
Abstract
Contact nursing services have been implemented in Swedish cancer care to increase healthcare quality. Too little is known about the content and quality of these services and the organizational prerequisites provided to contact nurses. The aim of this study was to explore contact nurses’ perceptions of their services and organizational prerequisites, as well as the connection between organizational prerequisites and moral stress. A cross-sectional survey was utilized consisting of a study-specific questionnaire and a select part of the Stress of Conscience Questionnaire. The study is reported in accordance with STROBE guidelines for cross-sectional studies. The results showed that contact nursing service content varied across settings and that 84% of contact nurses have what was categorized as satisfactory or moderately satisfactory self-reported organizational prerequisites. Perceived moral stress differed between contact nurses depending on organizational prerequisites. The variability of both services and prerequisites can be described as inequities in care and complicates evaluation and comparison.
Introduction
Cancer care is characterized by a high degree of complexity and, as diagnostics, treatments and rehabilitation evolve and become more efficient, people live longer with the consequences of cancer. 1 This places high demands on the healthcare professionals who are tasked with supporting people affected by cancer. Nurses constitute the largest profession within cancer care 2 and are key actors across the entire care trajectory and across cancer care settings. 3 Europe's Beating Cancer Plan 4 highlights the importance of providing healthcare professionals with sufficient support, so that they in turn can deliver high-quality care. To achieve high-quality care, it needs to be organized and resourced in a manner that allows healthcare professionals to optimize the utilization of their skills and knowledge. Donabedian's seminal conceptualization of structural quality 5 is described as ‘the conditions under which care is provided’ and concerns matters such as formal competency, the suitability of facilities, tools for work, workplace culture, leadership and management, administrative systems, and organization of care. 6 The term ‘organizational prerequisites’ is frequently used throughout this paper. It is to be understood as related to Donabedian's concept of structural quality, addressing meso and macro aspects of care provision that are out of the control of the individual nurse.
As cancer care develops, cancer nursing practices evolve and advance. 3 A multitude of titles, certifications, and educational programmes for registered nurses (RN) in cancer care have been developed internationally. The titles Oncology nurse navigators, 7 Cancer clinical nurse specialists 8 and Advanced nurse practitioners 9 are all examples of this. Besides an increased emphasis on academic work (nurses in these positions hold at least a master's degree in nursing science) and healthcare improvement efforts, RNs in such positions work autonomously, monitoring and addressing patients’ care needs, and they also collaborate within a multidisciplinary team to coordinate care. These nurse-led services have been shown to have positive effects for patients. 10 In Sweden, the strife towards more advanced and autonomous nursing roles has taken the form of the development of the role contact nurse in cancer care (CNCC).
CNCC services have been successively implemented in Swedish cancer care since the launch of the Swedish National Cancer Strategy in 2009, 11 where it was suggested that everyone diagnosed with cancer was to be offered the services of a CNCC. CNCCs serve patients across the entire clinical trajectory, supporting people with varying care trajectories, diagnoses, symptoms and side effects. CNCCs operate in different types of clinics within secondary care institutions, such as oncological, surgical, neurological, urological, gynaecological and haematological clinics. A national description of the scope of CNCC services has been developed, identifying lowest common denominator for CNCCs across these settings. 12 This description is indicative, but not statutory for operations to adhere to. According to this document, CNCC services include nursing care aimed at providing information and psychosocial support, assessing care needs, ensuring patient participation, establishing individual cancer care plans and facilitating active care transitions. Operating as a CNCC does not require any formal competence apart from being a registered nurse. However, Swedish universities offer non-mandatory advanced level courses to CNCCs.
The implementation of CNCC services in Swedish cancer care has been described as a success. 13 Access to these services seems to be increasing 14 and studies have reported access to be relatively high (76–88%).15–17 Sjövall et al. 16 found that being assigned a CNCC was associated with higher patient satisfaction in a sample of patients with colorectal cancer. However, other studies have not been able to detect positive effects for patients with access to CNCC services.18,19 Larsson and Bjuresäter 20 identified a substantial variation regarding the scope of practices and the organizational prerequisites of CNCC services. Issues of delimitation and variability of services across settings have also been highlighted in the international literature regarding comparable cancer nursing services.8,21,22 This warrants a closer look into whether CNCC services are organized and resourced in a manner that allows CNCC to provide patients with high-quality care.
Furthermore, organizational prerequisites impact not only the quality of care for patients, but also the work environment of CNCCs. A substandard work environment can contribute to feelings of inadequacy, stress and nurse burnout, 23 and may lower retention rates. 24 There is a critical interplay between the quality of care provided to patients and the quality of the organizational prerequisites provided to healthcare professionals. 25
In sum, CNCC services can be described as a part of an ongoing international endeavour to improve cancer care by advancing nursing practices. To maintain and develop sustainable CNCC services, it is essential to assess them from different perspectives. It has been argued that healthcare improvement studies and projects mainly focus on process improvements (the micro or possibly meso perspective) and too little on the improvement of the healthcare system and organization (meso, macro or structural level).6,26 Therefore, the present study utilized the lens of organizational prerequisites, where the structural aspects of care provision take centre stage.
The aim of this study was to explore CNCCs’ perceptions of their services, organizational prerequisites and moral stress.
Methods
This is a cross-sectional study. This study is annotated in accordance with The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines for cross-sectional studies 27 and the guidelines devised by the International Committee of Medical Journal Editors on uniform requirements for manuscripts submitted to biomedical journals. 28
Context
The Swedish healthcare system is predominantly public and comprised of 21 self-governing regions. These regions cooperate around the utilization of resources through six so-called healthcare regions. Each healthcare region has a Regional Cancer Centre (RCC), a civil servant organization promoting the development of cancer care. Some types of cancer care are highly specialized and are only performed at a limited number of units regionally or nationally, which requires further cooperation across regional borders. The state governs health care through legislation and fiscal instruments. 29
Hospitals are referred to as university hospitals, county hospitals or smaller county hospitals. County hospitals have competence and resources to address care needs within most areas of healthcare, whereas smaller county hospitals have limited offerings and less emphasis on specialized care. University hospitals are responsible for more rare, complex and resource intensive care. They receive referrals from the smaller hospitals and cooperate closely with academia. 30 CNCCs can be employed at any of these (and to a small extent also by private clinics). Due to the multimodal treatment approach required for many cancers, it is common for patients to receive care at several different units within a hospital or at different hospitals, depending on the patients’ place of residence.
Recruitment
Although no formal registry exists, the RCCs estimate that there are approximately 1500–1800 registered nurses in Sweden that work as CNCCs. The intention was to include all CNCCs operating during the study period. The inclusion criterion was therefore: being identified by one of the RCCs as working as a CNCC in Sweden.
Data collection
The study utilized a convenience sampling strategy. Data were collected between March and December 2020, with a disruption between April and September due to the COVID-19 pandemic. The RCCs distributed the survey link to their networks throughout their respective healthcare regions, either via cancer coordinators, managers or directly to CNCCs, depending on the preferences of the line managers. One region declined participation. In the invitation email containing link to the survey, respondents were given customary information to research participants, including information regarding the voluntary and confidential nature of participation. Respondents gave their informed consent by clicking the survey link. Two reminders were sent.
Instrument
The survey consisted of the study-specific Quality of care and Organizational Prerequisites for Contact Nurses (QOPCoN) questionnaire and the Stress of Conscience Questionnaire (SCQ). 31 The survey was programmed and hosted on a secure platform by the survey company IMPROVE-IT (https://improveit.se).
The QOPCoN questionnaire consists of 61 questions, divided into five domains: Demographics (two items), Formal competence (10 items), Employment (eight items), Organization of care (26 items) and Work tasks and services (15 items). The Formal competence domain charts respondents’ work experience and formal competence (i.e., if they have a specialist nurse degree or have completed a higher education course for CNCCs). In Employment, CNCCs report formalities regarding their employment and what patient group(s) they serve. In the domain Work tasks and services, each item was answered from two perspectives, referred to as perceived reality (PR) and subjective importance (SI). PR means respondents position their view regarding a claim, for example, ‘I provide psychosocial support to patients’, on a four-point Likert scale ranging from 1 (‘I do not agree at all’) to 4 (‘I fully agree’). Thereafter, they position their view regarding how important (SI) they perceive that item to be for patients on a four-point Likert scale ranging from 1 (‘Of little or no importance’) to 4 (‘Of the greatest importance’). A ‘Not applicable’ option was available for both scales. The Organization of care domain assesses how CNCCs perceive issues regarding, for example, availability and continuity across the care trajectory, workload and suitability of facilities. Twelve of the items in this domain follow the same logic as Work tasks and services, in that they ask about both perceived reality and subjective importance, whereas the remaining items have answer options that range from ‘Completely agree’ to ‘Do not agree at all’, with an option to answer, ‘Not applicable’. The questionnaire in its entirety is available as a supplementary file.
The SCQ is composed of nine two-part items (part A and part B). Part A assesses how often the respondent is exposed to a specified situation on a six-point Likert scale ranging from 0 (never) to 5 (every day). Part B assesses the extent to which these situations are perceived as leading to a troubled conscience on a 10-cm visual analogue scale, with the endpoints representing ‘No, it does not trouble my conscience at all’ and ‘Yes, it troubles my conscience greatly’, respectively. SCQ scores are calculated by multiplying part A (range 0–5) and part B (transformed from the 10-cm visual analogue scale into five groups, thus also a range of 0–5). The possible range per survey item is therefore 0–25.
As it became clear that the COVID-19 pandemic would have a substantial impact on cancer care, an additional area of inquiry, concerning the effects of the COVID-19 pandemic on CNCC services (10 items), was added to the survey as data collection resumed in September 2020. Those data have been published elsewhere 32 and are not a part of this study.
Statistical analysis
All statistical analyses were performed using the SPSS, version 28. 33
Subgroups were created according to healthcare region affiliation, what type of hospital CNCCs were employed at and the diagnosis group served. Only respondents serving exclusively one patient group were sorted into that category. Respondents serving more than one patient group were sorted into a separate category.
Descriptive data analysis methods were applied (specifically frequency, proportions, means and range). The choice of method depended on the characteristics of the respective survey item. Some survey items were formulated as claims, with CNCCs indicating to what degree they agreed with the claims on a four-point Likert scale. The replies ‘Completely agree’ and ‘Agree to a large extent’ were grouped to indicate confirmation.
In the domain Work tasks and services, both PR and SI of specific aspects of CNCC services were addressed. An index was created where the two dimensions were combined. Percentage in agreement with the PR dimension is calculated by the number of respondents that answered ‘Mostly agree’ or ‘Fully agree’ divided by the total number of respondents. Similarly, the respondents that replied ‘Of high importance’ or ‘Of the very highest importance’ are categorized as ‘high importance’ in the SI dimension. All respondents are placed in one out of four categories, labelled ‘Deficient quality’, ‘Low balance’, ‘High balance’ and ‘Superfluous quality’.
Survey items regarding availability across the care trajectory were formulated as how often CNCCs typically were in contact with patients at five time points (before start of treatment, during treatment, 0–3 months, 3–6 months and 6–12 months after completion of treatment). Responses were dichotomized as typically never having contact or typically having contact once or more during the five time points.
Exploratory factor analysis (EFA) is a method that can aid the understanding of data by identifying clusters and patterns of variables. 34 It was utilized as a tool to identify and compare self-reported organizational prerequisites for CNCCs. Ten survey items explicitly addressing organizational prerequisites were included in the EFA (see the Results section for more detail). The KMO value of 0.812 indicated a strong correlation. Additionally, the chi-squared result from Bartlett's test of sphericity was equivalent to 1017.40 with a significance level of <0.001. Thus, the data were deemed suitable for EFA. An eigenvalue ≥1 was set as cut-off to retain a factor. Item loading ≥0.45 was considered acceptable. The research team reached consensus regarding labels for the factors through discussion. The analysis yielded two factors, labelled Prerequisites as provided and Prerequisites as perceived.
Mean sum score for the items placed in factor one, (which was named Prerequisites as provided), was used as indicator of organizational prerequisites for CNCCs. The factor consists of the following items: I have a written assignment, signed by my manager; I have allotted time for my assignment as CNCC; I have a room allotted to my work as a CNCC; and I work independently in a clinic where I assess symptoms and needs and provide care. All items in factor 1 had answer options that ranged from 1 to 4. Cut-offs were set to indicate Satisfactory (top 25% of the response scale, mean value ≥3.36), Moderately satisfactory (middle 50% of the response scale, mean value 1.75–3.25) and Unsatisfactory (bottom 25% of the response scale, mean value ≤1.74) organizational prerequisites. See the Results section for further information.
To investigate CNCCs’ perception of how moral stress (which is characterized by experiencing incompatible demands and lack of control 35 ) differed according to organizational prerequisites, a study-specific selection of SCQ items were analysed. The SCQ is commonly analysed as a unidimensional total score of all nine survey domains. However, Glasberg et al. 31 suggested a two-domain solution, referred to as Internal demands and External demands and restrictions. This solution has also been described as theoretically meaningful by Åhlin et al. 36 Internal demands refer mainly to the internal voice of the caregiver, whereas External demands and restrictions focus on the surrounding structures. Given the question under investigation in this study, the survey items related to External demands and restrictions were used for analysis, with exception for of item 6 (‘Is your private life ever so demanding that you don't have the energy to devote yourself to your work as you would like?’) (Table 1). The mean score for the four selected survey items was calculated. Thereafter, analysis of variance was utilized to explore differences between groups of CNCCs with different organizational prerequisites, as defined by the factor analysis (see above). Tukey’s post-hoc test was applied. p < 0.05 was considered statistically significant.
Overview of the items utilized from the Stress of Conscience Questionnaire (SCQ).

Ethical considerations
The study protocol was approved by the Swedish Ethical Review Authority (Reg. no 2019–04958) and the study was conducted in accordance with the Declaration of Helsinki. 37 All data have been stored and processed on secure platforms to safeguard confidentiality, only accessible to the research team.
Results
The survey was completed by 535 CNCCs (132 responded before and 403 responded after the COVID-19 amendment). Assuming the estimation of the number of CNCCs (1500–1800) was correct, this gives a response rate of between 29.7% and 35.7%. Characteristics of respondents are described in Table 2. Half of the respondents (49.7%) had completed a higher education course for CNCCs and less than half (41.7%) had a degree as specialist nurse (equivalent to 60 higher education credits at advanced level). Most respondents had a public employer (95.1%) and it was most common to be employed at a county hospital (44.5%).
Demographical information about survey respondents (N = 535).
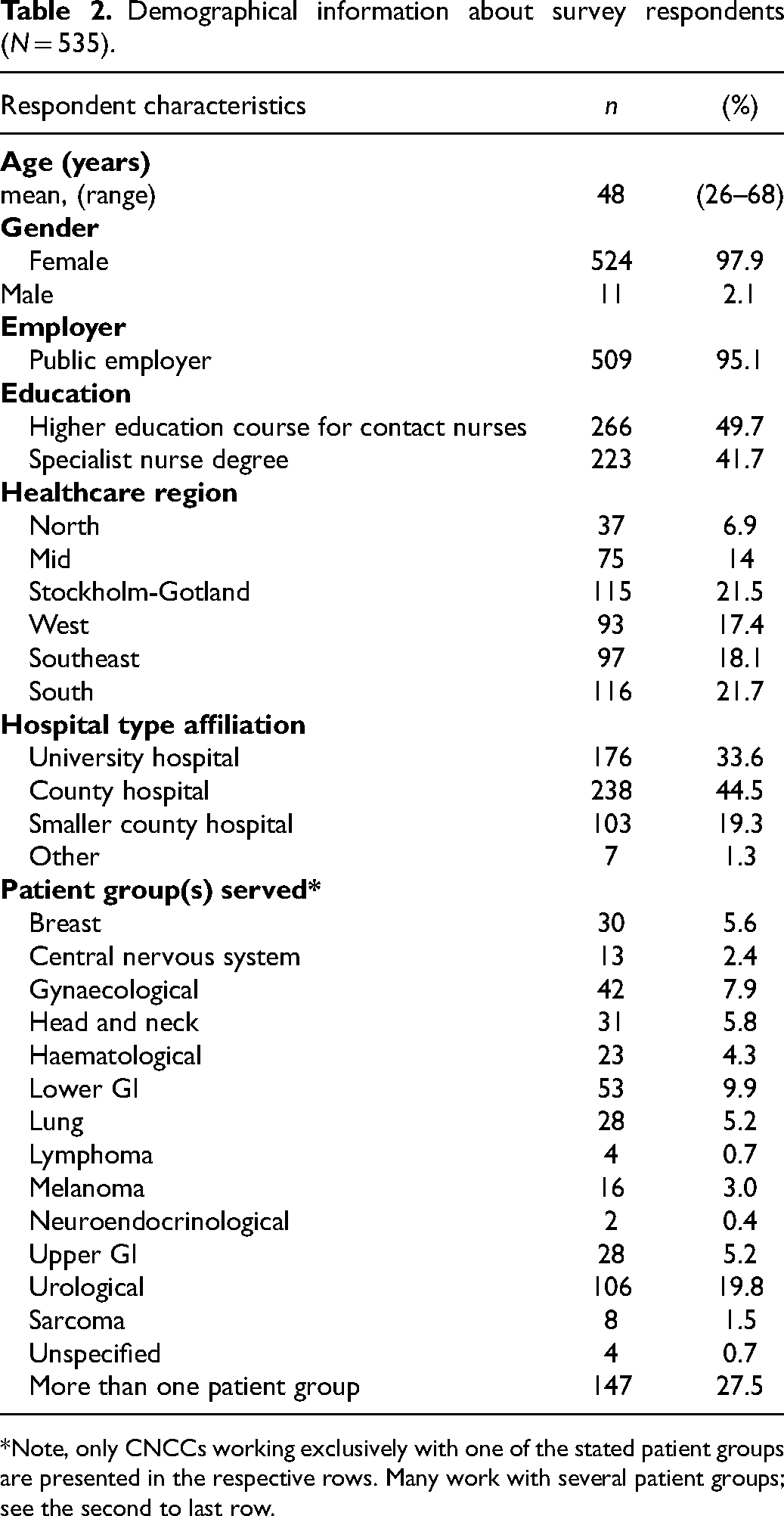
Note, only CNCCs working exclusively with one of the stated patient groups are presented in the respective rows. Many work with several patient groups; see the second to last row.
Contact nursing services in cancer care
CNCCs’ perceptions of the scope of their services are shown in Table 3. The content of CNCC services varied across subgroups and some tasks or aspects of CNCC services were less common than others. For example, only 37.6% agreed that they establish cancer rehabilitation plans, whereas 91.9% agreed to the claim that they inform patients about coming steps in the care trajectory. Three quarters (75.5%) of respondents reported that they participate in multidisciplinary team meetings, but there were large variations across groups of CNCCs. Amongst CNCCs serving patients with breast cancer, 86.7% affirmed to participating in multidisciplinary team meetings, whereas the corresponding value for CNCCs serving patients with melanoma was 38%. Regarding the claim ‘I monitor lead times in coordination with coordinators of the standardized cancer care pathways’, the largest proportion of affirmation was seen amongst CNCCs serving patients with upper gastrointestinal cancers (92.9%), whereas the smallest proportion of affirmation was seen among CNCCs serving patients with haematological cancers (43.5%). CNCCs serving melanoma patients stood out in some respects compared to other groups. For example, only 6.3% affirmed to establishing cancer rehabilitation plans. The smallest variations between subgroups were seen regarding the provision of information about coming steps in the care trajectory (range 76.9–100%) and the provision of psychosocial support to patients (range 75–100%). Differences were less obvious when comparing CNCCs at different types of hospitals, although notably more CNCCs at county hospitals affirmed to establishing cancer rehabilitation plans (40.7%) than CNCCs at university hospitals (24.4%) and smaller county hospitals (31%).
CNCCs’ perceptions of their services: proportion (%) of respondents that agree with the claims fully or to a large extent.
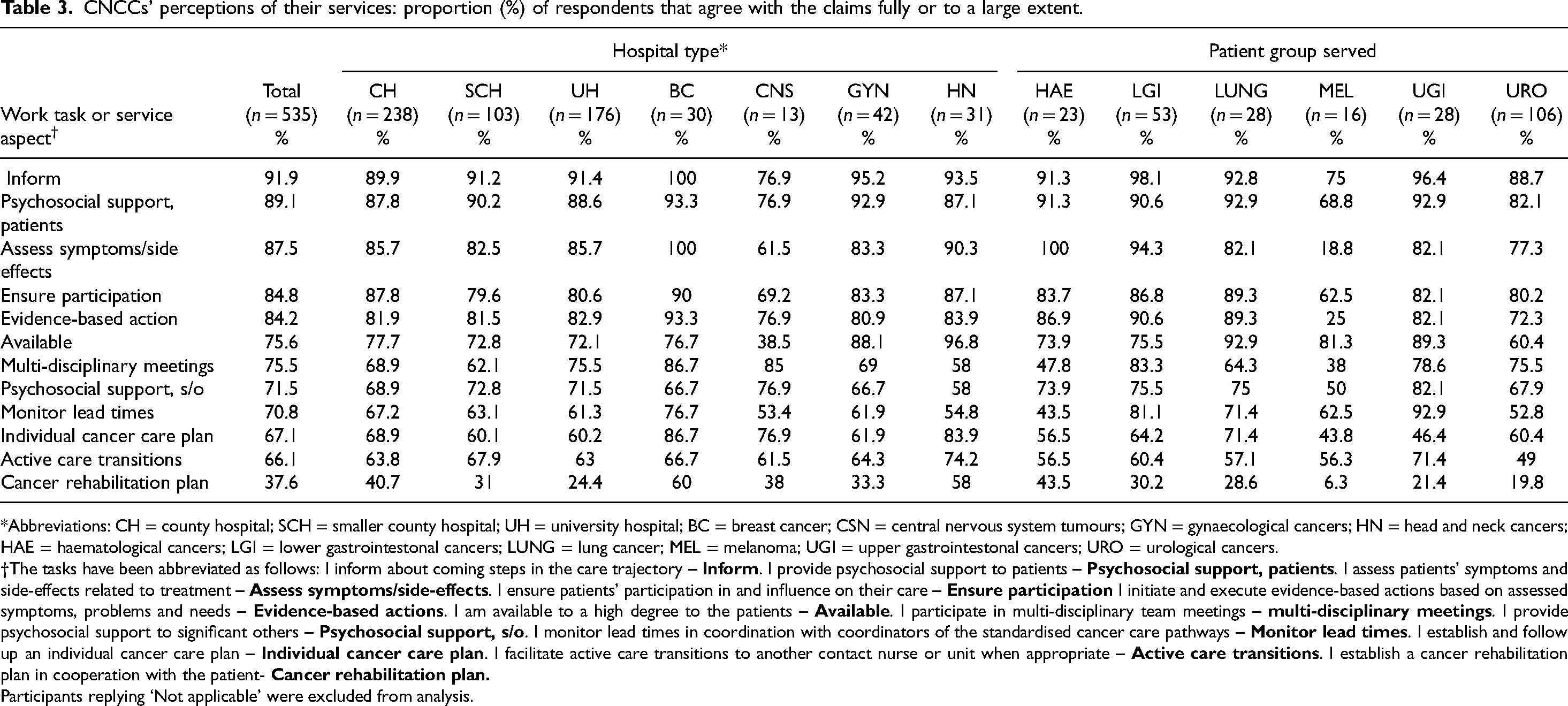
Abbreviations: CH = county hospital; SCH = smaller county hospital; UH = university hospital; BC = breast cancer; CSN = central nervous system tumours; GYN = gynaecological cancers; HN = head and neck cancers; HAE = haematological cancers; LGI = lower gastrointestonal cancers; LUNG = lung cancer; MEL = melanoma; UGI = upper gastrointestonal cancers; URO = urological cancers.
The tasks have been abbreviated as follows: I inform about coming steps in the care trajectory –
Participants replying ‘Not applicable’ were excluded from analysis.
When combining CNCCs’ perceptions of reality and the subjective importance ascribed to tasks (Figure 1), the most prominent deficiencies concerned the establishment of cancer rehabilitation plans and perceived availability. Here, 55% and 50% of respondents, respectively, were categorized into the ‘deficient quality’ group, indicating an imbalance where CNCCs perceive these items to be of great importance to patients, but that they do not perform these tasks to a high degree.
Relationship between perceived reality (PR) and subjective importance (SI) of specific aspects of contact nurse in cancer care (CNCC) services, based on the national description of the CNCC assignment. The index for the two dimensions PR and SI was created accordingly: 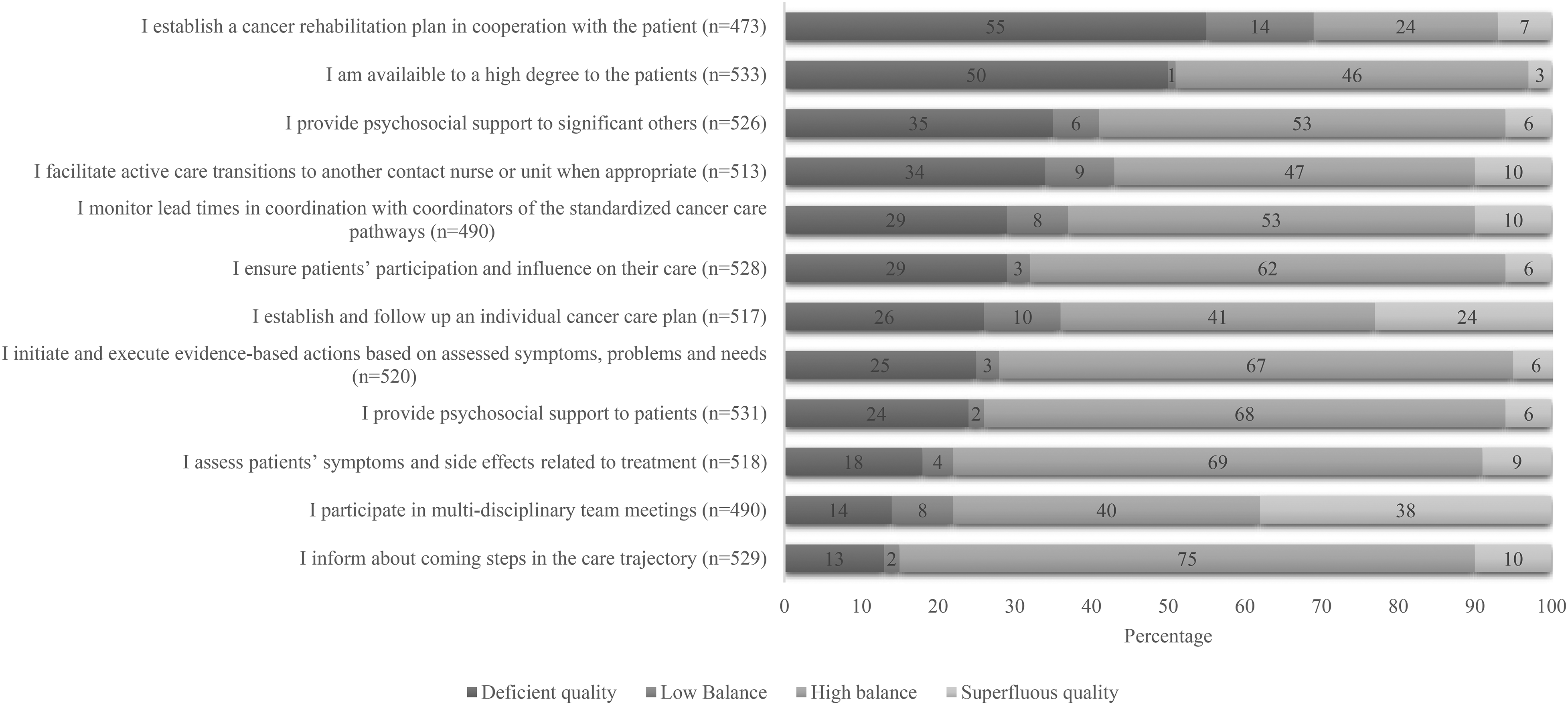
Availability across the care trajectory
CNCCs were asked to state how often they typically had contact with patients at five specified time points across the care trajectory (prior to start of treatment, during treatment, 0–3 months, 3–6 months and 6–12 months after completion of treatment). Half of the respondents (53%) reported typically having contact with patients on one or more occasion at all five time points. A small group of respondents (7.1%) reported typically having contact with patients at only one of the time points. Similarly, 7.9% of respondents reported typically having contact with patients at two time points, 14.6% at three time points and 17% at four out of the five time points. Figure 2 shows how patterns of contact differed across the care trajectory.
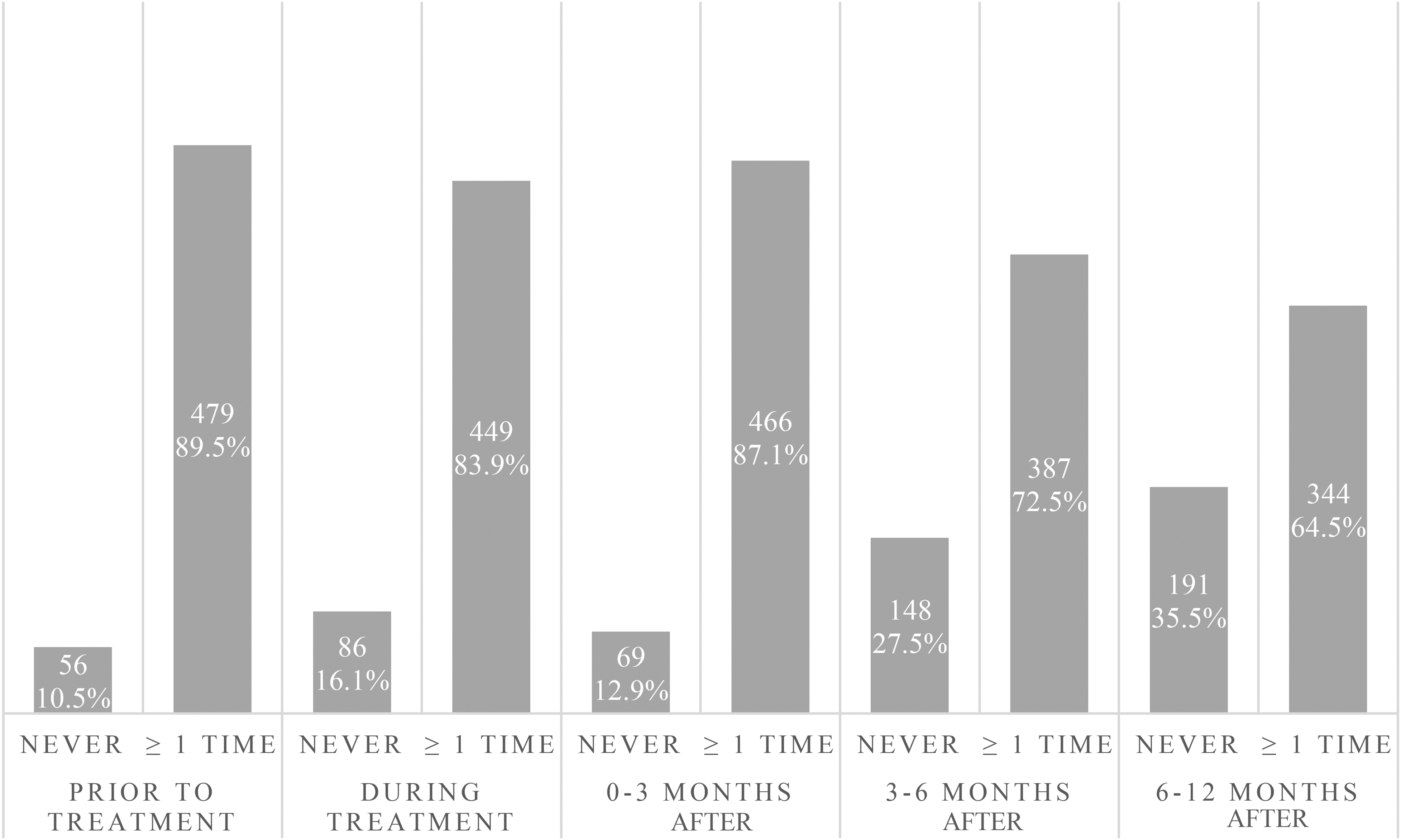
Contact nurse in cancer care (CNCC)’s perceptions of their frequency of interaction with patients across the care trajectory. Interactions are dichotomized as usually having no or ≥1 contact at five specified time points.
Perceptions of organizational prerequisites
Rotated component matrix of exploratory factor analysis (EFA).
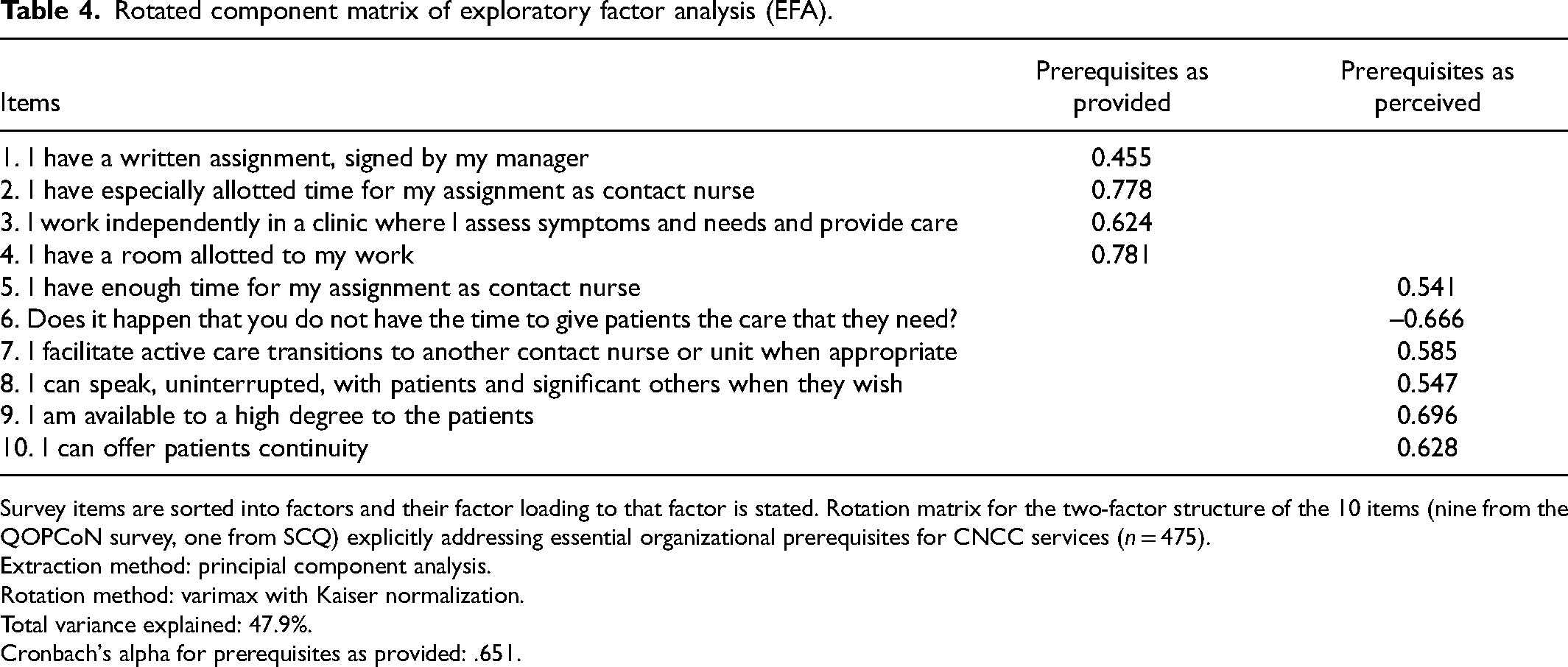
Survey items are sorted into factors and their factor loading to that factor is stated. Rotation matrix for the two-factor structure of the 10 items (nine from the QOPCoN survey, one from SCQ) explicitly addressing essential organizational prerequisites for CNCC services (n = 475).
Extraction method: principial component analysis.
Rotation method: varimax with Kaiser normalization.
Total variance explained: 47.9%.
Cronbach's alpha for prerequisites as provided: .651.
Proportion of respondents (%) in different subgroups of contact nurses in cancer care (CNCC) attributed satisfactory, moderately satisfactory and unsatisfactory organizational prerequisites.
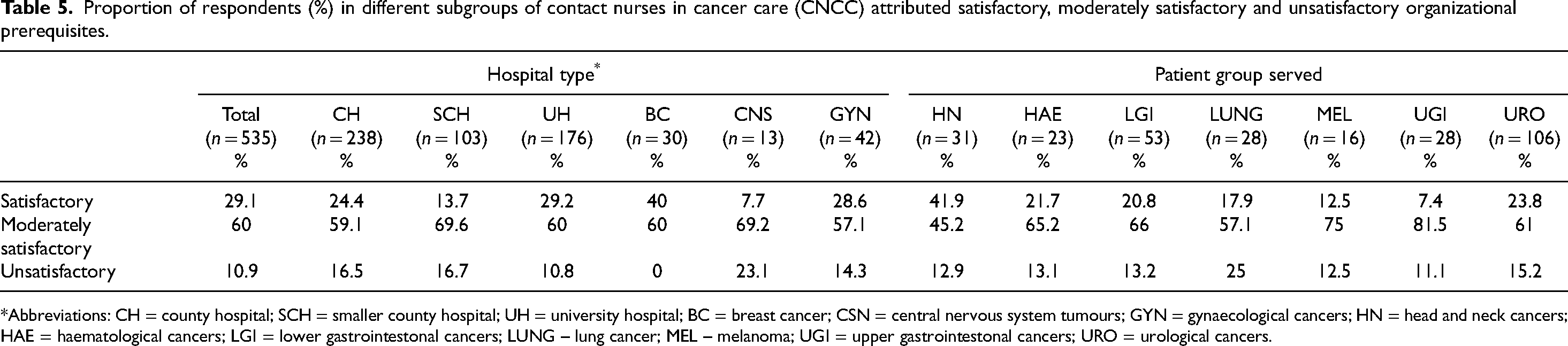
Abbreviations: CH = county hospital; SCH = smaller county hospital; UH = university hospital; BC = breast cancer; CSN = central nervous system tumours; GYN = gynaecological cancers; HN = head and neck cancers; HAE = haematological cancers; LGI = lower gastrointestonal cancers; LUNG – lung cancer; MEL – melanoma; UGI = upper gastrointestonal cancers; URO = urological cancers.
Moral stress and organizational prerequisites
There were statistically significant differences between groups of CNCCs with different organizational prerequisites (satisfactory, moderately satisfactory or unsatisfactory), regarding their perceptions of moral stress, as measured by four SCQ items. The total mean score for the items analysed was 7.3 (SD 5.2) (range 0–23.75). CNCCs who were attributed satisfactory organizational prerequisites reported the lowest scores (mean = 6.0) compared to CNCCs with moderately satisfactory organizational prerequisites (mean = 7.4) and CNCCs with unsatisfactory organizational prerequisites (mean = 8.6) (p = 0.002) (Table 6). There were no statistically significant differences between CNCCs who reported moderately satisfactory or unsatisfactory organizational prerequisites.
Mean self-reported moral stress scores among contact nurses in cancer care (CNCC) with different organizational prerequisites (dependent variable = perceived stress of conscience as defined by four Stress of Conscience Questionnaire (SCQ) items).

Discussion
The main finding from this study is noteworthy variabilities regarding both CNCCs’ perception of their services and their organizational prerequisites. We also demonstrate an association between organizational prerequisites and CNCCs’ perception of moral stress and, to our knowledge, the study is the first of its type to assess CNCC service with such a comprehensive approach.
Regarding services, some tasks from the national description of the CNCC assignment 12 were very common, whereas others, such as monitoring lead times and participating in multidisciplinary team meetings, were less common. We also observed differences regarding practices across subgroups of CNCCs. Clinically relevant differences were most distinct between diagnosis groups rather than between hospital types, but it is important to note that some of the groups were small. When patients are provided with different types of CNCC services depending on their tumour location, this can be described as inequities in care. A certain degree of variability is likely inevitable in any healthcare system, not least a decentralized one, such as the Swedish system. To a certain degree, the CNCC services also need to be dynamic and adaptive to meet the needs of individual patients and the characteristics of different cancer diagnoses. However, too large variations are not something that an ambitious healthcare system, striving towards high-quality equitable care, should accept.
It is possible that some aspects of CNCC services can be sensitive to the specific care trajectory. For example, the structures around multidisciplinary team meetings might differ in a way that can explain the relatively large variation seen in this sample regarding participation in these meetings. It is also relevant to note that previous research has identified that RN can be important actors in the multidisciplinary team meetings, but often have a blurred role.38,39 This may explain why a third of the respondents fell into the ‘superfluous quality’ group regarding this task, indicating that they might not see their place, or are not given sufficient space, in this setting.
Although a certain degree of variation regarding the content of CNCC services across settings might be expedient, it is difficult to justify why CNCCs’ organizational prerequisites should vary. Based on self-reported data, we found that a majority of CNCCs have what we refer to as moderately satisfactory organizational prerequisites. Fifteen percent can be said to have unsatisfactory organizational prerequisites. Previous studies emphasize that there is a connection between quality of care and the organizational prerequisites provided to healthcare providers. 40 These prerequisites are shaped on different structural levels, where not only the closest line manager and the hospital management, but also politicians and decision-makers at a local, regional, national and international level have influence. 41
In this study, CNCCs deemed to have satisfactory organizational prerequisites reported lower levels of moral stress. This is not surprising because the SCQ items utilized to represent moral stress were selected specifically for their connection to the work environment. Nevertheless, it is an important finding, which illuminates the fact that sufficiently organized and resourced care settings are in the interest of both patients and healthcare professionals, affecting their wellbeing and ultimately their ability to provide healthcare services at the top of their capacity. This is why it also is in the interest of healthcare organizations and systems. Moral distress theory 42 emphasizes the importance of organizational support and a positive nurse practice environment, including the opportunity to work autonomously and influence the working environment, in order to curb RN perceived moral stress. Studies have found that the nurse practice environment is an important factor for job satisfaction and retention.43–45 In times of alarmingly low retention rates among RN, the interplay between quality of care and the quality of the organizational prerequisites provided to CNCCs is of great importance for employers to consider.
If unwanted variation in organizational prerequisites has been identified, it is important to seek explanations as to why these variations occur. In this case, we suggest the governance structures surrounding the implementation process of CNCC services could be of interest to review. The Swedish National Cancer Strategy states that everyone diagnosed with cancer should be guaranteed an assigned a healthcare professional and suggest that this role could be attributed to a CNCC. 11 However, that suggestion has not been followed by a structured or formal implementation plan from national or regional governance entities. Little support regarding aspects of both the what and the how has been offered. The term CNCC is being used to describe a multitude of nursing practices within cancer care. For example, continuity and coordination are described as foundational aspects of these services, and achieving these can be considered the very point of introducing this service. 11 Even so, there are RNs with the job description of a CNCC that operate in very isolated parts of the care trajectory. In this study, roughly every third CNCC states that they typically never have contact with patients 3–6 months or 6–12 months after treatment completion. It is worth reflecting on what practices should be referred to as CNCC practices, especially in the context of follow-up, and if a firmer structuring or differentiation could benefit quality-of-care.
In the international movement towards more advanced and autonomous cancer nursing roles, issues regarding mandate, variability and optimization of services are frequently debated.3,8,9,22 Dowling et al. 9 note that the confusion regarding advanced practice nurses’ roles in cancer care results in the conflation and underutilization of RNs’ skills.
In comparison with internationally comparable roles, the CNCC role in Sweden lack formal competency demands, apart from being a RN. Donabedian suggests that formal competency is a dimension of structural quality. 5 Our data indicate that, regarding formal competency, a heterogeneous group of RNs are employed as CNCCs, which is in line with previous research. 46 Approximately half of the sample in our study have completed a degree as specialist nurse or completed a special higher education course for CNCCs. The absence of formal competency demands or certifications for CNCCs makes the Swedish healthcare system stand out in relation to other settings, where the cancer nursing roles have been advancing in recent decades. 9 We suggest a more stringent approach to qualification to add a layer of quality, harmonize practices with internationally comparable roles and further the development of the CNCC role.
Furthermore, the lack of clarity and formalization of the role of CNCCs makes the evaluation of the service more difficult. For managers and decision-makers to be able to understand and prioritize CNCC services, a greater focus on monitoring and evaluating services locally, regionally and nationally is mandated. The current format of CNCC services, where the boundaries and content of the services is not clear cut, makes such evaluation fraught with several difficulties.
Strengths and limitations
Methods
A cross-sectional study design was deemed a suitable method, but the findings from this type of observational study should as always be viewed in the light of the shortcomings of the method, not least regarding an inability to assess causal inference, rather being seen as hypothesis-building. 47
Context and recruitment
Because there is no registry of CNCCs it is not possible to calculate an exact response rate, affecting study validity. An integrative review by ĹEcuyer et al. 48 notes that response rates in nursing research online surveys vary significantly, and that there is no consensus regarding the lowest acceptable rate. The mean response rate of the studies included in their study was 42.46%. In comparison, the present study falls on the lower end, affecting the transferability of the results. However, the sample, consisting of approximately 30% of the total CNCC population, is representative of this population regarding geographical distribution, regional affiliation, hospital type and diagnosis group served. Only one of 21 regions declined participation, which is a strength.
Because healthcare systems and advanced nursing roles in cancer care vary in their shape and form, transferring findings outside of the Swedish setting is discouraged, even if the general issues discussed in the study can be of interest in other settings as well.
A limitation is that CNCCs serving children with cancer were not included. At the time of data collection, the term CNCC was not utilized within the childhood cancer sphere but has subsequently been adopted.
Data collection
Possibly, the fact that most of the data collection occurred during the COVID-19 pandemic might affect the validity of the results in the post-pandemic setting, as CNCCs’ everyday work situation can have been affected. It may also have affected the response rate negatively. Therefore, caution is advised when generalizing the findings from this study.
Statistical analysis
A strength of the study is the fact that it takes a broad approach to CNCC services, addressing different aspects and using different tools to maximize the utilization of the collected data.
It could be considered a limitation in that, because the study only utilized a select part of the SCQ (four out of the original nine items), the results are not comparable to other data sets using this questionnaire.
Conclusion
This study has identified that CNCCs reported varying perceptions regarding their services and their organizational prerequisites. Some aspects of CNCC services described in the national assignment for CNCCs seemed highly prevalent, wheras other aspects were less common. There were also noteworthy differences regarding these issues between CNCCs working at different types of hospitals and caring for different patient groups. Ultimately, these differences may translate into differences in quality-of-care people affected by cancer are offered by their CNCCs.
A majority of CNCCs have what we refer to as moderately satisfactory organizational prerequisites, and we identified a pattern where organizational prerequisites influenced CNCCs’ perceptions of moral stress. Through this, the study highlights the important interplay between quality of care provided to patients affected by cancer and the organizational prerequisites provided to CNCCs that are tasked with supporting them throughout an often challenging and complex care trajectory.
The results from the present study can inform future research regarding this topic. Advantageously, future research could focus on developing ways to measure and compare organizational prerequisites and quality of care fairly and comprehensively for CNCCs in different settings, to benchmark services and promote healthcare improvement. Delving deeper into different aspects of outcomes of CNCC services, by making, for example, a health economic evaluation, would also be a useful contribution.
Supplemental Material
sj-docx-1-njn-10.1177_20571585241290325 - Supplemental material for Contact nurses’ perceptions of their services, organizational prerequisites and moral stress: A cross-sectional study in Swedish cancer care
Supplemental material, sj-docx-1-njn-10.1177_20571585241290325 for Contact nurses’ perceptions of their services, organizational prerequisites and moral stress: A cross-sectional study in Swedish cancer care by Ellen Brynskog, Maria Larsson, Frida Smith, Linn Rosell and Kaisa Bjuresäter in Nordic Journal of Nursing Research
Supplemental Material
sj-docx-2-njn-10.1177_20571585241290325 - Supplemental material for Contact nurses’ perceptions of their services, organizational prerequisites and moral stress: A cross-sectional study in Swedish cancer care
Supplemental material, sj-docx-2-njn-10.1177_20571585241290325 for Contact nurses’ perceptions of their services, organizational prerequisites and moral stress: A cross-sectional study in Swedish cancer care by Ellen Brynskog, Maria Larsson, Frida Smith, Linn Rosell and Kaisa Bjuresäter in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We express our gratitude to all survey respondents for the time and effort they invested. The support of Jari Appelgren in the statistical analysis of this research paper has been invaluable. Katarina Graah-Hagelbäck provided valuable support in reviewing the language in this paper.
Data availability statement
The individual participant data that underlie the results reported in this article, are, after deidentification (text, tables, figures, and appendices), available from the corresponding author, EB, to researchers upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been funded by the Regional Cancer Centre South, the Regional Cancer Centre Stockholm-Gotland and the Regional Cancer Centre West.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.