
Abstract
The aim of this study was to explore registered nurses’ experiences of non-nurses being involved in nursing care of hospitalised patients at a Danish university hospital. A total of 16 registered nurses from 12 different inpatient wards where non-nurses were employed (employees without a nursing education) participated in five focus groups. The data were examined using thematic analysis. This article followed the COREQ guidelines. Three themes were generated: (1) balancing support: RNs’ experiences with non-nurses in indirect and direct nursing care; (2) managing complexity: RNs’ experiences with delegating nursing care to non-nurses; and (3) navigating responsibility: RNs’ experiences with coordinating patient care amidst non-nurse involvement. Replacing registered nurses with non-nurses makes delivery of nursing care complex. On the one hand, involving non-nurses in the delivery of indirect nursing care eases nurses’ workloads and releases time to spend with patients. Furthermore, quality of care can be improved if the competencies of the non-nurses’ match patients’ care needs. On the other hand, the involvement of non-nurses in direct nursing care complicates nurses’ delegation practice and causes uncertainty about their nursing role.
Background
Across the world, ageing populations and the increasing prevalence of individuals with multimorbidity have increased the pressures on healthcare systems. 1 Hospitalised patients often have complex care needs that require highly specialised nursing care.2,3 At the same time, healthcare institutions face a nursing shortage crisis due to an ageing workforce approaching retirement, few younger registered nurses (RNs)4–6 and RNs leaving the profession due to the increased pressure on healthcare systems.7–9 In 2022, the global workforce shortage was estimated to amount to 5.9 million nurses, a situation that worsened during the COVID-19 pandemic.4,10 Low job satisfaction and burnout among RNs are closely related to job stress, patient–nurse ratios and patient satisfaction. 11 Although preventive actions related to leadership, work environment and professional growth have been taken to keep RNs in the profession, the shortage has increased, 12 and requires healthcare systems to consider how to secure high-quality nursing care and patient safety. 13
Traditionally, patient care has been delivered by multidisciplinary teams that combine different bodies of knowledge and expertise. 14 However, due to the shortage of RNs, there is a need to increase and improve multidisciplinary collaborations to be able to use the available nursing skills more effectively. 15 In clinical settings, this has led to employment of allied health professionals and unregulated workers (all referred to here as non-nurses) in RN positions as a substitution for RNs. Allied health professionals are professionals with a health education but not a nursing education. Unregulated workers are employees without a health-related education. Having patient care and treatment delivered by a multidisciplinary team is common.14,16 However, employing non-nurses as a substitution for RNs in the delivery of nursing care has not been done to a significant extent thus far. Previous studies describe that higher numbers of qualified RNs per patient17–19 and more nursing hours per patient 20 lead to better patient outcomes, including length of stay, ulcer, pneumonia, urinary tract infection and mortality. Therefore, the presence of RNs is essential for patient outcomes.
The development in staff composition towards fewer RNs and more non-nurses involved in delivering nursing care entail altered working conditions for RNs and necessitate rigorous consideration of how to ensure high-quality care and patient safety. The implications of non-nurses being employed in RN positions have not yet been explored. To ensure high-quality nursing care, it is imperative to learn from RNs’ experiences of working with non-nurses. Therefore, this study explored RNs’ experiences of non-nurses being involved in nursing care to hospitalised patients at a Danish university hospital.
Methods
The study was designed as a qualitative focus group study, and is reported in accordance with the Consolidated criteria for reporting qualitative research (COREQ). 21
Setting
The study was conducted at a Danish university hospital. At the time of the study, non-nurses, including physiotherapists, occupational therapists, dieticians, pharmaceutical technical assistants, hospital porters, cleaners and service assistants, were part of the inpatient ward staff. Due to difficulties in recruiting RNs or nurse assistants, non-nurses held positions previously filled by these two types of staff. The hospital's management implemented this change to optimise the allocation of limited nursing resources to tasks exclusively within RNs’ scope of practice and assigned non-nurses to tasks for which they possessed overlapping skills with RNs. The intention was to establish clinical teams that could provide safe and high-quality care to patients. The wards’ nurse managers decided which type of non-nurses to include in the clinical teams on each ward.
Participants
Nurse ward managers of inpatient wards were contacted via email and informed of the study in April and May 2022. RNs from the inpatient wards that had employed at least one of the above-mentioned non-nurse staff could participate in the study. Eligible participants were RNs in permanent positions who had experience working with non-nurses on the ward. There were no exclusion criteria regarding gender, age and length of employment.
Data collection
Focus groups were conducted to gain insight into RNs’ experiences with the changed staff composition and of non-nurses being involved in delivering nursing care to hospitalised patients. Focus groups allowed for the exploration of multiple perspectives, including similarities and differences in the participants’ experiences, as data were generated from the interactions in the groups where the RNs stimulated and challenged their experiences, perceptions and beliefs.22,23
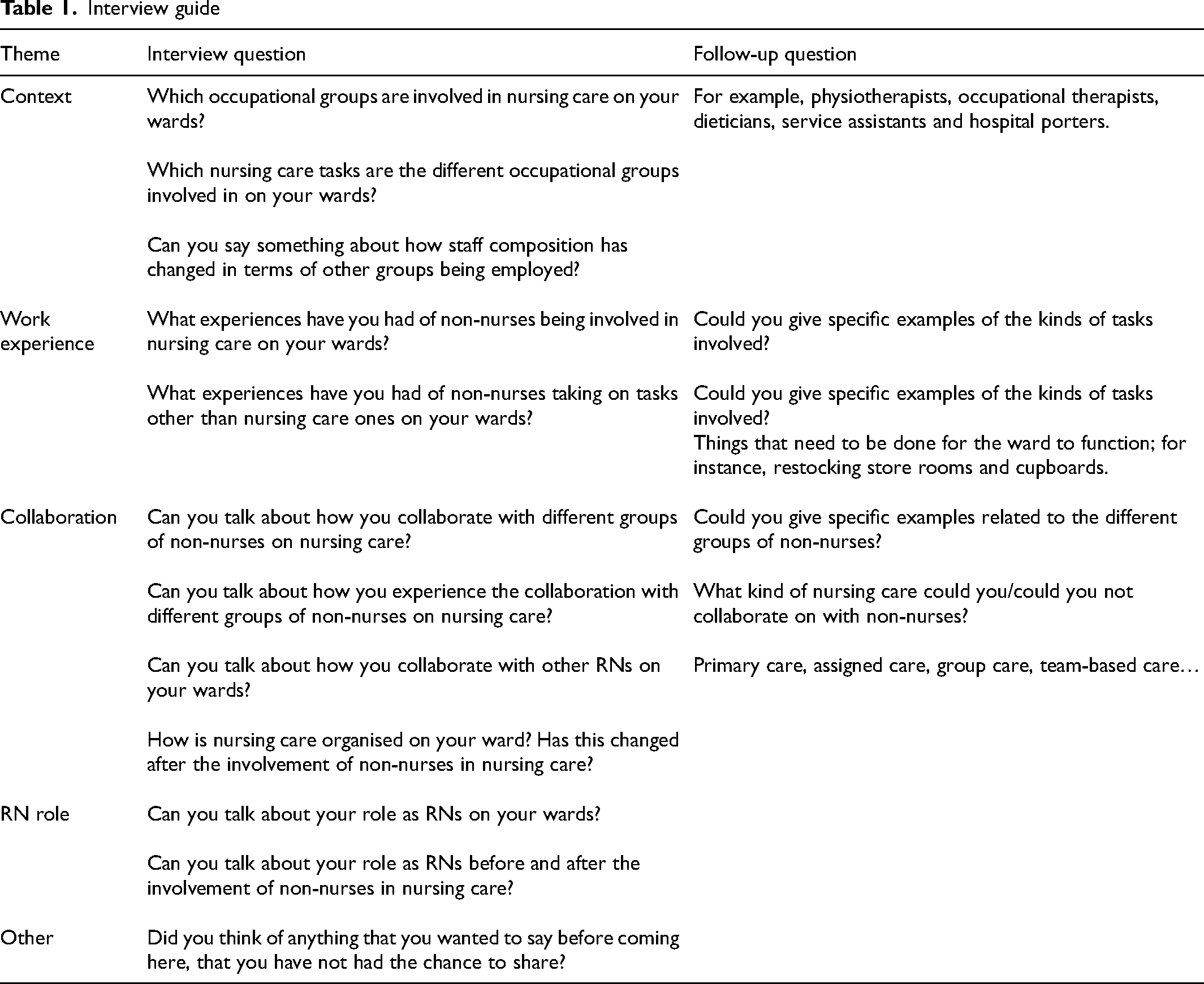
In total, 16 RNs participated in five focus groups between August and October 2022. There were 2–5 participants in each group. The focus groups lasted 69–73 min. Two researchers facilitated the focus groups; one moderated the group discussion, while the other one observed the interactions among the participants. The researchers were known by most of the participants as they were employed at the same university hospital but not at the same ward. A semi-structured interview guide was used to guide the focus groups (Table 1).
Interview guide
Data analysis
The data were analysed using thematic analysis, 24 which involved a non-linear process with six phases. In phase 1, the interviews were transcribed, read and reread several times by all the authors. Phase 2 consisted of the generation of initial, open codes by all the authors. In this phase, the data were organised into meaningful groups by two researchers (the first and last authors). In phase 3, the search for relationships among the coded data began, and initial themes emerged. This was a back-and-forth process where the work of the first and last authors was discussed by the research group, followed by revision by the first and last authors until the coded data were meaningfully clustered. Finally, in phases 4 and 5, the themes were reviewed, defined and named primarily by the first, second, second-to-last and last authors. This was also an iterative process during which the themes were discussed and described, and quotes were selected to represent the essence of each theme. In phase 6, the final analysis was described in the three themes presented below.
Ethics
The participants were provided with written and oral information about the study before giving their written consent. They were informed that participation was voluntary, and they were guaranteed anonymity as well as the possibility to withdraw from the study at any time without explanation or consequence. The study was carried out in accordance with the Code of Ethics of the World Medical Association, 25 and it was approved by the regional Danish Data Protection Agency (ID F2022-085). A secure data storage system was used, and only the research group (all authors) had access to the data.
Results
A total of 16 RNs working at 12 different surgical and medical inpatient wards participated in the focus groups (Table 2).
Participants’ characteristics.
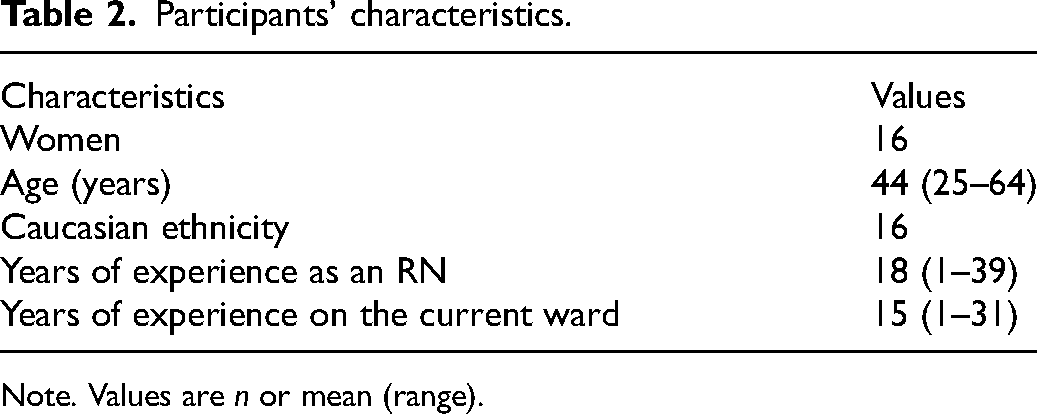
Note. Values are n or mean (range).
The thematic analysis led to the following three themes: (1) balancing support: RNs’ experiences with non-nurses in indirect and direct nursing care; (2) managing complexity: RNs’ experiences with delegating nursing care to non-nurses; and (3) navigating responsibility: RNs’ experiences with coordinating patient care amidst non-nurse involvement. These themes illustrate different dimensions of the complexity related to non-nurses being involved in delivering nursing care to hospitalised patients.
Balancing support: RNs’ experiences with non-nurses in indirect and direct nursing care
This theme describes how RNs experienced being supported by non-nurses in both direct and indirect nursing care. The RNs emphasised that non-nurses sometimes undertook tasks traditionally performed by RNs but not directly related to patients. For example, hospital porters ensured that cabinets in patients’ rooms and storage rooms were adequately stocked, cleaning staff ordered supplies such as bandages and utensils, and service assistants delivered samples or picked up medical equipment from other hospital wards. These tasks were described as practical tasks carried out ‘one step away’ from the patient. One RN said: ‘These practical tasks are somewhat separate from the patient. They are not close to the patient, but one step away from them. Still, it's really important that these things are in order for us to provide good care to the patients.’ (RN5, focus group 1)
Having non-nurses undertake practical tasks ‘one step away’ from patients was described by some RNs as indirect care, which contributed to the overall functioning of the ward and served as a prerequisite for the delivery of nursing care. In another focus group, an RN said the following about a service assistant: ‘She helps with everything, and we immediately notice it when she is not there. She restocks. She cancels. She does all kinds of things that are completely unimportant in relation to the patient but that make everything around the patient function.’ (RN2, focus group 3)
As a result of the work performed by the service assistant, time was released for the RNs to focus on other things. The RNs explained how non-nurses were also involved in direct nursing care by highlighting that hospital porters excelled at involving the patients’ physical resources during mobilisation. Pharmaceutical technical assistants reacted on the potential interactions among active ingredients when administering patients’ medications. Physiotherapists improved patients’ mobilisation and lung physiotherapy, and dieticians performed nutritional screenings and provided individualised nutrition plans. As one RN said: ‘Our dietician – she is the one who has these conversations with the patients, and she is the one who takes care of their actual nutritional problems. She weighs them, and she handles all the things [in this domain] that we [the RNs] used to do.’ (RN1, focus group 3)
The care delivered was perceived to improve when the competencies of the non-nurses aligned with the specific care needs of the patients. According to the RNs, the non-nurses could concentrate on specific patient needs or problems: ‘It really raises the level. It's more than we could do ourselves because we have so many other [patients]. They get to choose the ones [patients] … and then they work with them’ (RN5, focus group 1). In contrast, the RNs described how they often had to prioritise their delivery of care as they were responsible for many patients and had to ensure that all their care needs were met. The RNs emphasised that the non-nurses’ delivery of selected and defined caring tasks increased the quality of specific areas of care. However, this did not result in released time for the RNs to deliver nursing care.
Overall, the RNs valued the non-nurses’ involvement in indirect nursing care as their management of practical tasks was perceived to release time for RNs to focus on patients. The complexity increased when non-nurses became involved in direct nursing care. On the one hand, when they delivered care that matched their competencies, this improved the quality of patient care. On the other hand, this was not perceived to ease RNs’ workloads.
Managing complexity: RNs’ experiences with delegating nursing care to non-nurses
This theme unfolds how the RNs’ experienced the delegation of nursing care to non-nurses as a complex matter. This complexity was primarily related to having to balance the non-nurses’ competencies with the patients’ needs. The presence of non-nurses in the wards contributed to an increased awareness of the professional competencies of the different types of non-nurses. Working together as colleagues at the wards facilitated the involvement of non-nurses in nursing care. One RN said: ‘We have many old patients who come in with a fever. In the past, 2, 3 or 4 days went by during which their functional levels deteriorated before the physiotherapist actually came and saw them. Now, she [the physiotherapist in the ward] is on them from the start and gives them PEP [positive expiratory pressure] whistles.’ (RN3, focus group 1)
The easy access to non-nurses and their competencies often enabled prompt responses to specific patient needs. According to the RNs, this often prevented the development of further health problems. However, the RNs emphasised that this only occurred when there was an alignment between the competencies of the non-nurses and the patients’ care needs. Regarding all aspects of nursing care, the RNs said that the competencies of the non-nurses sometimes fell short and that this increased the complexity of delegating nursing care. Reflecting on collaboration with non-nurses during evening shifts, one RN said the following: ‘It actually didn’t work out … They wanted it to be physios and nothing else. So, it just became too narrow, and it didn’t work in practice. Anyway, if you want to have a physio [during the evening shift], it should be because they also take on other tasks.’ (RN2, focus group 3)
According to the participants, collaborating with non-nurses during shifts was generally difficult. Due to low staff levels, it was pivotal that the non-nurses’ competencies were aligned with the patients’ care needs. Consequently, non-nurses primarily worked during the daytime on weekdays. However, even during these times, the delegation of nursing care was reported as being complex and challenging. One example of these challenges is the multifaceted nature of nursing care activities, which made it difficult to divide them into smaller, specific tasks that could be delegated to non-nurses. One RN illustrated this issue with the following quote: ‘If she [the physiotherapist] only lifts the patient up to sit on the side of the bed or walks her to the bathroom, I still have to go in and wash her. Then, I have to leave the patient for the physiotherapist to come back and walk the patient back [to the bed].’ (RN2, focus group 5)
Delivering multifaceted and interconnected nursing care activities was necessary to adequately meet patients’ needs. Therefore, the RNs expressed concerns that nursing care could become fragmented if they only delegated nursing care activities matching the non-nurses’ competencies. Despite this concern, they reported delegating specific elements of nursing care that matched non-nurses’ areas of expertise to make the best use of their competencies. For some RNs, managing this complex collaboration was an ongoing process. ‘In our ward, this is something we practice all the time – finding the tasks that are right for them [non-nurses]. We have decided that the early warning score [monitoring of vital signs] is a task they need to take on because we need help with that.’ (RN1, focus group 5)
In some situations, the RN's had to delegate care activities that exceeded the non-nurses’ competencies. One example was having non-nurses use the early warning score system. Some RNs described this as helpful, while others were sceptical about it. They were concerned that it could potentially compromise the quality of care if non-nurses were not sufficiently trained. They highlighted that the system in question required more than just recording vital signs on paper; specialised knowledge about how to interpret the signs and respond appropriately was also necessary. The RNs explained that they felt obligated to prepare the non-nurses for the delegated nursing care. Some of them created specific paper-based tools to support an accurate information flow between the non-nurses and the RNs. ‘We have a service assistant. She has a cart with treats and she offers food. It is my task to check if there's anything she has to be aware of. If someone has diabetes or if someone is not allowed to eat. I have a small piece of paper where I write specific points of attention.’ (RN1, focus group 4)
The RNs described making preparations to make sure that non-nurses could manage care activities that went beyond their areas of competence. They also felt obliged to follow up on the nursing care provided by non-nurses. They underlined that certain care activities could be quite complex, even though they appeared basic and easily delegable. ‘Our patients with neurological conditions don’t sit on the side of the bed while eating. However, for the service assistants, the bedside table is the right place to put the tray, even though they [the patients] have a disability-friendly table that they must sit at. It means a lot to their general rehabilitation that they get up and sit properly for their meals.’ (RN1, focus group 2)
In these situations, collaborating with non-nurses who lacked nursing competencies was experienced as problematic because insufficient attention to the complexity inherent in nursing care and the patients’ conditions could compromise the quality of care. Although the RNs acknowledged the need for assistance from non-nurses, they said that delegating could be time consuming. One RN gave the following example: ‘I might as well do it myself. If I have to explain it to you [non-nurse] first, then it's actually easier if I just give the protein drink myself, or whatever it is’ (RN 2, focus group 4). In some cases, delegating care to the non-nurses became so complicated that RNs found it easier to perform the care activities themselves.
Navigating responsibility: RNs’ experiences with coordinating patient care amidst non-nurse involvement
This theme shows how the RNs perceived the overall coordination of patient care to be their responsibility. The involvement of non-nurses in delivering nursing care seemed to challenge the RNs ability to fulfil this responsibility, and they were challenged in grasping a changed and undefined nursing role. In all the focus groups, the RNs explained that they were primarily responsible for overseeing care on the wards. They also said that this was an expectation indirectly placed on them by the non-nurses. ‘You are the coordinator ... They [the non-nurses] carry out tasks in specific [areas], and what they do is really, really good … But they can just leave the patient. I feel that I am the one who has the whole responsibility.’ (RN 3, focus group 1)
The RNs argued that they were responsible for the full overview of the patient's situation as well as for coordinating their care, in contrast to the non-nurses, who primarily assumed responsibility for specific aspects of patient care. However, the RNs found it difficult to uphold their responsibilities when aspects of care were delegated to the non-nurses. As one of them explained: ‘Well, for example, when you do ward rounds, and the physician asks about the patient's breathing – how he is feeling today. Honestly, you’re saying, Well, I actually haven’t managed to meet the patient, but I haven’t heard from the one out there [non-nurse], so I assume everything is okay.’ (RN 1, focus group 4)
Not being fully informed about patients’ conditions during ward rounds put the RNs in a precarious position, which led to concerns about potentially overlooking important details. ‘We really want to handle it [nursing care] and do it independently and all that. Because then we are in control. Well, when there are many people [non-nurses] involved, it feels like you lose control a little.’ (RN5, focus group 1)
Several RNs described how this situation was linked to delegating care activities, which forced them to rely on non-nurses. Furthermore, they highlighted how obtaining comprehensive pictures of patients’ conditions was difficult when follow-ups on delegated care were fragmented and failed to address the entirety of patients’ problems and situation. The RNs questioned their ability to be responsible for overall patient care when communication regarding patients’ information relied on different non-nurses who did not always possess the knowledge and competencies necessary for deciding what must be reported back. Moreover, the RNs described that they had taken on new responsibilities. They felt obliged to support the non-nurses because they lacked nursing training, which could create challenging situations that were difficult the non-nurses to manage. ‘She [the non-nurse] had never seen a dead person before. You know, she totally broke down, and I felt so sorry for her. In some situations, she has been under pressure, and she has not been prepared for it. … There was also a patient who really scolded her. “I will not go back in there.” She was really upset, and that was okay. But as a nurse, you have to learned how to care also for the difficult patients. She has taken so many hits due to not being a nurse.’ (RN1, focus group 1)
As part of their new responsibilities, the RNs described looking after the non-nurses’ well-being on the wards. Furthermore, they felt accountable for the care delivered by the non-nurses when the care activities exceeded their competencies. In the focus groups, discussions about these situations facilitated reflections on the legal aspects associated with delivering nursing care. ‘If my nurse assistant colleague is with the patient and makes a mistake or doesn’t react to a low blood-glucose level or something, then it's due to her authorisation – it's not my responsibility. However, it becomes challenging when you deal with other staff, who are not trained [within nursing] … If mistakes are made, who is then responsible?’ (RN2, focus group 4)
The RN's expressed a strong sense of obligation to safeguard the quality of care at the hospital and ensure patient safety. The complexity of delegating care activities to non-nurses with or without competencies that matched patients’ needs could compromise the RNs’ sense of whether adequate nursing care was being delivered. Some of them described that the involvement of non-nurses in nursing care made them concerned about the compromises they would have to make. One RN explained: ‘Well, I think it means something – in the sense that I don’t get to do everything myself … I think that I’m ready to say, “Well, we have to be nurses in a different way.” I will not compromise nursing care, but I must think about working differently. What is important for me is being able to work so that nursing care isn’t split up into pieces but can continue to function as a whole.’ (RN5, focus group 1)
The participants realised that the delivery of nursing care was changing, and they described how collaborating with non-nurses impacted their role. They acknowledged that being supported by non-nurses could be a partial solution to nurse shortages. However, this collaboration challenged their traditional understanding of the nursing role and called for ongoing consideration of the complexities it entailed.
Discussion
This study aimed to explore RNs’ experiences of non-nurses being involved in nursing care of hospitalised patients at a Danish university hospital. Its findings make an important contribution to the knowledge of the complexities that arise when involving non-nurses in the delivery of nursing care to hospitalised patients.
The findings show that RNs experienced non-nurses to be involved in both indirect and direct nursing care. In the former, non-nurses carried out tasks not directly related to patients, which have usually been performed by RNs. The description of indirect nursing care activities more or less aligns with the definition of non-nursing tasks, which are tasks performed by RNs that do not require a nursing education 17 or fall below an RN's skills level. 26 This definition implies that there is a clear boundary between activities that require nursing training and those that do not. 27 Such a boundary was not evident in the present findings. Non-nurses’ involvement in indirect care was perceived as helping the delivery of nursing care because it supported the overall functioning of the wards. A qualitative interview study by Grosso et al. 28 found that RNs disagreed with the concept of non-nursing tasks. The nurses in that study argued that nursing care cannot be reduced to a predefined set of tasks. Instead, they highlighted the notions of being ‘inside’ or ‘outside’ the nurse's role, and they argued that RNs are outside such a role when they undertake activities that could be performed by other health professionals or unregulated workers. 28 This view seems in line with the opinions of the RNs in the present study regarding non-nurses’ involvement in indirect nursing care. Non-nurses carried out activities that were outside the nurse's role, which increased the efficiency of the ward and released time for the RNs to provide direct nursing care. When involving non-nurses in the delivery of nursing care, there is a risk that nursing care may become fragmented and task-oriented, potentially leading to unethical and unprofessional nursing care. This approach may result in patients not receiving person-centred care as their physical, psychosocial and relational needs are not considered holistically. 29
Our findings show that non-nurses were seen as delivering high-quality care when their competencies matched the patients’ needs. This can be explained by the presence of a scope-of-practice overlap in the involved professions. 30 A scope-of-practice overlap implies that no single profession holds exclusive rights to specific clinical knowledge, skills or tasks, which allows many activities to be safely and effectively performed by different professions. 30 This may explain why the RNs experienced that non-nurses helped to prevent the development of further health problems in patients – because they shared or supplemented the RNs’ knowledge and skills. However, overlapping scopes of practice may also lead to uncertainty regarding the boundaries of each profession.30,31 This seems to be the case in our study; the RNs had become unsure about their nursing role. This issue calls for mutual engagement and a shared understanding of the scopes of practice among all the involved professions, as well as agreement on the areas of overlap. 31 Mutual engagement is pivotal to ensure that the collaborative efforts of RNs and non-nurses are driven by patient-centred care rather than the interests of individual professions. 30 Despite the scope-of-practice overlap, RNs encountered challenges when non-nurses were assigned to evening and night shifts. Reduced staff levels during these shifts required staff members to possess wide-ranging competencies to meet all the needs of patients. This indicates that there may be a threshold in the ratio of RNs to non-nurses when staffing wards, as evidenced by the fact that non-nurses at the hospital in question worked primarily during the daytime on weekdays. Further research is needed to determine the optimal RN to non-nurse ratio on hospitals wards and identify the factors influencing this ratio.
The present study showed that the RNs saw themselves as the ones responsible for coordinating patient care, as non-nurses only took on specific aspects of such care. Although the RNs did not label the specific care model adopted on their wards, this could be defined as team based. Team nursing is a well-established care model in which a group of nursing staff with different educational levels (skill mix) share the responsibility for caring for a group of patients. 32 Team nursing and delegation are intertwined as RNs must delegate nursing care to team members so that the right care is accessed at the right time; this ensures that patient needs are met. 33 In the hospital we investigated, involving non-nurses in team-based nursing complicated the delegation of direct nursing care. Delegating became time consuming because the RNs felt responsible for preparing non-nurses and following up on delegated activities. In general, delegation involves transferring responsibility for a task from the delegator to the delegatee. In the healthcare sector, the delegator retains overall accountability for the decision to delegate and they must ensure that the delegatee has the competencies to deliver the required care. 33 This emphasises RNs’ responsibility, as delegators, to supervise non-nurses. The RNs in the present study reflected on the legal aspects of delegation, but they seemed unsure about the allocation of accountability if non-nurses made errors while providing nursing care. Reviews on RNs’ delegation practice to assistant nurses 34 and unlicensed workers 33 have highlighted the underdeveloped nature of delegation skills among RNs, and they have recommended education and training in efficient delegation practices. It is important to note that the delegation skills of the RNs in this study remain unknown, but it might be relevant to address this aspect when integrating non-nurses into the wards’ staff. Furthermore, the impact of delegating nursing care to non-nurses on patient outcomes is unknown as only the RNs’ perspectives were explored. Research on delegation practice states that there is a lack of evidence regarding its impact on patient outcomes. 33 However, this study suggests that patient safety may be compromised if nursing care is delegated to non-nurses who lack the necessary competencies. To gain a deeper insight into the complexities of delegation, further research is needed on the relationships between RNs’ delegation practices, the individuals assigned care activities (e.g. non-nurses), and patient outcomes and experiences. Acquiring this knowledge is crucial for developing skills or methods that support efficient delegation without compromising patient safety.
The findings of the present study are important as a systematic review of the factors contributing to the shortage of nurses found that increased workloads, unfavourable working conditions and lack of support can lead RNs to consider leaving their positions. 2 Therefore, involving non-nurses as ward staff seems to create a paradox. On the one hand, doing so addresses nurse shortages; on the other hand, it risks exacerbating such shortages if it contributes to RN turnover. This study can inform hospital managers’ decisions on how to organise and support the staffing of wards when this involves skill mix from outside the nursing profession.
Strengths and limitations
This study has some strengths and limitations. The study was conducted at a single Danish university hospital, which may limit the generalisability of the findings to other hospital settings. However, a considerable strength of the study is the inclusion of 16 RNs with extensive work experience (mean: 18 years), employed on 12 different surgical and medical wards. This heterogeneous sample provided nuanced insights into RNs’ experiences, in accordance with the study's aim. The use of five focus groups with different numbers of participants (range of 2–5) could be considered a limitation, as it is recommended that focus groups consist of 5–8 participants to support group discussion. 23 Each focus group was initially planned with five or more RNs, but cancellations on the day of the session due to sickness among the ward staff or an increased number of acutely admitted patients resulted in lower attendance. Therefore, the low number of participants may be a consequence of the nursing shortage at the hospital. Furthermore, while the study focused on RNs’ perspectives, it could have been enriched by conducting interviews with ward managers, non-nursing staff and patients to gain a comprehensive understanding of the impact of involving non-nurses in nursing care. This would have provided valuable insights into the experiences of different stakeholders.
Conclusion
Involving non-nurses in nursing care seems inevitable due to the global shortage of RNs. However, doing so is a complex matter, and there is ambiguity regarding its advantages and disadvantages. On the one hand, involving non-nurses may lead to a reduction in RNs’ workloads, and it may give RNs more time to provide direct nursing care to patients. Furthermore, involving non-nurses has the potential to improve the quality of care if their competencies match patients’ care needs. On the other hand, the involvement of non-nurses in direct nursing care can complicate RNs’ delegation practices and cause uncertainty regarding their nursing role. This can potentially compromise the understanding of nursing as being founded on having an overview of each patient and their care needs. The findings of this study call for paying attention to RNs’ roles and delegation practices as well as to the solutions for organising and supporting the collaboration between RNs and non-nurses to ensure the best possible care for patients.
Footnotes
Author contributions
CRediT authorship contribution statement: Helle Enggaard: Conceptualization, project administration, methodology, data collection, data analysis, writing – original draft, review & editing. Britt Laugesen: Conceptualization, methodology, data collection, data analysis, writing – review & editing. Karin, Bundgaard: Conceptualization, methodology, data collection, data analysis, writing – review & editing. Kathrine Hoffmann Kusk: Conceptualization, methodology, data analysis, writing – review & editing. Helle Haslund-Thomsen: Conceptualization, methodology, data collection, data analysis, writing – review & editing. Sara Jacobsen: Conceptualization, methodology, data collection, data analysis, writing – review & editing. Siri Lygum Voldbjerg: Conceptualization, methodology, data collection, data analysis, writing – review & editing. Birgitte Lerbæk: Conceptualization, project administration, methodology, data collection, data analysis, writing – original draft, review & editing.
Acknowledgments
We want to thank all the participating RNs for participating in this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.