
Abstract
Diabetes mellitus presents global health challenges, thereby increasing the need for person-centred care. This cross-sectional study of 157 diabetes specialist nurses evaluated the theoretical structure of the Swedish version of the Learning potential of the workplace scale and explored whether the learning potential of the workplace, work engagement, quantitative demands, influence, stress and work experience in diabetes care were associated with nurses’ perceptions of person-centred care. Regression analysis showed that the variables “opportunity to reflect”, “support in learning’, “work engagement” and “work experience in diabetes care” were positively associated with perceived person-centred care. Perceived organisational and environmental support for person-centred care was positively linked to “opportunity to reflect”, “support in learning” and “influence” and negatively to “stress” and “quantitative demands”. Reporting followed the STROBE guidelines. The findings demonstrated that healthcare systems can enhance nurses’ ability to provide person-centred care for persons with diabetes by fostering learning-oriented workplaces and addressing organisational challenges.
Keywords
Introduction
Diabetes mellitus is a complex, chronic metabolic disorder with significant global health effects, affecting a large population and imposing substantial burdens on healthcare systems. 1 The global burden of diabetes has grown significantly in recent decades, with incidence rates continuing to increase. This trend has placed increased pressure on individuals and healthcare systems worldwide. Because diabetes is a major cause of death, this development highlights the urgent need for ongoing diabetes awareness and prevention efforts to help reduce the growing impact of diabetes. 2 As global health demands increase, the nursing role needs to evolve to meet challenges. Nurse-led care models, designed to improve healthcare access and manage the growing demand for chronic diseases, such as diabetes, are increasingly necessary, 3 even in Sweden.
In Sweden, diabetes healthcare is decentralised. Patients with type 2 diabetes are enrolled at primary healthcare centres. By contrast, patients with type 1 diabetes are enrolled in specialised diabetes-care clinics at hospitals. Both units typically comprise a diabetes team, which involves diabetes specialist nurses (DSNs), physicians and other professionals, such as dietitians and foot-care specialists.4,5 To minimise variation in care provision, the Swedish government has established national guidelines for chronic diagnoses such as diabetes,4,5 as well as the National Diabetes Register, which maintains a record of diagnoses, treatments and metabolic outcomes for individuals with diabetes. 6 In Sweden, DSNs are registered nurses who hold advanced competencies in diabetes care and whose clinical responsibilities align with international, national and regional guidelines for the management and prevention of diabetes.4,7–9
A review by Lawler et al. 10 shows that DSNs play a crucial role in educating patients to promote diabetes management and quality of life, thereby fostering patient confidence in self-care management and sustaining healthcare benefits, such as delaying complications, as well as reducing hospitalisation and readmission. Additionally, a review by Zhu et al. 11 demonstrates that DSNs contribute to enhanced healthcare practices by improving clinical outcomes, reducing hospital stays and minimising complications. Zhu et al. 11 further describe that DSNs play a significant role in inpatient care by following the patient from admission to discharge at homecare and reducing inpatient harm. Also, in outpatient settings, they provide continuity of care. Additionally, DSNs are essential in paediatric diabetes care because they educate children and their families about diabetes care. DSNs further educate patients on the risks of diabetic foot ulcers, support those with gestational diabetes during maternal care and prescribe diabetes management aids. 11
DSNs describe their professional role as multifaceted, with complex responsibilities and challenges, 12 including potential conflicts arising from high quantitative, decision-making and learning demands. 13 Rapid technological advancements have also altered working conditions, contributing to increased workload pressure, as reported by nurses in primary healthcare. DSNs note that professional development is supported by education, ongoing professional learning, a collaborative healthcare team, networking with other DSNs, and strong leadership. 14 According to a review article, 15 professional development can occur through methods beyond external courses. It can also happen through reflection on assignments during work or through consultation with colleagues when needed. A workplace designed as a learning environment maximises opportunities for learning through professional experiences, such as activities and interactions. 16 This process is known as work-integrated learning, where professionals engage in continuous learning during their daily work. Any learning that is an integrated part of work is considered a work-integrated learning opportunity. 17
Person-centred care (PCC) is a humanistic approach that has been confirmed to enhance healthcare, education and patient collaboration. Through shared decision-making, it acknowledges patients as experts based on their perspectives and/or experiences. 18 Working with patients in a person-centred manner places new demands on health professionals, requiring skills such as listening, communication, negotiation and the ability to respond flexibly to each patient's unique needs. 19 A recent study 20 highlights that persons living with diabetes express a preference for multidimensional learning and person-centred care tailored to their capabilities and needs. While they value the opportunity to explore self-directed online resources for health improvement, they continue to hold DSNs in high regard, particularly when these professionals apply their expertise through meaningful, health-promoting dialogue.
Nurses are aware that practices and patient care standards are constantly evolving in healthcare, necessitating ongoing professional development throughout their careers. However, nurses expressed disappointment that management do not view training and education as essential to improving patient care because they did not allocate sufficient time for learning activities. 16 Similarly, barriers to implementing PCC became more complex under time constraints because professionals needed to learn new communication techniques and make time for PCC during their workday. This is problematic because professional education and training are key enablers for the effective application of PCC. 21 The present study aimed to 1) evaluate the theoretical structure of the Swedish version of the Learning potential of the workplace scale and 2) explore whether the learning potential of the workplace, work engagement, quantitative demands, influence, stress and work experience in diabetes care are associated with perceived person-centred care among diabetes specialist nurses.
Methods
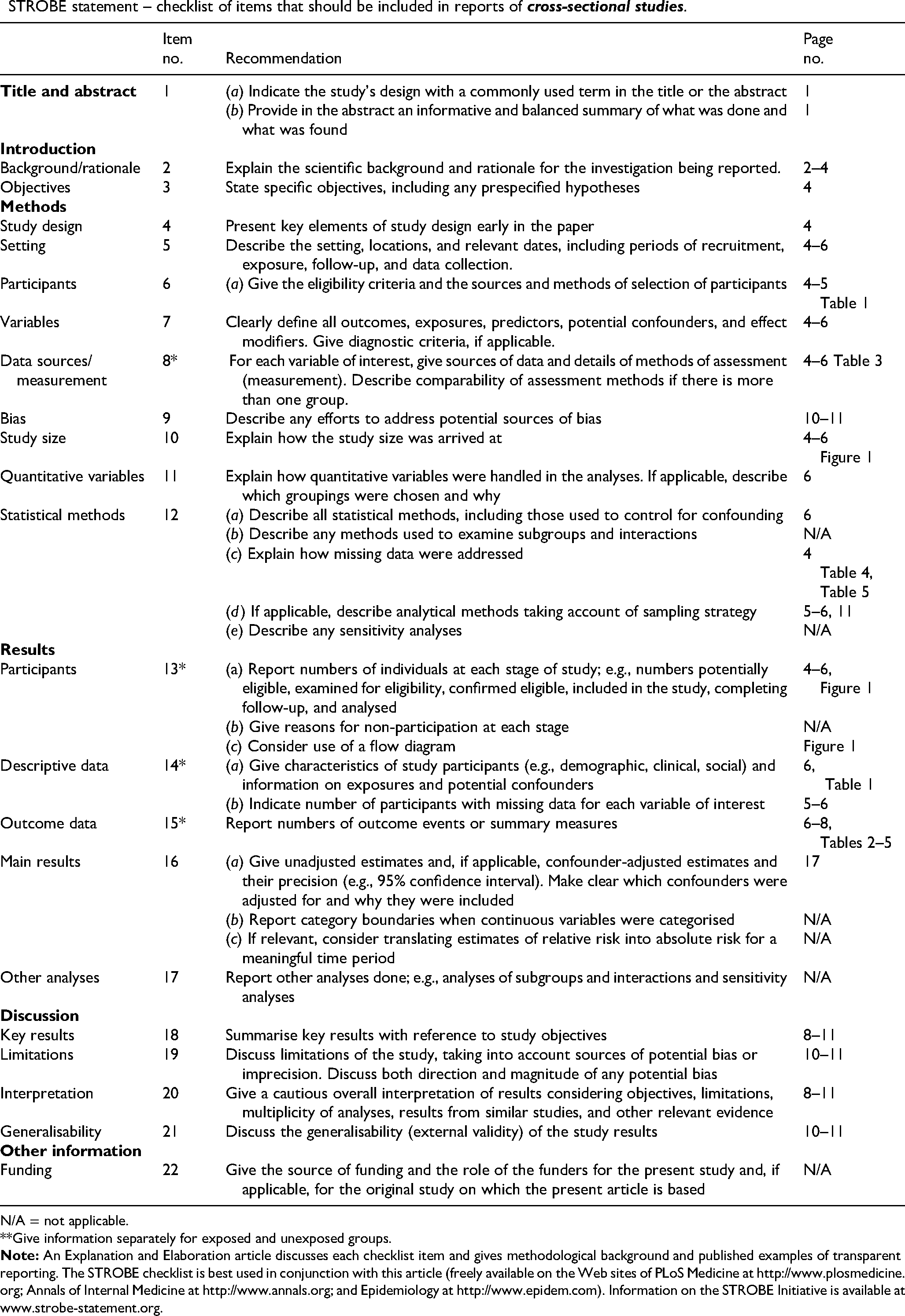
This study employed a cross-sectional quantitative design, adhering to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 22 (Appendix 1).
Participants and procedure
The study participants were recruited from the membership register of the Swedish Association for Nurses in Diabetes Care. The association distributed the study information and online survey link to all members nationwide and handled all contact with potential respondents (N = 560). The inclusion criteria were membership in the association and regular interaction with persons with diabetes in everyday work.
Questionaries
The Person-Centred Care Assessment Tool (P-CAT) was utilised to determine the perceived level of person-centred care. 23 The tool consists of 13 statements, divided into two subscales: Extent of Personalising Care (EPC) and Organisational and Environmental Support (OES).
These subscales capture the extent to which staff rate the care provided as person-centred.23–25 The EPC subscale, comprising items 1–7, 12 and 13 and the OES subscale, consisting of items 8–11, demonstrated good internal consistency, with Cronbach's alpha (α) values of 0.81 and 0.82, respectively. 23 Items 8–11 were negatively worded and were therefore reverse-coded before analysis. Participants responded to a five-point Likert scale, ranging from (1) “completely disagree” to (5) “strongly agree”.
The Learning Potential of the Workplace (LPW), a multidimensional instrument, consists of 12 items formulated as statements that measure the learning potential of the workplace, with three items per subscale across four dimensions. These dimensions include “ Learning through Reflection” (α = 0.91), “Learning through Experimentation” (α = 0.90), “Learning from Colleagues” (α = 0.83) and “Learning from Supervisor” (α = 0.90), all indicating high internal consistency. 26 After obtaining permission from the original developers, the instrument was translated, and the content of the items was minimally adapted for the Swedish healthcare context. A forward and backwards translation method, with forward translation by a bilingual panel of authors and backwards translation by an authorised translator, was used. The final Swedish version was pre-tested on a smaller group of DSNs (not included in the present sample) to ensure clarity and cultural appropriateness, confirming that the instrument was easy to understand and use.27,28 Participants responded to a five-point Likert scale ranging from (1) “not applicable” to (5) “completely applicable”.
The Copenhagen Psychosocial Questionnaire (COPSOQ III) assessed multiple aspects of the organisational and social environment in the workplace. 29 The three selected dimensions used in the study were Work Engagement (α = 0.84), comprising three items; Quantitative Demands (α = 0.85), comprising three items; and Influence (α = .75), comprising four items, all indicating good internal consistency. Participants responded to a five-point Likert-type scale ranging from (100) “Always” to (0) “Never/hardly ever”.
A single-item measure of stress symptoms was used to measure stress. 30 Participants responded to the question: “Stress refers to a situation in which a person feels tense, restless, nervous, or anxious, or is unable to sleep at night because of his or her mind is troubled all the time. Are you currently experiencing such stress?” Participants responded to a Likert scale ranging from (1) “not at all” to (5) “very much”.
Data collection
Data were collected nationwide through an online questionnaire distributed via email by the Swedish Diabetes Nurses’ Interest Association to all their members between May and July 2023. The association sent an initial invitation followed by two reminders with the online questionnaire link to a total of 560 potential respondents, which resulted in 157 completed responses, comprising a response rate of 28%. To ensure that each participant submitted only one response, email verification was required for access to the questionnaire. No duplicate or missing data were recorded. Email addresses were treated as personal data, coded using unique identifiers and stored separately from the survey responses to maintain confidentiality. The sampling procedure conformed to the recommendations for designing online survey studies 31 and details are illustrated in Figure 1.

Flowchart illustrating the sampling procedure.
Data analysis
The Statistical Package for the Social Sciences, version 29.0 for Windows (IBM Corp., Armonk, NY, USA), was used for data analysis. The demographic characteristics of the participants were described using descriptive statistics, including means, standard deviations, skewness, frequencies, percentages and 95% confidence intervals (CI). Exploratory factor analysis was performed to identify the factor structure of the Swedish version of the LPW scale. First, the Kaiser-Meyer-Olkin coefficient (≥ 0.8) was calculated to ensure that exploratory factor analysis was applicable. The analysis included principal component analysis, varimax rotation, eigenvalue assessment, scree plot analysis, factor loading evaluation and Bartlett's test of sphericity. 32 Cronbach´s alpha coefficient was used to explore the reliability of all scales. The study examined the zero-order correlations between variables using Spearman's rho correlation. Two multiple linear regression models were utilised to analyse the associations between the perceived level of person-centred care and learning potential of the workplace, controlling for the organisational and social environment at the workplace, stress symptoms and nurses’ years of work experience in diabetes care. The statistical significance level was 5% (P < 0.05). The multicollinearity in the regression models was checked using the variance inflation factor (VIF). VIF values < 5 confirm low multicollinearity among the predictors 33 (VIF = 1.06−2.38).
Ethical considerations
The Swedish Ethical Review Authority approved the study (Dnr 2023-00920-01), which adhered to the Helsinki Declaration of Medical Research Ethics and Standards. 7 All participants received detailed cover letters that informed them about the project and provided the researchers’ contact details. It was emphasised that participation was voluntary and that completion of the questionnaire was considered informed consent for voluntary participation in the study.
Results
The demographic characteristics of the 157 participants are presented in Table 1. The participants were primarily female, with an average age of 51 years (SD = 9.41) and an average of 12.66 years (SD = 9.2) of work experience in diabetes care.
Characteristics (n = 157).

Most participants (98.73%) expressed a positive attitude towards patients with diabetes seeking advice online; however, only 24.8% informed patients about supportive health websites, while 15.9% reported that they rarely or never did so. DSNs reported conducting digital healthcare visits at varying frequencies, with a mean of 9.14 visits per month; however, the data were highly skewed (skewness = 4.7) with high dispersion (SD = 22.2), and 35.7% (n = 56) never conducted any visits. The estimated impact of increased digitalisation on healthcare workload was as follows: 52.9% (n = 83) reported that their workload remained unchanged, while 30.6% (n = 48) experienced an increase and 16.6% (n = 26) experienced a decrease.
Exploratory factor analysis
The Bartlett's sphericity test was significant (χ2= 1135.344; P ≤ 0.001), and a KMO value of 0.842 was obtained. In this study, using principal component analysis, three common factors were extracted (eigenvalues > 1) from a 12-item questionnaire, with a cumulative contribution of 70.63%. Factor 1, which included four item (explained variance = 47,42%), was labelled “Opportunity to Reflect”; Factor 2, which included six items (explained variance = 13,78%), was labelled “Support in Learning”; Factor 3, which included two items (explained variance = 9,43%), was labelled “Time for Exploration” (Table 2).
Exploratory factor analysis of the Swedish version of the learning potential of the workplace instrument.

The Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalisation. Factor loadings above 0.30 are shown and indicated in bold for factors with the highest loadings.
LPW = Learning Potential of the Workplace.
Correlations and multiple regression models
Table 3 presents the mean scores, standard deviations, CI and Cronbach´s alpha values for all the instruments used in analyses. P-CAT’s two subscales, EPC and OES, which we have interpreted, possess theoretically different orientations. The EPC includes items in the P-CAT tool related to professionals’ performance and desire to provide person-centred care, while the OES addresses organisational obstacles that may hinder person-centred care. For this reason, the global score was not used in the present study. Separate analyses were conducted with EPC and OES as outcome variables to explore these differences.
Descriptive data and Cronbach's alpha of dimensions/subscales in the used instruments.

CI = confidence interval; P-CAT = Person-Centred Care Assessment Tool; EPC = Extent of Personalising Care; OES = Organisational and Environmental Support; LPW = Learning Potential of the Workplace.
The correlation analyses revealed that EPC was positively associated with all subscales of LPW (P ≤ 0.001), work engagement and influence (P ≤ 0.001) and work experience in diabetes care (P = 0.002), while being negatively associated with stress symptoms (P = 0.011) and quantitative demands (P ≤ 0.001). Further, OES was positively associated with all subscales of LPW, work engagement and influence (all P ≤ 0.001), and negatively associated with stress symptoms and quantitative demands (P ≤ 0.001) (Table 4).
The correlation between the studied variables.
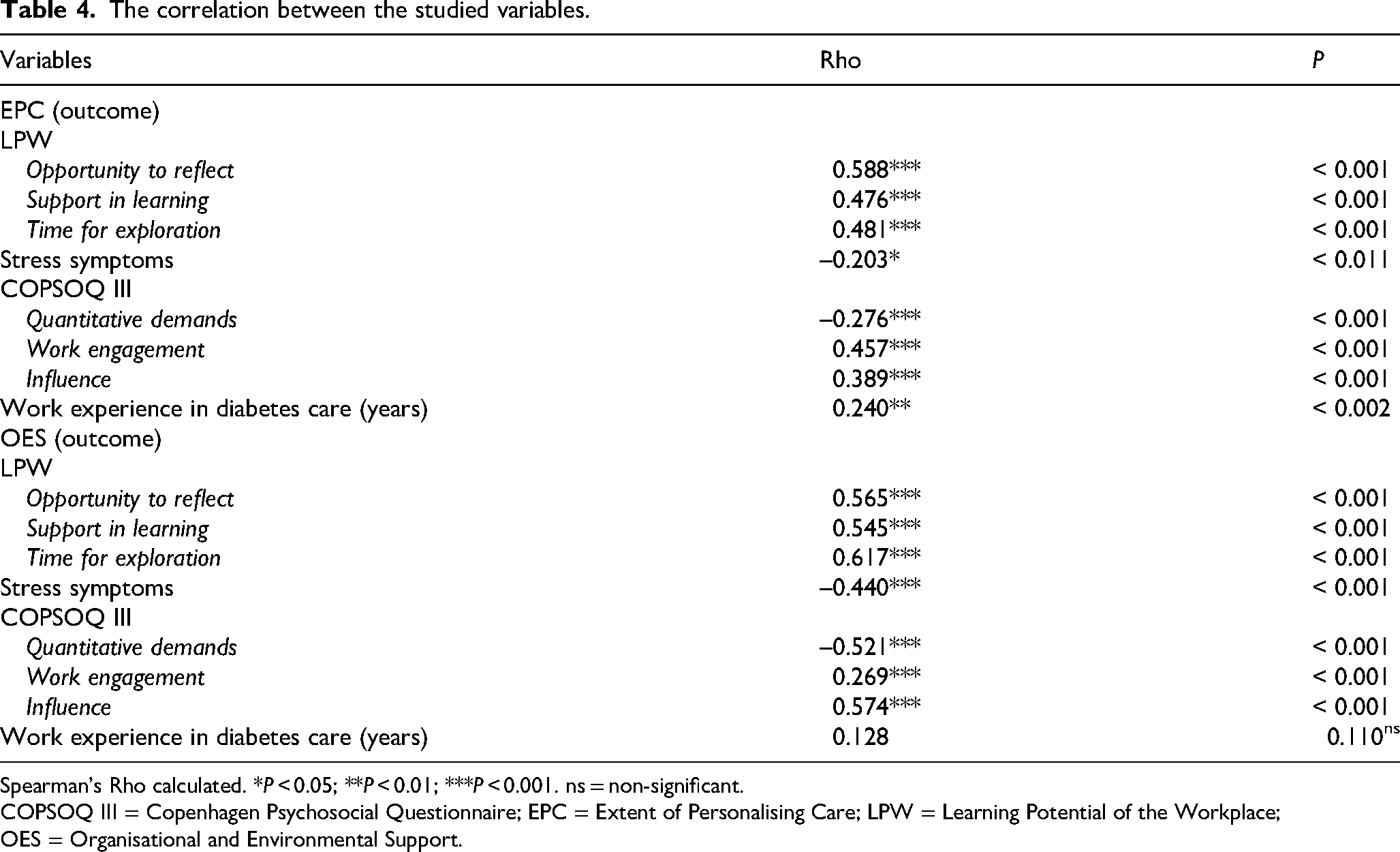
Spearman's Rho calculated. *P < 0.05; **P < 0.01; ***P < 0.001. ns = non-significant.
COPSOQ III = Copenhagen Psychosocial Questionnaire; EPC = Extent of Personalising Care; LPW = Learning Potential of the Workplace; OES = Organisational and Environmental Support.
All independent variables significantly correlated with the criterion variables (EPC and OES) were included and tested using two separate multiple regression models. The first multiple regression model showed that the opportunity to reflect, support in learning and work engagement (all P ≤ 0.001), as well as work experience in diabetes care (P = 0.033), were all positively associated with the DSNs’ perceived person-centred care. The model explained 50% of the variance in EPC (Table 5).
The multiple regression models associated with EPC and OES.
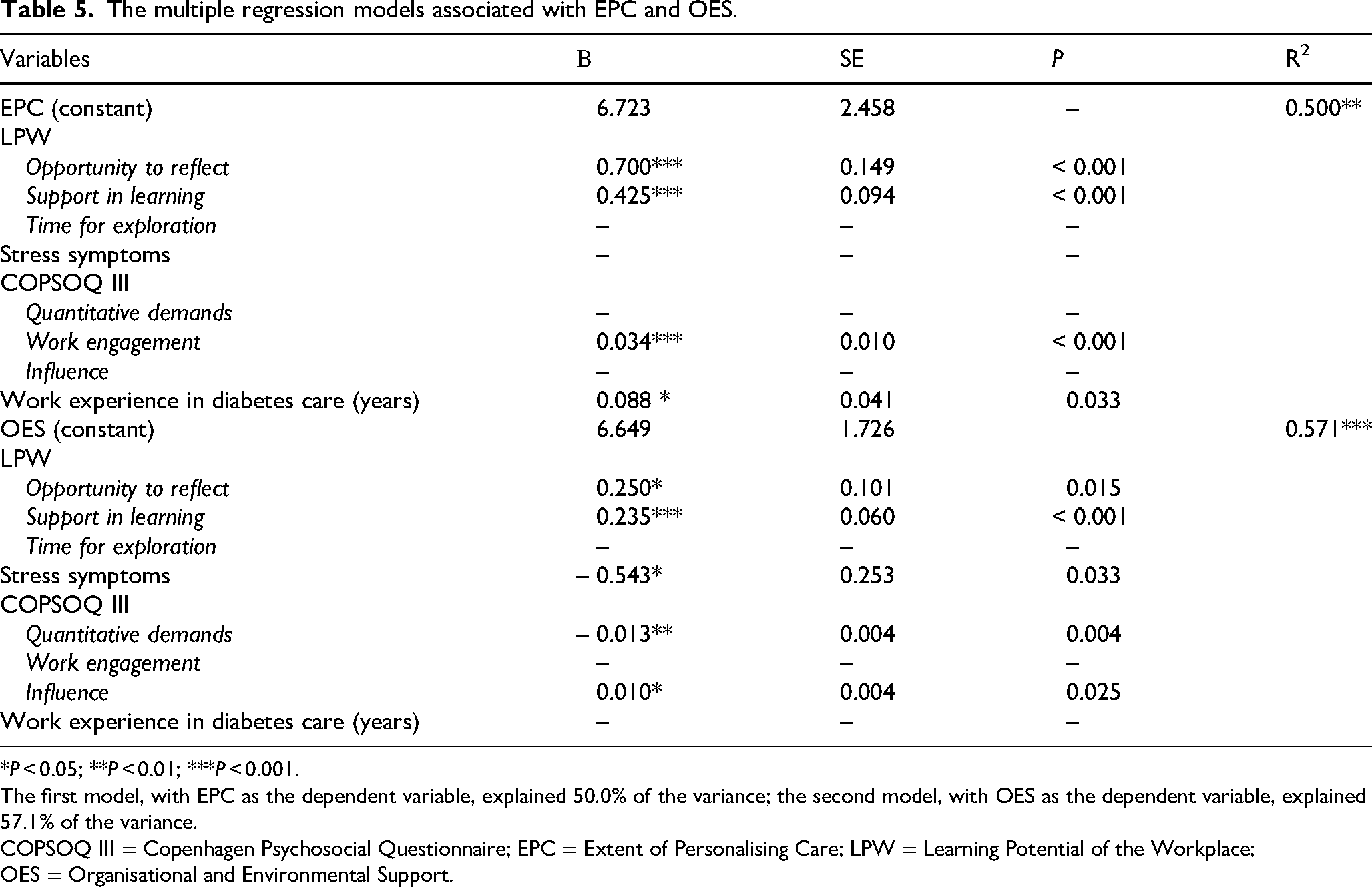
*P < 0.05; **P < 0.01; ***P < 0.001.
The first model, with EPC as the dependent variable, explained 50.0% of the variance; the second model, with OES as the dependent variable, explained 57.1% of the variance.
COPSOQ III = Copenhagen Psychosocial Questionnaire; EPC = Extent of Personalising Care; LPW = Learning Potential of the Workplace; OES = Organisational and Environmental Support.
The second multiple regression model, which included the opportunity to reflect (P = 0.015), support in learning (P ≤ 0.001) and influence (P ≤ 0.025), was positively associated with DSNs’ perceived organisational and environmental support for PCC. On the other hand, stress symptoms (P = 0.033) and quantitative demands (P = 0.004) were negatively associated with DNSs’ perceived organisational and environmental support for PCC. The model explained 57.1% of the variance in OES (Table 5).
Discussion
The present study began with the translation and evaluation of the LPW instrument, which measures the learning potential of the workplace. Through the evaluation, we found that the Swedish version of the LPW scale exhibited a three-factor structure, a deviation from the original four-factor model. 26 This three-factor structure explained 70.63% of the total variance, indicating that the model is reliable for understanding the underlying constructs in the Swedish healthcare context. We believe that the difference in factor structure may be attributed to variations in the occupational groups studied and cultural or linguistic differences in the workplace. The original instrument includes items that emphasise learning from superiors, but this is less relevant in Swedish diabetes care, where DSNs often work autonomously 13 and take on the coordination of diabetes care in specific diabetes care units 12 without having access to a supervisor with particular knowledge in diabetes care. Therefore, we modified the wording of these items to “supervisor and/or work manager”. The DSNs described their professional role as multifaceted, with challenges such as role ambiguity, feelings of being uninformed, fragmented, resigned and time-pressured. 12 The multifaceted and challenging nature of the role is characterised by demands for autonomy in planning, confident decision-making, and the flexibility to adapt to different situations, requiring problem-solving abilities. 14
In the present study, we found that perceived person-centred care, as measured by the EPC subscale, was positively associated with the learning dimensions measured by LPW: “Opportunity to Reflect” and “Support in Learning”. These findings imply that DSNs’ work-integrated learning activities, such as interactions with colleagues and or supervisors/work managers, may be equally important in perceived person-centred care at their workplaces. This result aligns with previous research, which found that teamwork and workplace leaders serving as role models are essential for initiating work practices that support PCC implementation in workplaces. 21 This underscores the important role of a supportive learning environment in encouraging ongoing professional development.15,16 Lunden et al. 34 suggest that knowledge management is facilitated by an organisational culture that promotes continuous learning, information sharing and constructive feedback. Therefore, workplaces should commit to fostering a positive work-integrated learning environment to facilitate professional development and person-centred care.
EPC was also positively associated with years of work experience in diabetes care and work engagement. DSNs in our study had a mean of 12.6 years (SD = 9,2) of work experience in diabetes care. Aungsuroch et al. 35 reviewed the literature and found that work engagement was positively associated with years of work experience, performance, positive emotions and health across diverse healthcare settings.
This study also found that OES was positively associated with “Opportunity to Reflect”, “Support in Learning” and influence at work. These findings indicate that reflection and supportive work environments play an essential role in both learning and person-centred care. Sjögren et al. 36 confirmed that in residential care, staff perceptions of the psychosocial climate as supportive were strongly linked to their perceptions of the care provided as person-centred. Conversely, job strain and stress of conscience were negatively associated with, and may inhibit, person-centred care. Additionally, our study identified stress and quantitative demands as negative predictors of OES. The study findings indicate that workplaces should strive for a work environment where employees experience a balance between work demands and work control, thereby perceiving organisational and environmental support for delivering person-centred care. Another study found that DSNs raised concerns about limited access to learning and professional development, as well as the impact of workload on patient care and safety. 10 Another type of workload described by primary healthcare nurses was the increased digitalisation in healthcare, which was viewed as beneficial but more demanding. 37 However, in our study, just over half of the participants (52.9%) reported that their workload remained unchanged due to increased digitalisation in healthcare. In comparison, about one-third (30.6%) reported an increase in workload, and the remaining participants (16.6%) reported a decrease. Additionally, most DSNs were positive about patients using online services to obtain health information related to diabetes when needed; however, only a quarter (24.8%) reported guiding patients to reliable websites for this purpose. These findings are noteworthy and supported by a previous study, 20 which showed that patients often seek health-related diabetes information online but ask professionals to guide them to the most reliable websites.
PCC has increasingly been promoted as a recommended humanistic care model for the future, adopted worldwide by policymakers, researchers, nursing curricula and practitioners. 38 Our study's findings would be of interest to policymakers and stakeholders who want to create a work environment that promotes work-integrated learning for professionals. Such an approach could also enable the implementation of person-centred care.
Our study participants were DSNs from Sweden, most of whom had extensive work experience in diabetes care, and the majority held a master's degree. Findings from another study show that the work environment influences how nurses recognise their need for learning. 39 When experienced senior colleagues set the standards for learning, other nurses tend to follow, meaning that experienced nurses promote learning by serving as role models for less experienced colleagues. Highly educated and experienced nursing staff, such as the DSNs in current study, can promote a favourable environment for work-integrated learning and create conditions for job satisfaction, thereby sustaining the profession. Another study showed that professionals who rated PCC more highly were also less likely to consider leaving their current workplace. 23 By establishing an encouraging work environment that fosters DSNs’ work-integrated learning and person-centred care, high-quality diabetes care can be ensured.
Methodological considerations
A cross-sectional study design was applied to identify relationships and control for confounding variables. One weakness of this analysis may be its limitation in terms of establishing causal inference. 40 Therefore, the study's contribution to the research field is the important associations between relevant variables; these associations could indicate causality, but, more importantly, they form the basis for further research.
A strength of the present this study lies in its focus on a specific group of nurses, DSNs, who play a crucial role in diabetes healthcare. The recruitment of participants through a national professional interest association may have benefited the representativeness of this population in terms of geographical distribution, regional affiliation and healthcare type. However, the response rate was low, despite following advice about attaining an appropriate response rate, including sending multiple reminders. 31 Although the generalisability of the results may be limited, the study identifies notable findings about DSNs’ workplace learning and person-centred care. Also, a part of the aim was to translate and validate the LPW scale in a Swedish diabetes-care context. The study's findings revealed that the scale can be a useful tool in research on the learning potential of the workplaces (i.e., an addition to self-reported learning surveys). 31
Conclusions
The present study highlights the crucial role of the learning potential of workplaces for DSNs’ perception of person-centred care in a diabetes-care context. The findings demonstrated that opportunity to reflect, support in learning, work engagement and professional experience in the field were positively associated with perceived person-centred care, while organisational and environmental factors, such as stress and high quantitative demands, acted as barriers. By fostering a learning-oriented workplace culture and addressing organisational challenges, healthcare systems can enhance DSNs’ ability to provide person-centred care for persons with diabetes.
Footnotes
Ethical approval
The Swedish Ethical Review Authority approved the study (Dnr 2023-00920-01), which adhered to the Helsinki Declaration of Medical Research Ethics and Standards7. All participants received detailed cover letters that informed them about the project and provided the researchers’ contact details. It was emphasised that participation was voluntary and that completion of the questionnaire was considered informed consent for voluntary participation in the study.
Author contributions
AD conducted this study under the supervision of UFL, SA and EB. All authors contributed to the concept and design of this study. AD collected the data. AD, UFL and EB carried out the data analysis. AD was responsible for drafting the manuscript. All authors revised the manuscript critically and evaluated the final manuscript submitted for publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Other identifying authors’ information
2FoU-centrum Skaraborg, Regionens hus, Stationsgatan 3, S-541 80 Skövde, Sweden
Appendix 1
STROBE statement – checklist of items that should be included in reports of
| Item no. | Recommendation | Page |
|
|---|---|---|---|
|
|
1 | (a) Indicate the study's design with a commonly used term in the title or the abstract | 1 |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | 1 | ||
|
|
|||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported. | 2–4 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 4 |
|
|
|||
| Study design | 4 | Present key elements of study design early in the paper | 4 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection. | 4–6 |
| Participants | 6 | (a) Give the eligibility criteria and the sources and methods of selection of participants | 4–5 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable. | 4–6 |
| Data sources/measurement | 8* | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group. | 4–6 Table 3 |
| Bias | 9 | Describe any efforts to address potential sources of bias | 10–11 |
| Study size | 10 | Explain how the study size was arrived at | 4–6 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 6 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 6 |
| (b) Describe any methods used to examine subgroups and interactions | N/A | ||
| (c) Explain how missing data were addressed | 4 |
||
| (d) If applicable, describe analytical methods taking account of sampling strategy | 5–6, 11 | ||
| (e) Describe any sensitivity analyses | N/A | ||
|
|
|||
| Participants | 13* | (a) Report numbers of individuals at each stage of study; e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | 4–6, |
| (b) Give reasons for non-participation at each stage | N/A | ||
| (c) Consider use of a flow diagram | Figure 1 | ||
| Descriptive data | 14* | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders | 6, |
| (b) Indicate number of participants with missing data for each variable of interest | 5–6 | ||
| Outcome data | 15* | Report numbers of outcome events or summary measures | 6–8, |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | 17 |
| (b) Report category boundaries when continuous variables were categorised | N/A | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | N/A | ||
| Other analyses | 17 | Report other analyses done; e.g., analyses of subgroups and interactions and sensitivity analyses | N/A |
|
|
|||
| Key results | 18 | Summarise key results with reference to study objectives | 8–11 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 10–11 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 8–11 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 10–11 |
|
|
|||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | N/A |
N/A = not applicable. **Give information separately for exposed and unexposed groups.