
Abstract
Adolescents with attention deficit hyperactivity disorder (ADHD) and a co-existing medical disorder face challenges because the two disorders interfere with each other in everyday life. To support adolescents’ management of co-existing ADHD and medical disorder, the Guided Self-Determination intervention was adapted to this group of adolescents. The aim was to evaluate the implementation outcomes (feasibility and acceptability) of the Guided Self-Determination intervention by investigating how adolescents and their parents used and perceived the intervention. The intervention consisted of five sessions with a nurse, and the participants completed reflection sheets prior to the sessions. Ten adolescents and 14 parents participated. Feasibility was evaluated based on registrations of the participants’ engagement in the intervention. Acceptability was evaluated through semi-structured interviews. The reporting of this study follows COREQ (i.e., Consolidated criteria for reporting qualitative research). The results showed that the parent session and adolescent sessions 1 and 2 were more feasible than adolescent sessions 3 and 4. Acceptability was described in three themes: (1) personal preferences for attending sessions; (2) reflection sheets as a turning point in conversations; and (3) being supported or challenged by the completion and content of the sheets. In conclusion, feasibility and acceptability is complex and depend on the participants’ use of the intervention.
Introduction
Adolescents with attention deficit hyperactivity disorder (ADHD) and a co-existing medical disorder (MD) face challenges because the two disorders interfere with each other in everyday life, creating a dual task that cannot be managed by dealing separately with the two. 1 The Guided Self-Determination intervention (GSD) was adapted to support adolescents with ADHD and a co-existing MD in managing the dual task, and to support their parents, who are often the most important allies in adolescents’ health management. 2 The intervention was evaluated in psychiatric and paediatric outpatient settings. 3 Evaluating implementation outcomes are imperative to support the translation of evidence into clinical practice;4,5 however, only a few GSD studies have done that. 6 Therefore, the present study evaluated the implementation outcomes (feasibility and acceptability) of the GSD–ADHD–MD intervention by investigating how adolescents and their parents used and perceived the intervention.
Background
GSD is an empowerment-based intervention in disease management,7,8 and originally developed for adults with type 1 diabetes.7,9,10 GSD has shown effect among adolescents with type 1 diabetes. GSD individual sessions improved adolescents’ motivation for diabetes self-management 11 and GSD group sessions enhanced adolescents’ glycaemic control. 12 Qualitative studies showed that the adolescents highlighted the reflection sheets and communication with nurses as helpful in their diabetes management.13,14 Although those studies did not systematically investigate implementation outcomes, findings from the group setting pointed toward challenges. Some adolescents needed parental help in group sessions and to fill out the reflection sheets because some sheets could be difficult to understand or time-consuming to complete. 14 Because complexity in an intervention is known to affect participants’ engagement 5 and interfere with the intended outcomes, 15 it is imperative to investigate implementation outcomes to understand how an intervention works in a particular population. In addition, adolescents with co-existing ADHD and MD differ from adolescents with diabetes because living with two disorders creates a dual task. 1 ADHD and MD are linked in everyday life, creating a dual task because changes in either ADHD or the MD can affect the management of the other condition. For example, limitations imposed on daily life by a MD can accentuate the behavioural symptoms of ADHD, while having ADHD can complicate the management of a MD. 1 Therefore, the results on GSD among adolescents with diabetes may not be transferable to adolescents with co-existing ADHD and MD. Thus, the latter is considered as a new population in GSD research.
When introducing an intervention in a new population, clinical and implementation outcomes must be evaluated.16,17 Clinical outcomes assess the intervention's effects, and implementation outcomes assess attributes such as feasibility and acceptability.5,18 We evaluated the clinical outcomes of the GSD–ADHD–MD intervention and found that the intervention seems able to improve adolescents’ management of co-existing ADHD and MD. 3 The present study evaluates the implementation outcomes of feasibility and acceptability.
Feasibility indicates whether the intervention will work in the intended setting. 5 Because failure to utilize or deliver the intervention as intended is likely to influence the intended outcomes, 15 assessing feasibility can help to account for success or failure. 5 For the present purposes, feasibility was defined as “the extent to which a new treatment, or an intervention, can be successfully used or carried out within a given agency or setting”. 5 Additionally, feasibility is often reflected in participation rates. 5
Acceptability refers to the perceptions of those delivering or receiving the intervention.5,19 Acceptability is likely to change with experience and can be evaluated before, during or after engagement in the intervention.5,19 Assessing acceptability can help to explain engagement; if an intervention is not considered acceptable, people are less likely to engage.5,19 For the present purposes, acceptability was defined as “the perception among implementation stakeholders that a given treatment, service, practice, or innovation is agreeable, palatable, or satisfactory”. 5 Acceptability should refer to stakeholders’ direct experiences of the intervention's various dimensions such as content, complexity or comfort. 5
The present study aimed to evaluate the implementation outcomes (feasibility and acceptability) of the GSD–ADHD–MD intervention by investigating how adolescents and their parents used and perceived the intervention.
Methods
This study is part of an evaluation of the GSD–ADHD–MD intervention (Figure 1). Clinical outcomes were evaluated in a mixed methods study. 3 This study evaluated implementation outcomes (feasibility and acceptability) using registrations and semi-structured interviews and is reported in accordance with consolidated criteria for reporting qualitative research 20 (see supplementary material, File S1).
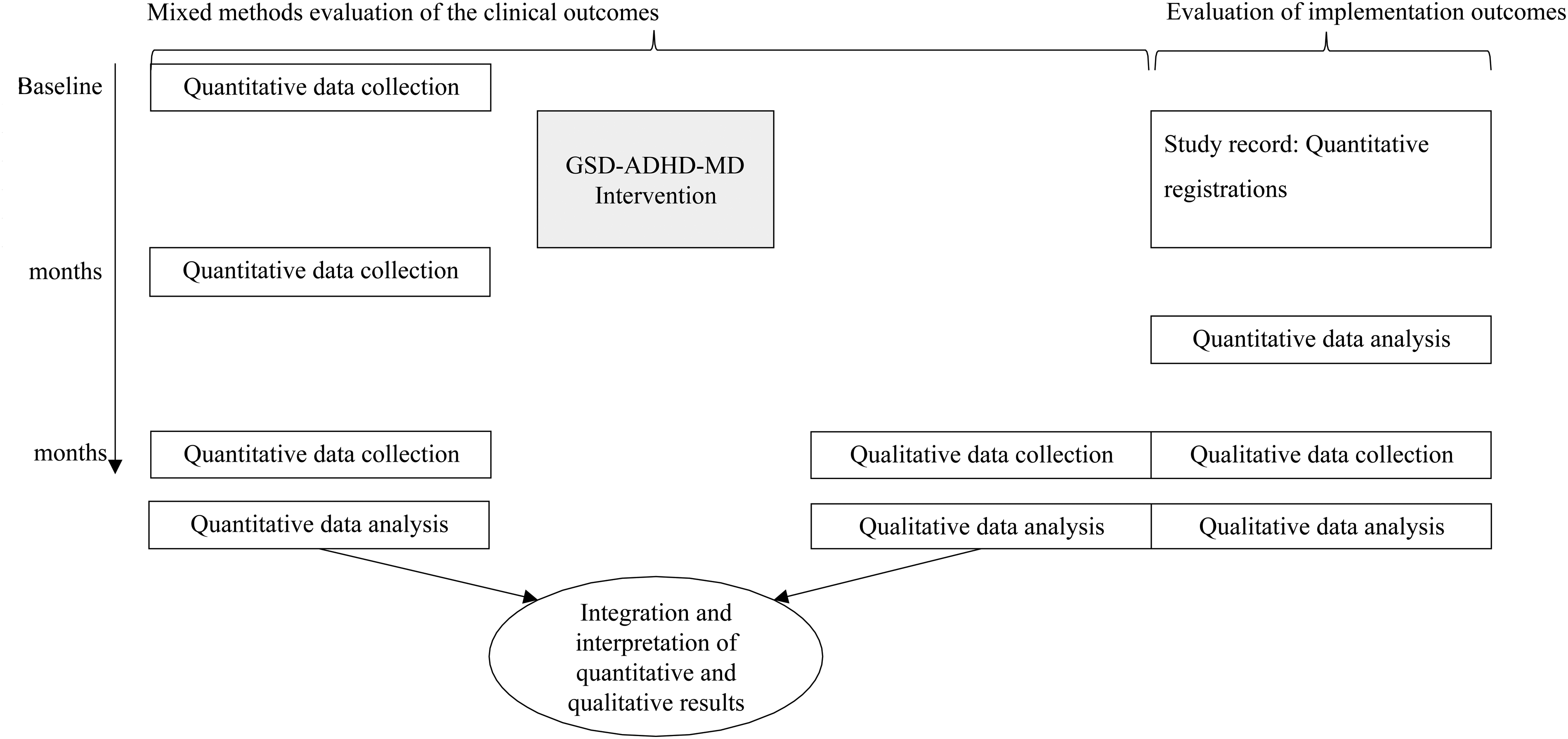
Design of the evaluation of the Guided Self-Determination (GSD) intervention among adolescents with attention deficit hyperactivity disorder (ADHD) and co-existing medical disorder (MD) and their parents.
Setting and participants
The study was performed in 2018–2019 in an outpatient ADHD clinic and an outpatient paediatric clinic at a public university hospital in Denmark.
Twenty-two adolescents were invited of which ten adolescents consented to participate: three females and seven males, aged 13–17 years (mean = 14 years). Nine adolescents were diagnosed with ADHD, and one had ADD (referred to here as ADHD). Their MDs included allergy (n = 1), cerebral palsy (n = 1), constipation (n = 1), epilepsy (n = 1), migraine (n = 1), obesity (n = 3), ulcerative colitis (n = 1) and underweight (n = 1). Parents of all 10 adolescents consented to participate, mothers and fathers (n = 4 + 4) and mothers only (n = 6). The recruitment process has been described elsewhere. 3
The Guided Self-Determination intervention
GSD uses semi-structured reflection sheets and communication to improve patient self-management. 7 Before meeting with the nurse, the patient completes the reflection sheets. At the sessions, the patient reads aloud from the sheets and the nurse uses mirroring, 21 active listening 22 and value clarification 23 to explore the content with the patient. This helps the patient and the nurse to develop a mutual understanding of the patient's difficulties of living with a disorder and serves as a basis for further problem-solving.
The reflection sheets were adapted by replacing the word diabetes with the term disorders. The original version of GSD comprised eight sessions and twenty reflection sheets. 7 The GSD intervention to adolescents with diabetes included parents in the adolescent sessions or in individual parent sessions.11,12 The clinical management at the two included clinics could not allocate resources for that many sessions. Therefore, the intervention was adapted to the core principles of GSD and to require as few sessions as possible to increase the uptake of the intervention in clinical practice. The GSD–ADHD–MD comprised four sessions for the adolescents with 18 reflection sheets and one session for parents with three reflection sheets. Each session had a predefined focus and matching reflection sheets (Table 1). The reflection sheets are shown in the supplementary material, File S2. The parent session was placed after the adolescents’ second session. Each family decided whether parents participated in adolescent sessions, but the adolescents were not invited in the parent session. The intervention was delivered in addition to the usual outpatient care managed by nurses (45–60 min), with a recommended maximum interval of 4 weeks between the adolescent sessions and an expected completion time of 3 months. Two nurses from each outpatient clinic were trained by the first author (HE) to deliver the intervention; the training has been described elsewhere. 3
Overview of GSD–ADHD–MD intervention sessions and reflection sheets.
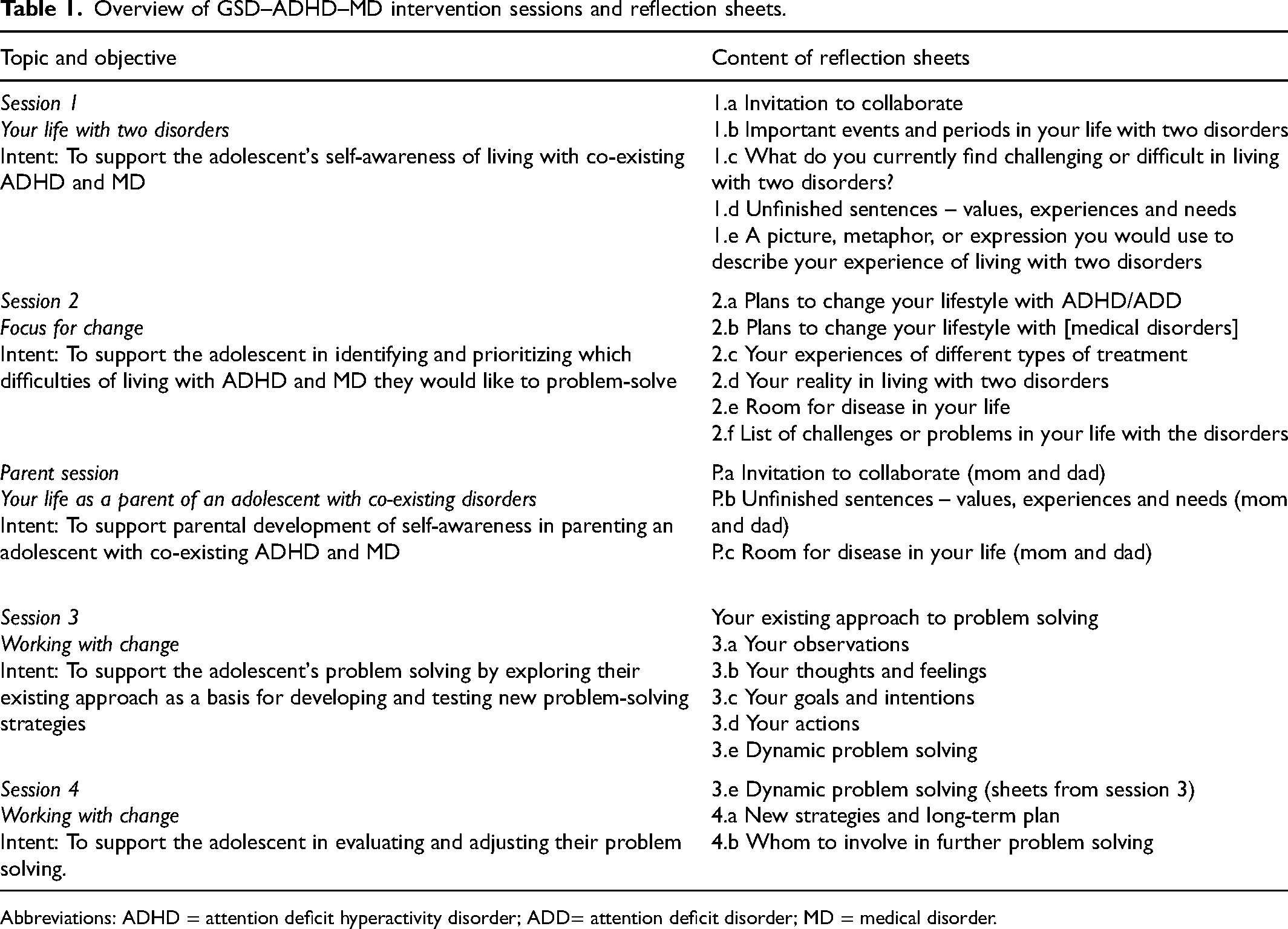
Abbreviations: ADHD = attention deficit hyperactivity disorder; ADD= attention deficit disorder; MD = medical disorder.
Data collection and data analysis
Feasibility
Feasibility was evaluated based on participants’ engagement measured by participation rates. 5 A study record was developed to enable the nurses to register the details of each session: participants’ name(s), session duration, completion of reflection sheets prior to the session and rescheduled sessions. Basic descriptive statistics were calculated for participation rates.
Acceptability
Acceptability was evaluated based on the participants’ perceptions after the intervention had ended. Following Procter et al., 5 the evaluation assessed three dimensions: content, complexity, and comfort. Content included the dual focus on co-existing ADHD and MD, the flexibility of attendance, the four adolescent sessions, the single parent session, and the reflection sheets. Complexity and comfort were interpreted based on the participants’ perceptions of content elements.
Nine of the 10 participating adolescents consented to an individual semi-structured interview, seven of whom completed the intervention. Parents of eight adolescents consented to participate in a semi-structured interview (eight mothers and three fathers) of whom one mother had not participated in the parent session. The interviews were conducted by the first author (HE; experienced interviewer) at the family home, 6 months after enrolment in the study. There was no pre-existing relationship between the parties prior to their enrolment in the study. Parents did not participate in the adolescents’ interview and vice versa. In addition to the semi-structured interview guides (Table 2), copies of the interviewee's reflection sheets were used to prompt further elaboration of their experiences.
Interview guides.
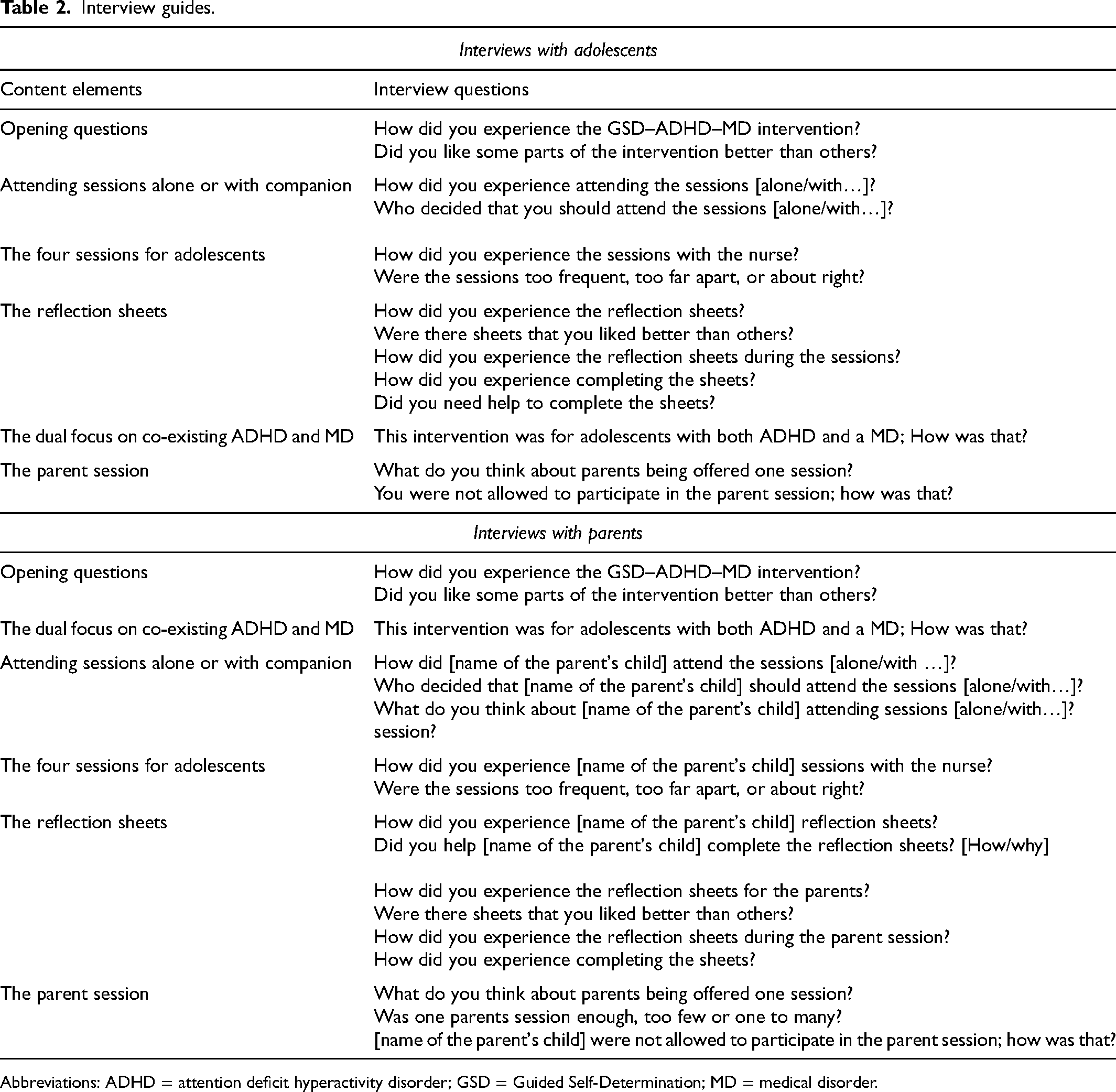
Abbreviations: ADHD = attention deficit hyperactivity disorder; GSD = Guided Self-Determination; MD = medical disorder.
The audio-recorded interviews were transcribed verbatim for thematic analysis. 24 The transcripts were read several times to become familiar with the data. The data describing the participants’ perceptions of the content elements of the intervention were coded. Table 3 illustrates the coding tree. The coded data were searched for patterns to generate themes reflecting adolescents’ and parents’ perceptions of the content elements and their complexity or comfort. The themes were reviewed and refined according to their content. Finally, the themes were named, and the description of each theme was supported by examples and quotes. The analysis was initiated by the first author (HE) and discussed and refined in close collaboration with co-authors. NVivo software was used to organize the analysis. 25
Illustration of the coding tree.
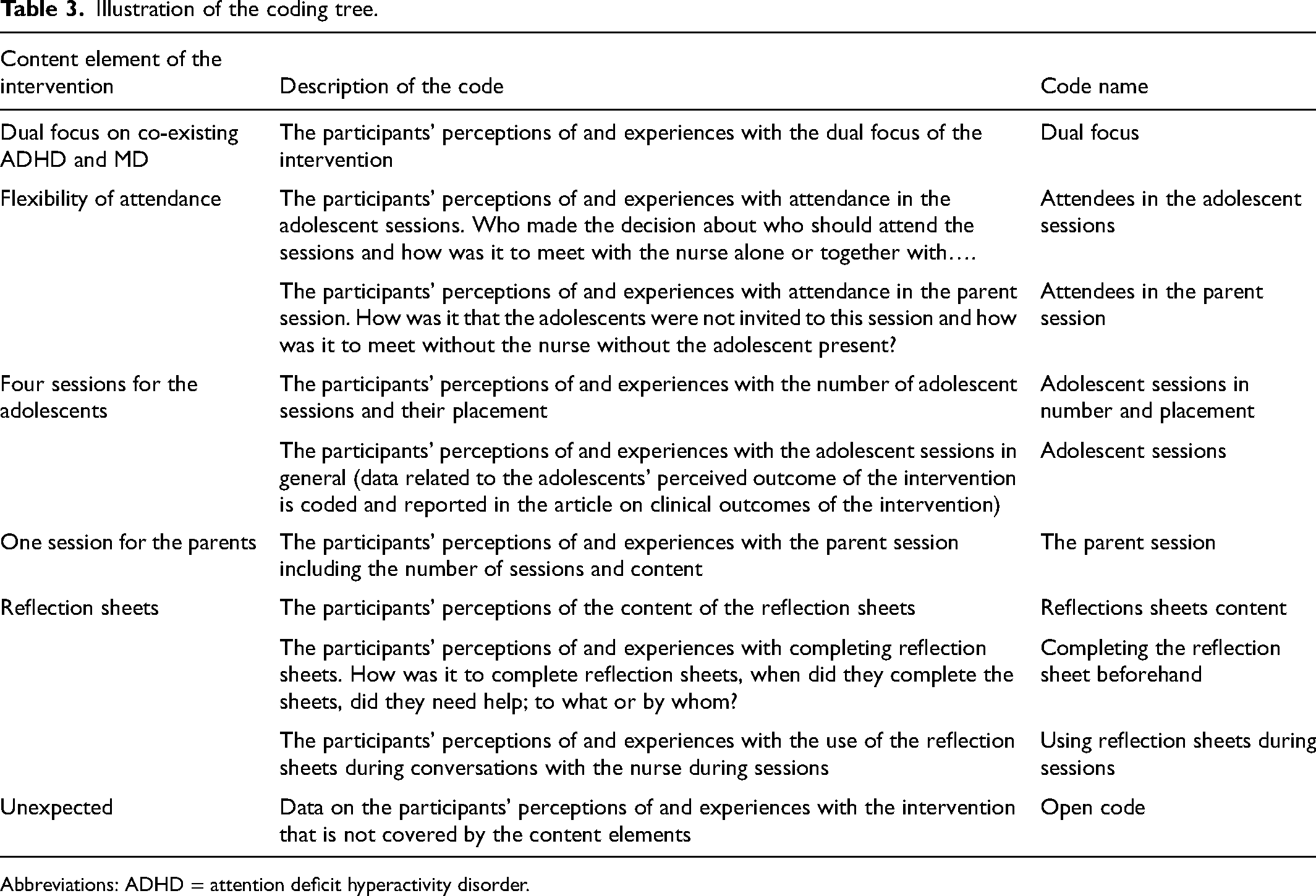
Abbreviations: ADHD = attention deficit hyperactivity disorder.
Ethical considerations
According to Danish legislation, the study was exempted from approval by the Ethics Committee, but the study complies with the principles set out in the Declaration of Helsinki. 26 The participants were given written and verbal information about the study. Participation was voluntary, and participants were guaranteed anonymity and were informed of their right to withdraw from the study without consequence. The study was registered at The Danish Data Protection Agency (2008-58-0028).
Results
Feasibility
The participants’ engagement in the intervention is summarized in Table 4. Three of the 10 participating adolescents dropped out of the intervention; one was reluctant to discuss personal difficulties with the nurse, and the other two had developed new health problems that required treatment at other hospitals. Seven adolescents completed the intervention: three within 11 weeks, one within 15 weeks, and three within 20–23 weeks. In four cases, the intervention was prolonged by the need to reschedule due to various reasons. Parents of seven adolescents participated in the parent session. In three of the parent sessions the mother participated and in four parent sessions both the mother and father participated. Five of the adolescents (aged 13–17 years) attended the sessions alone, and five (aged 13–15 years) attended the sessions with a companion. Sessions 1 and 2 and the parent session each lasted about an hour; sessions 3 and 4 lasted about 30 min. More adolescents completed the reflection sheets before sessions 1 and 2 than before sessions 3 and 4, except for sheets 1.e (picture, metaphor, or other expression) and 2.c. (experiences of treatment). Five of the seven mothers and half of the fathers completed all the reflection sheets before the parent session. Table 4 also provides a detailed overview of how many adolescents completed which reflections sheets before the different adolescent intervention sessions and how many parents completed which of the reflection sheets before the parent session.
Adolescents’ engagement with the GSD–ADHD–MD intervention.
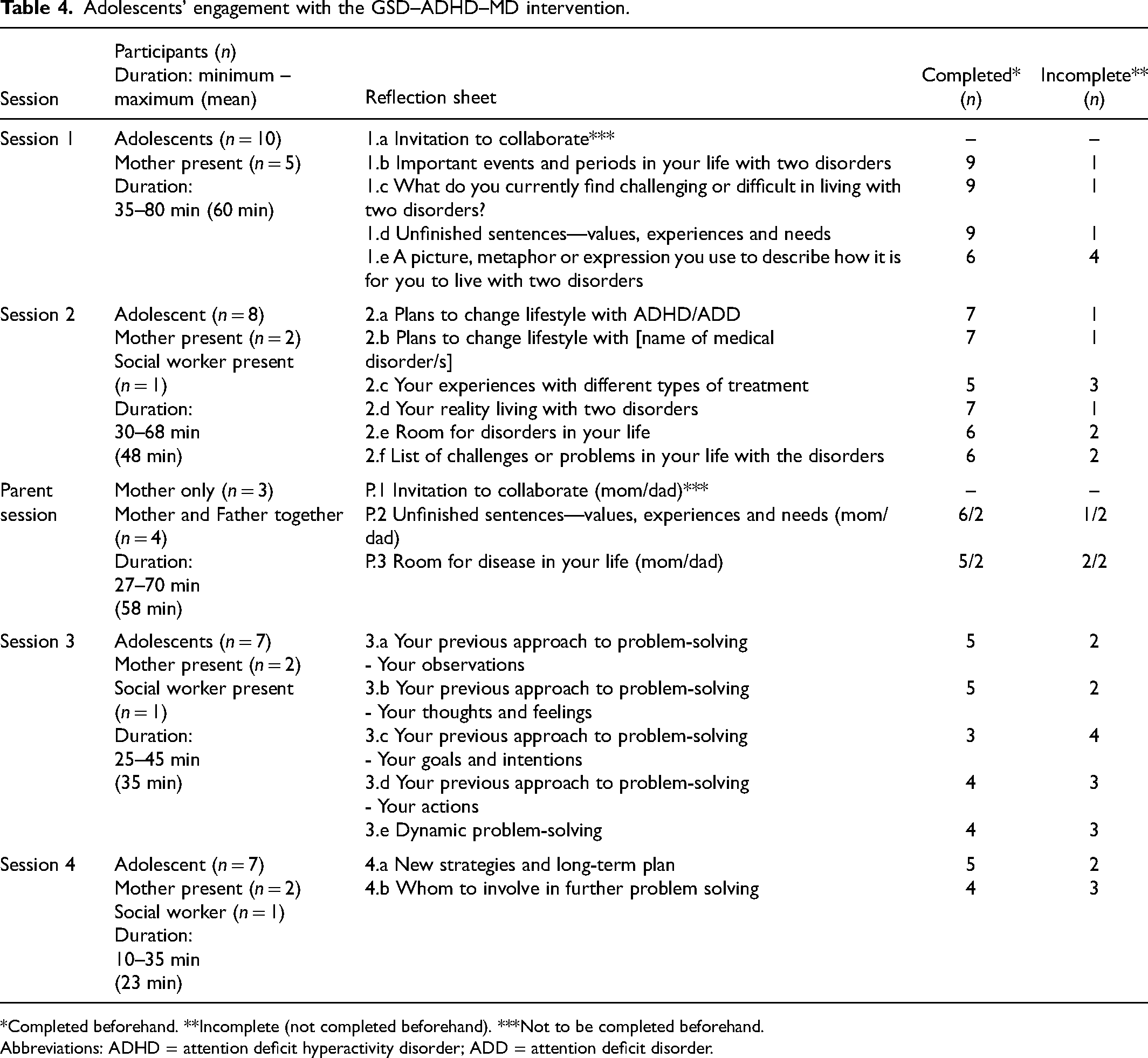
*Completed beforehand. **Incomplete (not completed beforehand). ***Not to be completed beforehand.
Abbreviations: ADHD = attention deficit hyperactivity disorder; ADD = attention deficit disorder.
Acceptability
The analysis generated three themes.
Personal preferences for attending intervention sessions
The adolescents received the sessions at different intervals. Some adolescents felt that it was appropriate to have one session each month: “It can’t be too often… nor should there be too long a time between visits… I think a month is appropriate” (P4). Others had weekly or biweekly sessions and found this preferable: “Once a week was better because then I was better able to remember what we had talked about last time” (P8). Some adolescents expressed concerns if the time interval between sessions was too long, and others worried that the intervention would interfere too much with their everyday life if the sessions were too frequent. By contrast, none of the parents expressed concerns of the sessions being placed too often: “…the thing that was good, was when [nurse] and [adolescent] sat together often, because that really made a difference” (Mom6). Parents accepted frequent sessions as they perceived them more beneficial for the adolescents, whereas attending the sessions based on personal preferences made participation more comfortable for the adolescents.
The adolescents appreciated being able to decide if they preferred to participate in the sessions alone or with a companion. For four of the five who attended the sessions alone, it was the first time they met with a nurse alone: “I have always had my parents speaking on my behalf” (P1). Respecting the personal preferences of the adolescents made participation more comfortable and the adolescents accepted being actively involved in the encounter. The parents supported the adolescents as they highlighted the adolescents’ need for a room to talk more freely. However, some of the parents were concerned about missing important knowledge. “For my part, it has been a bit irritating, because I like to know what is going on. But for her part,… it has been really good” (Mom2). Other parents expressed concerns about their adolescent needing help to express their viewpoints. “We have to tell what it is he is experiencing because it is not always, he will bring it up himself” (Dad5). The parents’ concerns indicate that they felt losing control. Some parents tried to initiate conversations about the adolescent's sessions. “I have tried to get her to talk…., but she just closed up. It is not something to poke one's nose into” (Mom8). Although parents accepted the adolescents’ preference for attending sessions alone it was accompanied with some degree of discomfort as they were not informed about what was discussed or agreed on at the adolescents’ sessions.
The five adolescents who attended sessions with a parent or social worker appreciated having a companion who helped them to express their point of view and to remember what was discussed or agreed on during the sessions: “She [mom] can hear what is said, because she remembers a little bit better than me” (P7). For these adolescents, having a companion present seemed to make the sessions more comfortable. The parents that had accompanied their adolescent described similar experiences about their role in these sessions.
All interviewed parents except one appreciated that they attended the parent session without the adolescents; “you can bring up things that would be difficult to bring up, if he was present” (Dad6). Parents seemed comfortable with privacy when discussing concerns or challenges with the nurse. In addition, the adolescents spoke positively about the parent session: “The parents may get some counselling on what they can do to help their child” (P2). The adolescents seemed aware of their parents’ need for the nurses’ help in providing the best possible support for them, which made the adolescents comfortable with the parent session.
Reflection sheets as a turning point in conversations
The adolescents highlighted that the reflection sheets changed the content of the conversation with nurses; by focusing on their everyday life with ADHD and MD, they were able to talk about what they considered important. However, the adolescents also expressed uncertainty about whether they could address ADHD-related issues with the nurse at the paediatric clinic or vice versa: “You could say what was important to you, and that makes sense. But I was also a bit confused because I thought that you only talked about ADHD at the ADHD clinic” (P2). The adolescents accepted the dual focus of the intervention, but it also added some complexity. Some of the parents described that the reflection sheets and the dual focus of the intervention introduced a turning point. “It is the only right thing…. We will never ever resolve this [MD] if we only look at the physical aspects. If we don’t deal with it all, then we will not get it solved” (Dad6). The holistic understanding of the adolescents’ challenges seemed imperative in helping the adolescents.
The reflection sheets led to more focused conversations for the adolescents, even when not completed beforehand: “We took one sheet at a time… it was better, because we had something tangible to talk about…. it helped me to follow the conversation” (P8). The adolescents highlighted that the sheets helped them to play an active role in the sessions: “You read out loud what you have written, and then you have to explain it so the nurse can understand what you wanted her to understand” (P1). The adolescents felt that the sheets made the conversations more meaningful and focused and supported them in expressing their views. In addition, two of the three parents who had attended the adolescents’ sessions described that the sheets facilitated a mutual understanding between parent and the adolescent. “I think, something that surprised him a lot was the example with shading [reflection sheet 2.e]. How much it [MD and ADHD] impacts me and how much it impacts him. He was very surprised to see it visually” (Mom6). This indicates that parents were comfortable with conversations based on reflection sheets as they facilitated mutual insights.
Some adolescents felt that the nurses hurried through the conversation and did not pay enough attention. Consequently, they became less interested in elaborating on the sheets. This suggests that the nurse's approach to the conversations or the number of reflection sheets was also important factors for adolescents’ engagement.
The parents were not used to nurses focusing on them as parents; “I think we could have used it earlier. She has had the diagnosis since second grade, and we have actually not really got any help until now” (Mom1). They did not elaborate on the use of reflection sheets in the parent session, but they described that the nurses took their challenges seriously and intended to help them. This indicates that the parents accepted and were comfortable with reflection sheets being part of the parent session. However, none of the parents found that one parent session was enough: “I believe that one conversation is a hundred times better than none because it put something in motion. But where do you then go with that…” (Mom3). The parents requested follow-up parent sessions that allowed back-and-forth processes about their challenges and how to manage them.
Being supported or challenged by the completion and content of the reflection sheets
Although the adolescents were willing to complete the reflection sheets prior to the sessions, they approached it differently. In four cases (including two who dropped out of the intervention), the parents wrote the adolescents’ answers because they were uncomfortable about writing: “She [mom] wrote the things I asked her to write” (P5). The fact that they needed parental support suggests they found it complex. Five adolescents completed the sheets themselves and only involved their parents if they were unsure of what was required or needed help to remember details (e.g., age at diagnosis). The adolescents further explained that they did not share their sheets with their parents because they did not want their parents to suggest changes. However, it was difficult for the adolescents to respond to all the reflection sheets. Some adolescents found it difficult to put their thoughts on paper: “It was not difficult to figure out, but it was hard to put my answers into writing” (P8). Despite the challenges, adolescents were generally comfortable completing the sheets on their own. The parents reported that they often had to remind the adolescents about the reflection sheets, and the mothers who completed the sheets together with the adolescents were aware of their role: “I was very conscious about not putting my words into his mouth” (Mom3). The parents accepted it although it was difficult.
The parents were willing to prepare reflection sheets prior to the parent session. However, three parents had forgotten about the sheets and the rest found it difficult and time-consuming to do: “You got to think about things when you sit with these questions. It was sometimes difficult to answer the questions because you have not thought about it” (Mom1). Additionally, parents living together found that the sheets initiated conversations with their partner: “It is very interesting to know based on these sheets. I see differences in how we perceive things, and that gave us an opportunity to talk together at home” (Mom4). Although parents found it complex to complete the sheets, they accepted it because they gained new insights.
Another important aspect was the content of the reflection sheets. The adolescents indicated that they found some reflection sheets supportive and others challenging. When the adolescents were asked to share their impressions of the sheets, most focused on the first two sessions; only one commented on the sheets from session 3 and 4: “I couldn’t quite get the hang of it [the content of sheet 3.a-e]” (P7). In addition, none of the parents elaborated on the concrete content of the adolescents’ or the parents’ reflection sheets.
The adolescents highlighted several sheets as satisfying to work with. Sheet 1.b (lifeline important events and periods) helped them to develop a better understanding of their lives with both disorders: “When I saw it on paper, it gave me an overview of what I struggle with. This is not something I normally think about” (P2). Sheets 1.d (unfinished sentences) and 2.e (room for disease in your life) prompted reflection about everyday life, which they found enlightening. Some appreciated sheet 1.e (a picture, metaphor, or expression) because it allowed them to be creative: “it was good to show something without needing to have all the words” (P4). All these sheets focused on everyday life with co-existing disorders and enabled the adolescents to reflect on this. There was no indication that anyone was uncomfortable with any of the content.
The adolescents found some of the reflection sheets for Session 2 challenging to work with. The layout of sheets 2.a and 2.b (plans to change lifestyle ADHD/MD) was confusing because they had to consider several aspects of each lifestyle recommendation: “It really is simple, but in my head, it was difficult to figure out. You had to put crosses on [both] sides” (P1). Reflection sheets 2.c (experiences with treatment) and 2.d (living with two disorders) were difficult because the adolescents did not always know which treatments they had tried or how to describe the impact of symptoms on daily living. In general, the content of these sheets was perceived as complex if the layout was not intuitive or if completion depended on knowing about disorders and their management.
Discussion
The present study aimed to evaluate the implementation outcomes (feasibility and acceptability) of the GSD–ADHD–MD intervention by investigating how adolescents and their parents used and perceived the intervention. The adolescents and parents accepted the dual focus of the intervention, but it also introduced complexity by conflicting with their expectations as they usually attended separate clinics for ADHD and MD. The World Health Organization 27 recommends that professionals take co-existing disorders into account because treatment should be understood in the context of the individual patient. This intervention was able to integrate co-existing disorders in outpatient care. However, preparing adolescents and their parents for this dual focus seems important to ensure their comfort. Therefore, the dual focus should be introduced on reflection sheet 1.a/P.a (mutual expectations for collaboration) in future use.
Attending intervention sessions based on personal preferences was important. Five adolescents aged 13–17 years were comfortable meeting nurses without their parents and accepted their active involvement in these encounters. This can be interpreted as the quest for independence from their parents, which starts around the age of 12–14 years. 28 However, these young adolescents preferred to attend on their own, although ADHD tends to delay maturity by a few years. 29 This may explain why the other five adolescents (aged 13–15 years) were more comfortable attending with a companion. The need for help in expressing themselves and difficulties in remembering discussed topics indicates that some adolescents found the sessions complex. Similar findings were found among adolescents with diabetes in the group-based GSD intervention. 14 The fact that the intervention could be tailored to personal preferences seemed to enhance the acceptability and make participation comfortable for the adolescents. However, adolescents should be involved in decisions about how to attend sessions.
The adolescents and the parents found that the reflection sheets made conversations more tangible and focused. This suggests that the reflection sheets were effective in ensuring that all parties were aware of the subject being discussed, helping them to develop a mutual understanding of the patient's difficulties.8,30 Additionally, ADHD is associated with inattention 31 and adolescents with ADHD are more motivated to engage in activities that support their sense of competence. 32 The sheets provide structure that may support these adolescents’ sense of competence; however, preparing the sheets in advance was a demanding task, which may have diminished the adolescents’ motivation for filling out the sheets. Individuals with ADHD tend to be more motivated by activities where the desired outcome is achieved immediately, and less motivated when the outcome is delayed. 33 The benefit of working with the reflection sheets at home was not realized until the sessions with the nurse, which may have influenced the adolescents’ motivation and challenged parents in supporting the adolescents’ completion of the sheets.
The duration of the parent session and sessions 1 and 2 were almost twice as long as sessions 3 and 4 which may be due to the content of the sessions. Sessions 3 and 4 focused on problem-solving. ADHD is associated with working memory problems, leading to difficulties in processing verbal and visual information and using that information in decision-making. 34 The problem-solving tasks can have seemed too complex, which may explain the lower levels of engagement in these sessions. To fully understand the intervention's potential to support problem-solving among adolescents with ADHD and co-existing MD, more research is needed on the use and perceptions of the reflection sheets in the adolescent sessions.
Overall, the adolescents indicated that the content of sessions 1 and 2 and the associated reflection sheets were acceptable. They appreciated the opportunity to reflect, as this helped them to gain a better understanding of their situation. This further confirms the appropriateness of these sessions and reflection sheets because they facilitate self-exploration and insight as intended. 8 Conversely, the adolescents reported that some of the reflection sheets were complex, which is also described by adolescents with diabetes. 14 The present study reported that reflection sheet 2.c was complex because the adolescents were unaware of previous treatment. This may be because responsibility for treatment is only gradually transferred from the parents during adolescence. 2 The layout of reflection sheets 2.a and 2.b was perceived complex, perhaps due to problems with working memory challenging the process of a lot of information. 34 Further adjustments are needed in terms of content and layout.
The adolescents sometimes found that nurses hurried through the sessions, indicating that the number of sheets and session should be considered. In addition, the adolescents did not share the content of their sessions with their parents, which is a challenge because parents often are the most important allies in adolescents’ disease management. 2 The adolescents may need parental support to maintain or implement the changes they have chosen based on their engagement with the GSD–ADHD–MD intervention. A support parents are unable to provide if they are not involved. Moreover, parents requested more parent sessions. Thus, the optimal number of sessions and reflection sheets and how the intervention supports collaboration between the adolescents and their parents warrant further research.
Strengths and limitations
It could be considered a limitation that it was a pragmatic solution to reduce the number of intervention sessions in this study. However, a review on GSD shows that it has clinical significance despite differences in intervention dose (number of sessions and reflection sheets). 6 It is a strength that nine adolescents, eight mothers and three fathers participated in an interview, including parents and adolescents who had not completed the full version of the intervention. This ensured variation in the sample 35 and included multiple perspectives about the intervention. Acceptability should ideally also be investigated from the perspectives of the nurses delivering the intervention to ensure an even broader understanding. 5 Data collected through interviews are highly relevant when exploring participantś experiences on a topic. 36 However, the timing of the interviews was not optimal because some participants found it difficult to recall their experiences on the specific sessions and reflection sheets in detail. This approach was adopted to avoid any interference with data collection for the evaluation of clinical outcomes (Figure 1). 3 Although the first author (HE) initiated each step in the thematic analysis, the management of the analytical process, including the development of initial and final themes, was discussed collaboratively with the co-authors throughout. This collaborative approach strengthened the analysis by promoting researchers’ reflexivity, which is essential to ensure that the themes accurately represent the data and, as noted by Malterud, 37 enhances the validity of qualitative findings.
Conclusions
The feasibility and acceptability of the GSD–ADHD–MD intervention are complex and dependent on the participants’ use of the intervention. However, the content of the intervention and the flexibility in how the adolescents and the parents used the intervention seems important for the feasibility and acceptability of the intervention. Overall, the adolescents and their parents found the use of reflection sheets with the nurses acceptable and comfortable, yet completion of the reflection sheets was considered complex for both parties. The sessions and reflection sheets that focus on everyday life with co-existing disorders (adolescent sessions 1 and 2) and the parent session were more feasible and acceptable than those related to problem-solving (adolescent sessions 3 and 4). The results also point to areas that need further adjustments, the content and layout of reflection sheets for adolescents, the number of sessions and reflection sheets for adolescents and parents, and the collaboration between adolescents and parents on the management of co-existing disorders. However, the GSD–ADHD–MD intervention's ability to integrate co-existing disorders and the use of reflection sheets with the nurses suggests that it has the potential to support empowerment among adolescents with co-existing ADHD and MD in clinical practice.
Supplemental Material
sj-docx-1-njn-10.1177_20571585241300244 - Supplemental material for Feasibility and acceptability of the Guided Self-Determination intervention for adolescents with co-existing ADHD and medical disorder and their parents
Supplemental material, sj-docx-1-njn-10.1177_20571585241300244 for Feasibility and acceptability of the Guided Self-Determination intervention for adolescents with co-existing ADHD and medical disorder and their parents by Helle Enggaard, Britt Laugesen, Melissa DeJonckheere, Michael Derwin Fetters, Marlene Briciet Lauritsen, Vibeke Zoffmann and Rikke Jørgensen in Nordic Journal of Nursing Research
Supplemental Material
sj-doc-2-njn-10.1177_20571585241300244 - Supplemental material for Feasibility and acceptability of the Guided Self-Determination intervention for adolescents with co-existing ADHD and medical disorder and their parents
Supplemental material, sj-doc-2-njn-10.1177_20571585241300244 for Feasibility and acceptability of the Guided Self-Determination intervention for adolescents with co-existing ADHD and medical disorder and their parents by Helle Enggaard, Britt Laugesen, Melissa DeJonckheere, Michael Derwin Fetters, Marlene Briciet Lauritsen, Vibeke Zoffmann and Rikke Jørgensen in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We thank the participating adolescents and parents, the nurses who delivered the intervention, and the healthcare professionals that assisted with the recruitment process.
Author contributions
CRediT authorship contribution statement:
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.