant differences in the mean EK (p < 0.05) between different grades of stromal degenerations (mild: 2.654 ± 1.093, moderate: 5.115 ± 1.774, and severe: 7.250 ± 2.217). Statistically significant differences were observed in CD68 expression in tumor cells of various TNM stages (p = 0.049), histopathological grades (p = 0.045), and stromal degeneration (p = 0.024). Likewise, lysozyme expression in tumor cells was also statistically significant in histopathological grades (p = 0.004) and mean EK value (p = 0.0119).
Conclusion:
The mean EK in OSCC increases with increasing histopathological grades, TNM stages, and stromal degeneration. CD68 and lysozyme can be used as markers of EK in OSCC.
Introduction
Endocytosis of keratinocytes (EK) is an important morphologic feature to distinguish benign from malignant lesions. EK has been described previously in breast carcinoma, 1 giant cell carcinoma of lung, 2 gall bladder carcinoma, endometrial stromal carcinoma, 3 malignant thymoma, 4 malignant melanoma, 5 and so on, and is correlated well with the aggressiveness, degree of anaplasia, invasiveness, and metastatic potential of the malignancy. Demonstration of an increased number of EK may also be helpful in grading breast carcinoma. 1 Our laboratory first reported EK in oral squamous cell carcinoma (OSCC) in five cases and proposed the terminology called “complex cannibalism.” 6 We are also the first to report endocytosis of stromal cells in central and peripheral giant cell granulomas of the oral cavity. 7 It is concluded that the endocytosis of stromal cells by giant cells can be used to predict biological behavior of the lesions.
Transformation of tumor cell into endocytic cell (cell performing EK) is a phenomenon, which involves complex framework of molecular events. Markers that are implicated in EK process are cluster of differentiation 68 (CD68), lysozyme, caveolin-1, actin, ezrin, cathepsin B, nine transmembrane segments, vimentin, Rho-associated protein kinase (ROCK)–actin/myosin pathway, and so on.
8
CD68 is a 110-kDa transmembrane glycoprotein, highly expressed by monocytes and tissue macrophages, classified as a member of the scavenger receptor family; it contains a lysosome-associated membrane protein-like domain.
9
Lysozyme is a single-chain polypeptide of 129 amino acids cross-linked with four disulfide bridges. It hydrolyzes b(1AE4) linkages between N-acetylmuraminic acid and N-acetyl-
With this view in mind, the present study was designed to evaluate EK in tumor cells of OSCC with clinical–pathological correlation. The study further explores the expression of phagocytic markers (CD68 and lysozyme) in the tumor cells to corroborate this phenomenon.
Materials and methods
The scientific and ethics committee of the institute approved the present study. From the year 2010 to 2014, 150 cases were screened for histopathological evidence of EK in tumor cells of OSCC. Cases showing endocytosis of neutrophils, lymphocytes, and red blood cells (RBCs) by tumor cells were also considered. Totally, 56 (37.33%) cases were identified and selected for clinical–pathological analysis and immunohistochemical analysis. The details of the demographic data are shown in Table 1.
Patients and disease characteristics with mean endocytic cells per HPF.
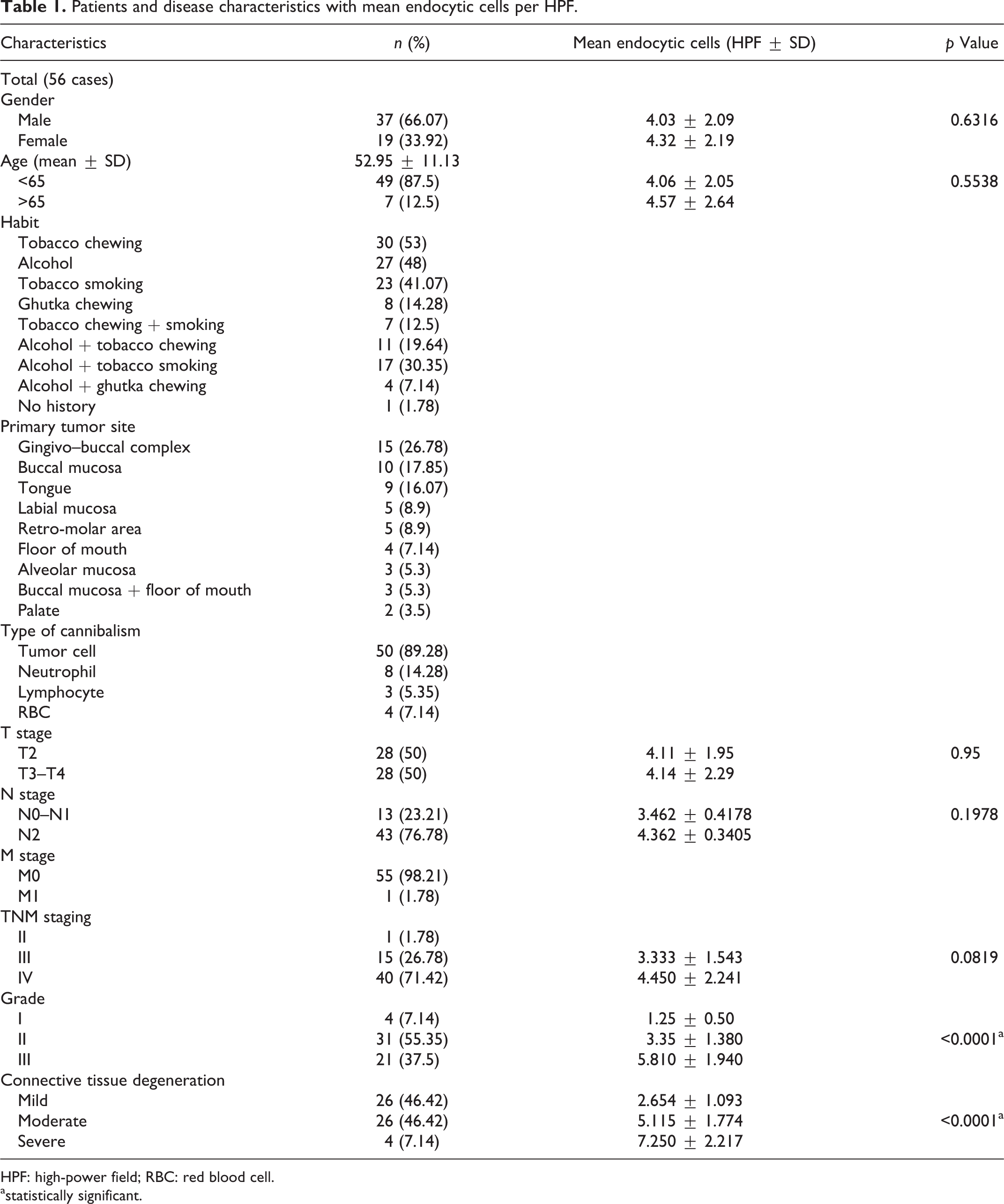
HPF: high-power field; RBC: red blood cell.
astatistically significant.
Identification of EK
The morphology of the classically described EK is composed of a crescent-shaped nucleus engulfing another cell with a round to oval faded (smudged) nucleus. This particular feature is mostly due to the fact that the ingested cell is contained in a big vacuole that pushes the nucleus of the endocytic cell, squashing it at the periphery of the cell. Brouwer et al. 11 proposed the successive steps in the process of EK. At first, the endocytic cell comes in contact with the free cell. This is followed by the gradual engulfment of the cell cytoplasm of the free cell. The nucleus of the free cell is unaltered; however, the nucleus of the endocytic cell changes to a semilunar shape. Finally, the free cell completely dies off and its nucleus disintegrates.
Sections were observed with a 40× objective under a light microscope at three different fields, which showed maximum density of such a phenomenon. The average of three different fields was calculated and expressed as number of EK per high-power field (HPF). Overlapping of tumor cells, dyskeratotic cells, koliocytic cells and degenerating cells were carefully examined and excluded during evaluation.
Immunohistochemical analysis
For the immunohistochemical study, 3-µm sections were obtained from the formalin-fixed paraffin-embedded specimens of the lesions. Immunohistochemical staining was carried out using the streptavidin–biotin–peroxidase complex method. The following antigens were evaluated: CD68 (macrophage-associated monoclonal antibody, KP-1 clone, 1:50; BioGenex, Fremont, California, USA), incubated at room temperature for 1 h; lysozyme (rabbit polyclonal antibody, BioGenex), incubated at room temperature for 30 min. For CD 68, the tissue sections were previously treated with citric acid in three cycles for 5 min and no pretreatment was recommended for lysozyme. Diaminobenzidine was used as chromogen. Lymph node was used as positive control for CD68 and lysozyme.
A semiquantitative method was used to score the CD68 and lysozyme expression in the epithelium of OSCC, as previously described by Soini et al. 12 Scoring was based on (a) the intensity of the immunostaining in the malignant cells (0 = absent, 1 = weak, 2 = moderate, 3 = strong, and 4 = very strong) and (b) the percentage of positive malignant cells (0 = 0% positive cells, 1 = <25% positive cells, 2 = 25–50% positive cells, 3 = 50–75% positive cells, and 4 = >75% positive cells). The final immunostaining score was determined by the sum of (a) and (b). Final scores ranged from 0 to 8 (0 = absent, 1–4 = weak, and 5–8 = strong).
Statistical analysis
Data collection was conducted using the Microsoft Office Excel package and processed with the SPSS 16.0 software package (SPSS Inc., Chicago, Illinois, USA) for the statistical analyses. The Student’s t-test and/or Fisher’s exact test was used to assess the differences among quantitative variables and qualitative variables, respectively. All the tests were two-sided, and p values < 0.05 were considered statistically significant.
Results
Histopathological analysis of EKs
Both complete and partial EK were observed in the present study (Figure 1(A)). Some endocytic cells showed degradation of internalized cells. The cells ranged from 1 to 10 with a mean of 4.125 ± 2.107. The phenomenon of complex EK was observed in 9 (16.07%) cases (Figure 1(B)). Eight cases (14.28%) displayed endocytosis of neutrophils. Neutrophils were abundant and could be identified both within the malignant epithelial cells as well as in the stroma adjacent to the tumor cells (Figure 1(E)). Both partial and complete neutrophil engulfment were seen by tumor cells in all the cases. At many places, multiple neutrophil engulfment with moth-eaten nuclear appearance of endocytic cell was observed (Figure 1(E)). The internalized neutrophils showed different stages of degeneration. The neutrophils showed striking tumoral-centric distribution, decreasing in number away from the tumor cells. Maximum of five and minimum of eight neutrophils showing endocytosis per HPF were observed with a mean value of 5.875 ± 0.99. Similarly, lymphocytic and RBC endocytosis by tumor cells was reported in three cases each (Figure 1(D)). Surprisingly, in two cases, we also noted an extremely rare phenomenon in which the engulfed cell was undergoing mitotic division (Figure 1(F)).
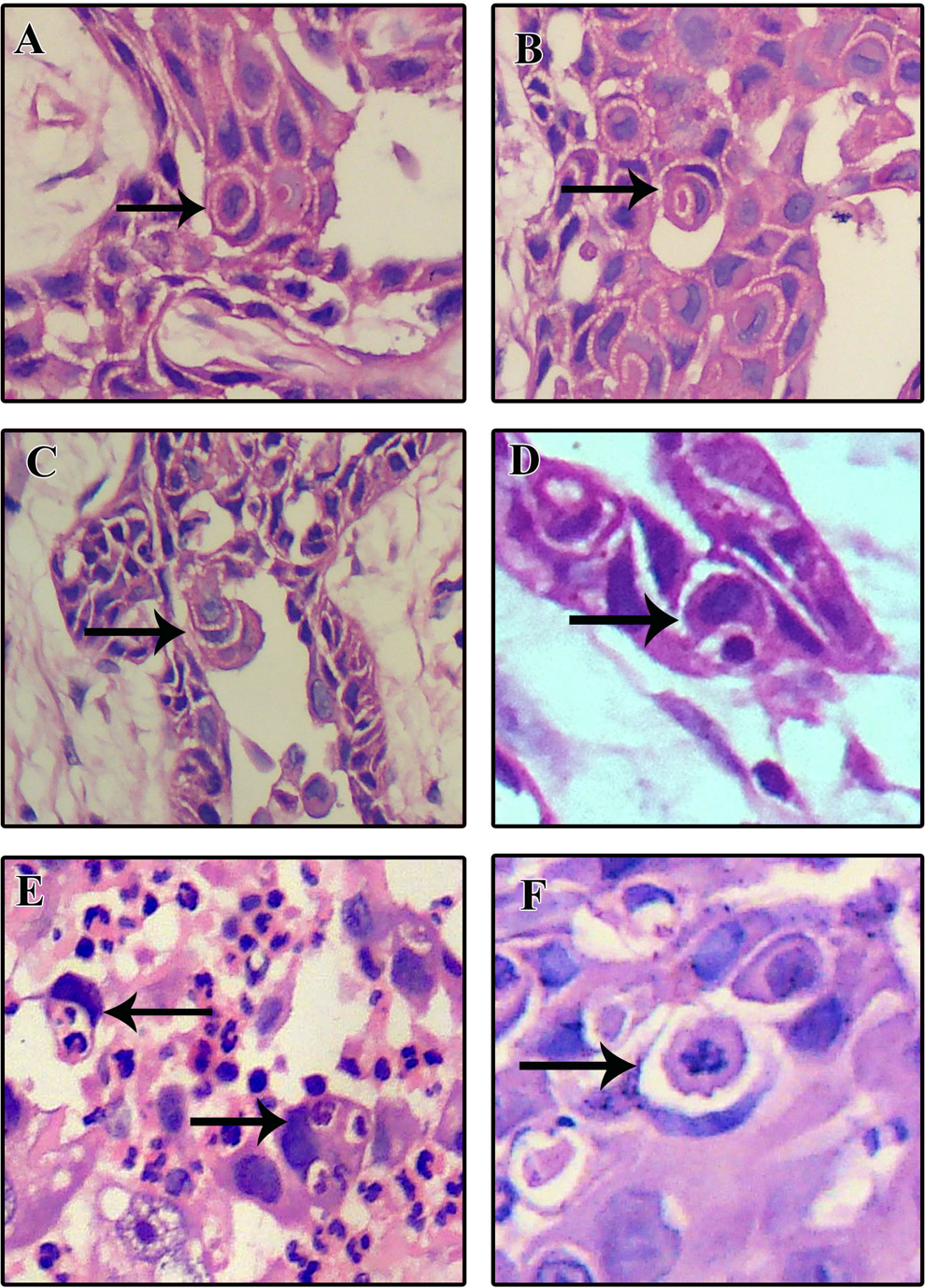
Photomicrograph showing complete endocytosis (A), complex endocytosis (B), endocytosis in acantholytic cells (C), lymphocytic endocytosis (D), neutrophilic endocytosis (E), and mitotic activity in internalized cell (F). The phenomenon is indicated by a black arrow. (Hematoxylin and eosin stain; original magnification ×400.)
TNM stage and EKs
Maximum cases were in stage IV (40; 71.42%), followed by stage III (15; 26.78%) and stage II (1; 1.7%). Since there was only one case in stage I, it was not included in the statistical analysis. The mean EK was higher in stage IV (4.450 ± 2.241) than in stage III (3.333 ± 1.543), with a statistically significant difference (t = 1.304; p = 0.1978; df = 54). Although there were more EK in the N2 stage (4.362 ± 0.3405) as compared to N0–N1 (3.462 ± 0.4178), but the results were not statistically significant (t = 1.304; p = 0.1978; df = 54; Table 1).
Histopathological grading and EKs
Of the 56 cases, 31 (55.35%) were moderately differentiated followed by poorly differentiated (21 cases; 37.5%) and well differentiated (4 cases; 7.14%; Figure 2). More numbers of mean EK were reported in poorly differentiated OSCC (5.810 ± 1.940) followed by moderately differentiated (3.35 ± 1.380) and well differentiated (1.25 ± 0.50). There was statistically significant difference between all the grades: well versus moderate (t = 2.992; p = 0.0052; df = 33), moderate versus poor (t = 5.993; p ≤ 0.0001; df = 50), and well versus poor (t = 4.598; p = 0.0001; df = 23). Three cases of acantholytic/adenoid OSCC showed maximum mean EK (10, 8, and 7; Table 1).

Photomicrograph showing well (A), moderate (B), and poorly (C) differentiated OSCC. The cannibalism is shown by black arrow. (Hematoxylin and eosin stain; original magnification ×400.) OSCC: oral squamous cell carcinoma.
Stromal degeneration and EKs
There were 26 cases of mild and moderate stromal degeneration each, followed by four cases of severe degeneration (Figure 3). Mean endocytic cells were calculated in each group (mild: 2.654 ± 1.093, moderate: 5.115 ± 1.774, and severe: 7.250 ± 2.217). The differences in mean EK between these three groups were found to be statistically significant: mild versus moderate (t = 6.024; df = 50; p ≤ 0.0001); mild versus severe (t = 6.778; df = 28; p ≤ 0.0001); and moderate versus severe (t = 2.176; df = 28; p = 0.0381; Table 1).
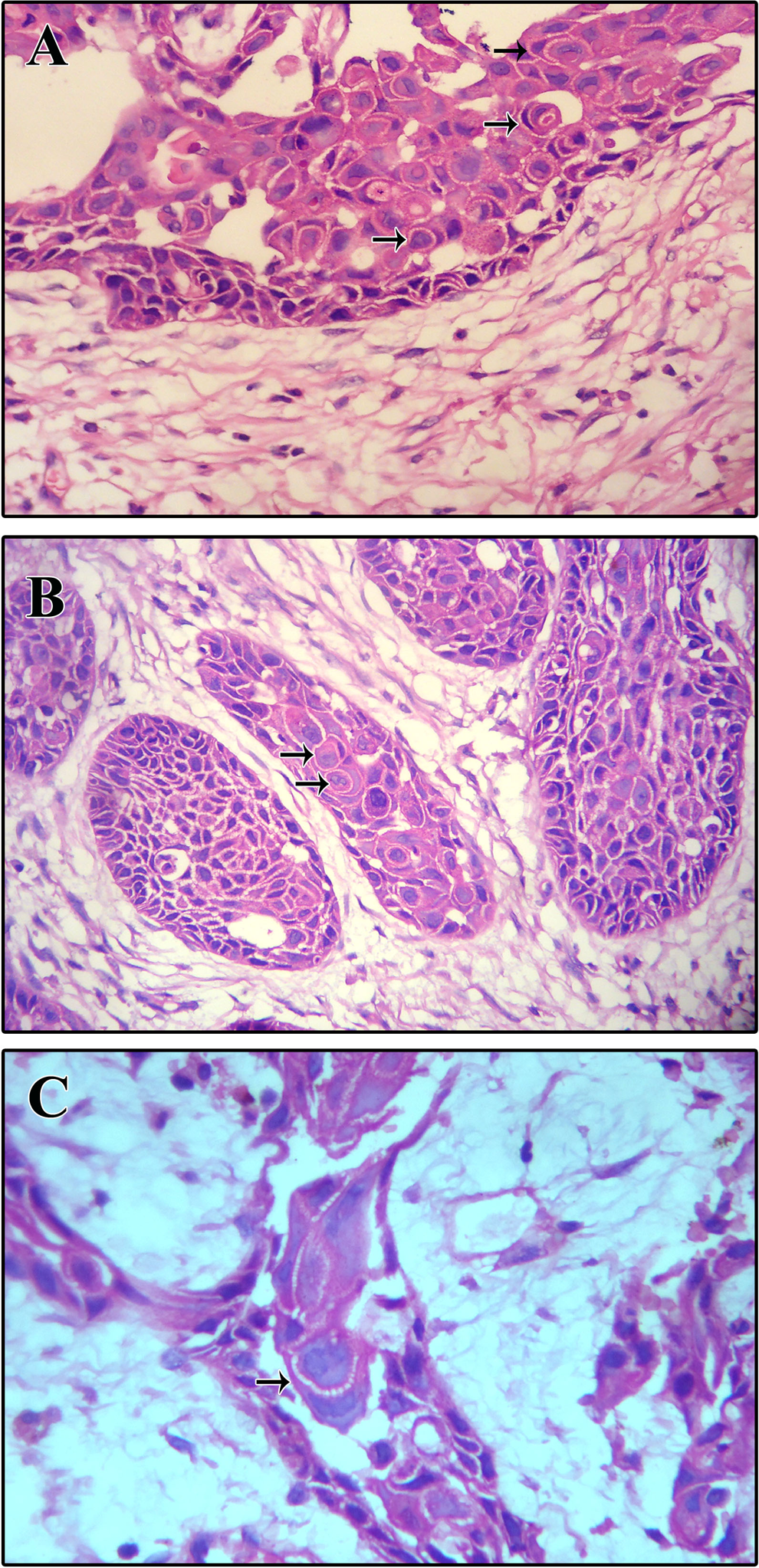
Photomicrograph showing mild (A), moderate (B), and severe (C) grades of connective tissue degeneration. The cannibalism is shown by black arrow. (Hematoxylin and eosin stain; original magnification ×400).
Immunohistochemistry
The expression of CD68 and lysozyme was localized to the cytoplasm of malignant cells (Figure 4(A) and (B)). Expressions were seen not only in endocytic cells but also in other tumor cells. All the cells showing positivity were included for grading the expression. CD68 staining in the epithelium of OSCC was present in 50 cases (89.28%; weak: 47 (94%) and strong: 3 (6%)). Similarly, lysozyme expression was present in 47 cases (83.92%; weak: 45 (95.74%) and strong: 2 (4.25%)).

Immunohistochemical expression of CD68 (A) and lysozyme (B) in tumor cells of OSCC (original magnification ×400). CD68: cluster of differentiation 68; OSCC: oral squamous cell carcinoma.
Statistically significant differences were observed in CD68 expression of TMN stage (F = 4.653, p = 0.049), histopathological grades (F = 5.294, p = 0.045), and stromal degeneration (F = 5.978, p = 0.024). However, results for sex (F = 1.926, p = 0.449), age (F = 1.161, p = 0.63), T status (F = 3.928, p = 0.10), N status (F = 3.00, p = 0.24), M status (F = 3.02, p = 1.00), and number of EK (F = 5.008, p = 0.08) were statistically insignificant. Likewise, for lysozyme expression, the results were statistically significant in histopathological grades (F = 9.182, p = 0.004) and number of EK (F = 8.861, p = 0.0119). However, results for sex, age (F = 3.354, p = 0.179), T status (F = 1.406, p = 0.72), N status (F = 2.759, p = 0.231), M status (F = 2.177, p = 1.00), TNM stage (F = 3.797, p = 0.17), and stromal degeneration (F = 4.233, p = 0.115) were statistically insignificant (Table 2).
CD68 and lysozyme expression in different parameters of OSCC.
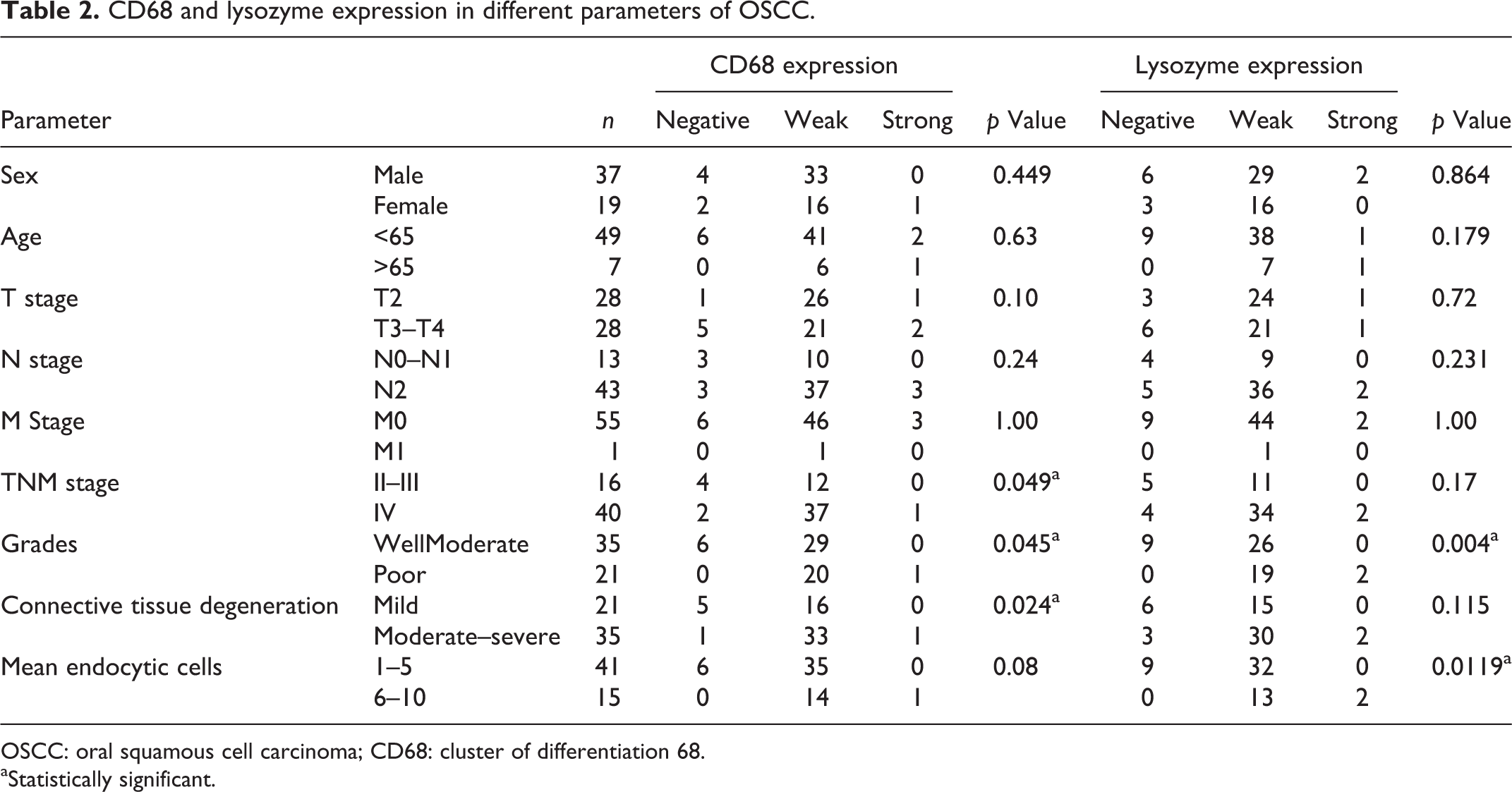
OSCC: oral squamous cell carcinoma; CD68: cluster of differentiation 68.
aStatistically significant.
Discussion
Various methodologies have been used for grading EK in various tumors. Especially in OSCC, Jose et al. 13 graded cellularity of EK as grade I: <5 cells, grade II: 6–15 cells, and grade III: >16 cells. In our recent study on central and peripheral giant cell granulomas, hundred giant cells were examined in each section and the number of endocytic giant cells was expressed in percentage. Fernandez-Flores 14 studied 66 cases of giant cell tumor of the tendon sheath (localized type) and graded giant cell endocytosis on a scale from 0 to 4 based on the percentage of giant cells showing endocytosis (0: no evidence; 1: <10%; 2: 10 to <25%; 3: 25 to 90%; 4: >90%). However, in the present study, four hot spots were selected per slide and the number of endocytic cells was counted. The final value was expressed as mean EK per HPF. The EK ranged from 1 to 10 with mean of 4.125 ± 2.107. The phenomenon of complex endocytosis was observed in 9 (16.07%) cases. Jose et al. 13 reported very few suspicious-looking cells with bizarre pattern of endocytosis.
One more unusual aspect reported in the present study is mitotic activity in the internalized cells (two cases). But this phenomenon was reported in partial endocytosis suggesting engulfment of mitotically dividing adjacent tumor cell. This feature possibly demonstrates that endocytic cell does not differentiate between normal cells and mitotically dividing cells when there is scarcity of nutrition in the tumor cells. Such feature has never been reported in the literature and further studies are needed to explore the significance of such behavior.
Of 56 cases of OSCC, 8 (14.28%) displayed endocytosis of neutrophils (mean: 5.875 ± 0.99; Figure 1(E)). The largest published series till date reported 11 fine needle aspiration cases with tumor cells showing endocytosis of neutrophils. 14 This series included carcinomas arising from gallbladder, small intestine, pancreas, breast, larynx, lung, and disseminated tumor of unknown origin. Two cases in this series were non-Hodgkin lymphomas. The phenomenon of endocytosis of neutrophils has also been documented by the light microscopy in pleomorphic (giant) cell carcinomas of lung, gall bladder, pancreas, and intestine. 15 –19 Caruso et al. 20 reported electron microscopic features of endocytosis of neutrophils, which showed the characteristic equipment of discrete primary and secondary granules, glycogen, and lipid bodies. Neutrophils were present within vacuoles of adenocarcinoma cells and showed various phases of apoptotic changes. Recently, Barresi et al. 21 reported five cases of gastric cancer with micropapillae showing infiltration by neutrophils. Hematoxylin and eosin staining, terminal deoxynucleotidyl transferase deoxyuridine triphosphate nick-end labeling (TUNEL) assay, and immunostaining for caspase-3 demonstrated apoptotic neutrophils within cytoplasmic vacuoles of tumor cells.
Also in the present study, lymphocyte (Figure 1(D)) and RBC engulfed by tumor cells was reported in three cases each. Lugini et al. 5 reported T lymphocyte endocytosis by metastatic melanoma cells. Morphologic analyses, including time-lapse cinematography and electron microscopy, revealed a sequence of events, in which metastatic melanoma cells were able to engulf and digest live autologous melanoma-specific CD8+ T cells. The mechanism underlying lymphocyte endocytosis involved a complex framework, including lysosomal protease, cathepsin B activity, caveolae formation, and ezrin cytoskeleton integrity and function.
In the present study, although the mean EK was more in stage IV as compared to stage III, the difference was statistically insignificant. Jose et al. 13 reported majority of cases of grade III cancer endocytosis (>16 cells) in stage IV of OSCC. We believe that increase in stage or size increases the tumor load and thus increases the requirement of nutrition. Thus, lack of nutrition in advanced stages due to increased tumor load might be responsible for increased endocytic activity in the tumor cells. Analogously, in the present study the expression of CD68 was found to be increased in advanced stages of OSCC. However, the difference in the expression of lysozyme in different TNM stages of OSCC was statistically insignificant.
Another major determinant of the prognosis of OSCC is the presence and extent of lymphatic invasion, 22 which is pursued by increased probability for metastatic growth. 23 In the research carried out by Jose et al., 13 all the positive lymph node cases were found to have higher grades of endocytosis (>16 cells) with statistically significant results. However, in the present study, mean EK was found to be increased from N0–N1 stage to N2 stage of OSCC, but the results were statistically insignificant.
Several authors have emphasized that the number of EK can be correlated with the aggressive and metastatic behavior in systemic malignancies. 1 –5 Moreover, Towers and Melamed 1 have stated that increased number of EK may be useful in grading of breast carcinoma. OSCC consists of a diverse cell population with probable differences in invasiveness and metastasis behavior. Hence, clinical behavior depends on whether a tumor consists of highly aggressive cells or not. In the present study, differences in the mean EK for well versus moderately, moderately versus poorly, and well versus poorly differentiated OSCC were statistically significant. However, Jose et al. 13 did not report statistically significant correlation of cell endocytosis with the histopathological grades. The results of the present study signify that poorer the differentiation in cancer cells more is the EK. The poorly differentiated OSCC is more aggressive with high proliferative rate. We believe that nutritional supply to the tumor cells is not in pace with the high proliferation-related tumor load. This caused increase in nutritional demand in tumor mass, which could probably initiate endocytosis in tumor cells. Correspondingly, CD68 and lysozyme expression in the tumor cells was also found to be increased with the increasing grades of OSCC. Hence, expression of CD68 in tumor cells of OSCC can be used as a prognostic marker. However, future studies on increased sample sized with follow-up data are needed to validate this finding.
The tumor cells receive nutrition from vascular supply present in the stroma. Stromal degeneration is a well-known phenomenon in aggressive neoplasms, which could possibly hamper the nutritional supply to the tumor cells. Thus, we hypothesized that there could be possible association between stromal degeneration and the number of EK. In the present study, stromal degeneration was classified into mild, moderate, and severe. (Figure 3) The differences in mean EK between these three groups were found to be statistically significant. These findings confirm the association of EK with the stromal degeneration and thus the nutrition. In the present study, it is also reported that with increasing grades of stromal degeneration, the CD68 expression increases in the tumor cells of OSCC. Such correlation has never been reported in the literature till date.
To study the association between mean endocytic cells and expression of phagocytic markers (CD68 and lysozyme), the cells were categorized into two groups, namely, 1–5 mean endocytic cells per HPF and 6–10 mean endocytic cells per HPF. It is observed that as the endocytic activity increases, the expression of lysozyme and CD68 also increases in the tumor cells (p = 0.0119 and 0.08, respectively). However, the results were statistically significant only for the lysozyme expression. These results also propose that the degradation of internalized cell is mainly mediated by lysozyme.
In the present study, three cases of acantholytic/adenoid OSCC displayed maximum mean EK (Figure 1(C)). Endocytosis was reported mainly in the acantholytic tumor cells lying in the pseudolumen. We believe that the nutritional supply to acantholytic cells gets cut off because of the loss of cell-to-cell contact and hence possibility of these cells showing endocytosis increases. Future studies on evaluation of EK in acantholytic/adenoid OSCC are needed to validate our findings.
Expression of CD68 antibody has been reported in tumor cells of various malignancies, such as breast carcinoma, prostatic carcinoma, renal cell carcinoma, melanoma, endometriosis, and even different soft tissue sarcomas. 24 –28 Doussis et al. 25 found CD68 expression in cytological specimens of adenocarcinoma and poorly differentiated carcinomas with KP-1 clone giving strong positive results. In the aforementioned malignancies, CD68 expression has been regarded as diagnostic and prognostic marker. The expression of CD68 and lysozyme has never been reported in the tumor cells of OSCC. In the present study, the expression of CD68 and lysozyme was reported not only in endocytic cells but also in tumor cells without morphological evidence of EK. We propose that such tumor cells showing expression of CD68 and lysozyme could represent the potential cells, which in future can transform into endocytic cells. Thus, in future, such markers can be used for early detection of potential endocytic cells in tumor mass.
In the present study, internalized cell showed signs of degradation on histopathological examination. Positive expression of CD68 and lysozyme markers suggests lysozyme-mediated degradation of internalized cell. However, possibility of programed cell death in internalized cell cannot be ruled out based on the results of the present study. Hence, to further explore the fate of internalized cell, it is important to study apoptotic markers like caspases and TUNEL assay in OSCC cases showing EK.
Conclusion
The findings of the present study suggest that the mean endocytic cells in OSCC increase with increasing histopathological grades and TNM stages. Moreover, their association and correlation with stromal degeneration grade supports the ‘lack of nutrition’ theory of EK in OSCC. The expression of phagocytic markers (CD68 and lysozyme) has never been reported in the literature. Expression of these markers can be used for histopathological grading of OSCC. Moreover, their expression in non-endocytic tumor cells could help in identifying tumor cell populations having potential endocytic behavior. To further explore EK phenomenon in OSCC, we recommend future studies on markers like caveolin-1, actin, ezrin, cathepsin B, nine transmembrane segment, vimentin, Rho-ROCK–actin/myosin pathway, and so on. Since EK is associated with poor nutritional supply, future studies on angiogenesis and hypoxia-induced factors in the context of endocytosis in OSCC will unveil new facets. The possibility to interfere with endocytic behavior could represent a new perspective in pharmacological control of cancer progression.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.