
Abstract
Nursing staff's pressure ulcer (PU) prevention knowledge in long-term older people care (LOPC) varies. In particular, more evidence is needed to improve the knowledge of nursing staff with a lower level of education with context-tailored interventions. The aim of this study was to evaluate the impact of intervention on nursing staff's PU prevention knowledge. The intervention, a consistent PU prevention practice for nursing staff based on international guidelines, was developed and implemented using the OMEBP model. The data were collected in two LOPC facilities from 253 registered and practical nurses using the Pressure Ulcer Prevention Knowledge test. In the intervention facility, knowledge improved in three PU prevention areas and in the total sum. Context-tailored PU prevention practice interventions focusing on nursing staff in LOPC facilities should be developed and these aspects should also be included in lower-level nursing staff's education.
Keywords
Background
Nursing staff's knowledge has a fundamental role in evidence-based prevention of pressure ulcers (PUs) and in diminishing the suffering and costs caused by PUs. Research evidence has shown that a prerequisite for high-quality PU prevention is professionals/nursing staff with sufficient knowledge about it. 1 However, earlier studies have indicated a need to strengthen knowledge around PU prevention. Studies in hospitals have reported insufficient knowledge levels among registered nurses (RNs) or nursing staff on PU prevention.2,3 In long-term care, RNs’ PU prevention knowledge has been at a moderate level 4 ; however, the knowledge of nursing staff, including employees with lower education levels, has been less reported. 5
In hospitals, shortcomings in knowledge related to PU prevention among nursing staff, including RNs, practical nurses (PNs) and nursing assistants (NA), have varied. Knowledge gaps have been identified in PU classification, PU preventive activities related to repositioning, seating support or pressure-relieving devices.2,6–8 Low knowledge has also been reported in the practice of avoiding massage in the region with tissue injury and in identification of the role of lack of tissue oxygen as a cause of PU development.8,9 In nursing staff's knowledge in risk assessment and nutrition, the results have been contradictory.3,6,9
In long-term care, RNs’, NAs’ and last year student nurses’ (SNs) knowledge was the lowest in PU classification, risk assessment, skin assessment, repositioning and reduction of pressure and shear.4,5 Other areas of low knowledge were identification of the role of lack of tissue oxygen as a cause of PUs. 9 In long-term care, RNs, NAs and SNs had the highest PU prevention knowledge in PU aetiology and development, risk assessment, nutrition and pressure-reducing mattresses.4,5
The increase in knowledge about PU prevention is influenced by various factors. A higher-level nursing education of nurses seems to improve nursing staff's knowledge about PU prevention. On the other hand, there is a need to strengthen PU prevention knowledge among nursing staff with lower levels of education.5,7,9,10 Knowledge has also been improved with specific education in PU, participation in in-service training programmes or conferences, or reading about PUs. In addition, positive improvement has been found with previous experience with PU management, caring for a higher number of patients with PUs per week, or working in intensive care units or wound care clinics.8,10 To improve nursing staff's PU prevention knowledge in long-term care, it has been suggested that guidelines, education programmes and an environment that makes it possible to provide continuing education should be created for nurses to prevent PUs. 4 An increase in PU training, in both nurse education and continuing education and training after graduation based on strong clinical leadership, has been suggested as a solution.6,11 However, opposite results have also been presented. 12
Educational interventions to improve PU prevention knowledge in hospitals have consisted of face-to-face or virtual education training sessions on PUs, or both,13,14 as well as an electronic clinical decision support system for PU prevention. 15 In the nursing home context, they have consisted of the implementation of multiple PU prevention guidelines, 16 an electronic clinical decision support system for PU prevention 17 and construction of a framework for nursing homes by analysing the nursing competency for PU management, followed by implementation of suitable PU education programmes. 18
Most studies on PU prevention knowledge, including PNs or Nas, have been conducted in acute care or hospital settings. More context-tailored research for PU prevention knowledge is needed in long-term older people care facilities (LOPC) because of the characteristics of nursing staff with lower levels of education and the characteristics of residents with old age, cognitive impairments, including dementia, or movement disabilities.5–7,9,19 This indicates a need for interventions with appropriate and practical education in this area.
Aims
The aim of this study was to evaluate the impact of nursing staff's renewed consistent PU prevention practice intervention on their PU prevention knowledge. In this study, nursing staff is defined as registered nurses (bachelor's degree education) and practical nurses (vocational level education). The research question was: What is the nursing staff's knowledge of PU prevention at baseline and after the renewed consistent PU prevention practice intervention? The hypothesis was that after the intervention, the nursing staff's PU prevention knowledge would be more improved in the intervention facility compared to the comparison facility.
Methods
Study design and participants
The study had a quasi-experimental intervention design. Data collection took place in two LOPC facilities (n = 13 units) in one hospital district in Finland. The facilities were chosen purposefully and then randomly allocated, by pulling from a hat, to an intervention and a comparison facility (Figure 1). Registered nurses (RNs, bachelor's degree education) and practical nurses (PNs, vocational level education) working in these units during data collection who were willing to take part in the study were included. The intervention facility and the comparison facility were located in different cities, more than 50 km apart. Blinding was not used. The sample size was not determined in advance because all the nursing staff in the facilities were given an opportunity to participate in the study. The TREND Statement checklist 20 was used as the reporting method.
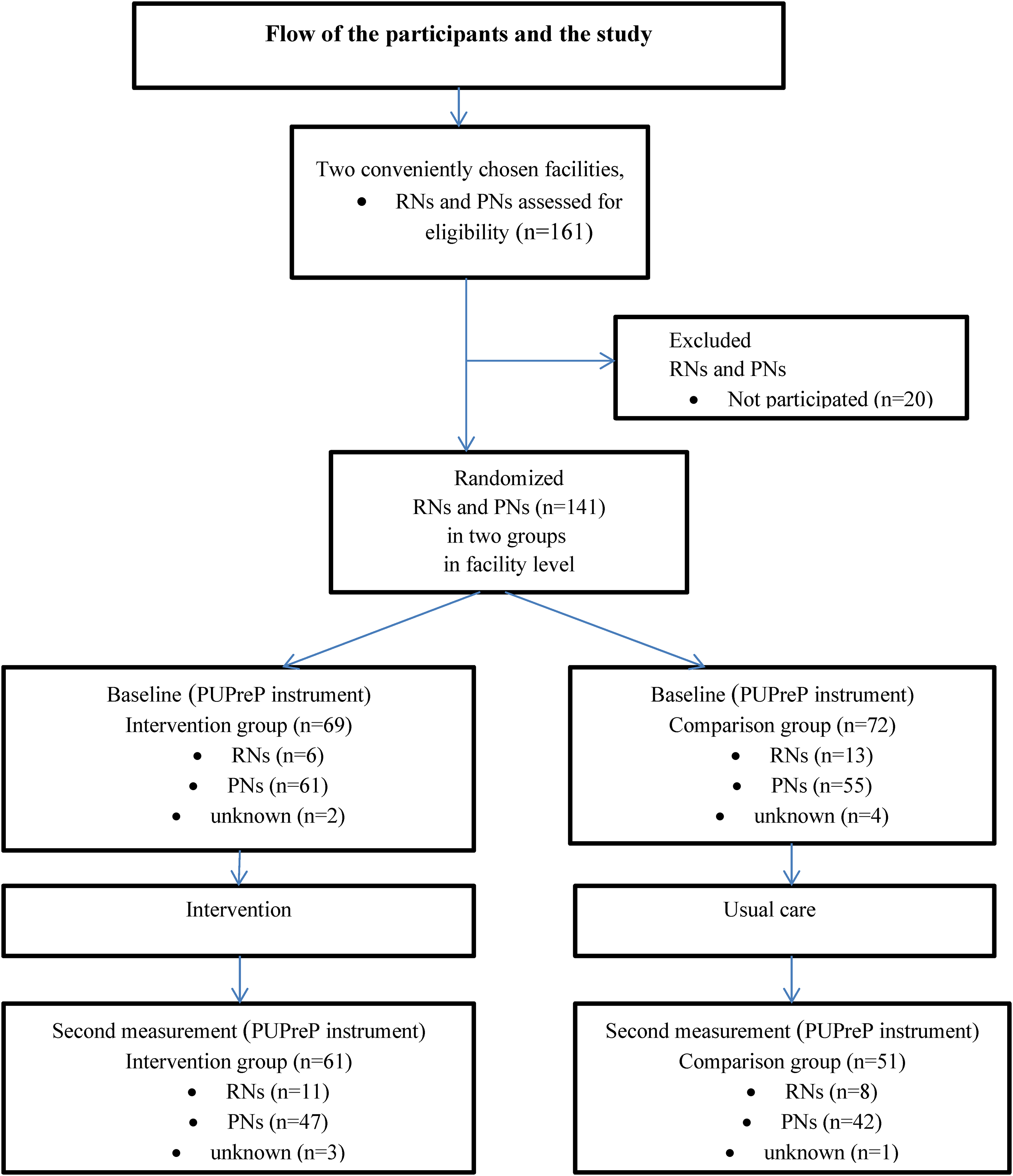
Participant and study flow.
Data collection
The data were collected twice, in January 2016 and January 2017. The Pressure Ulcer Prevention Knowledge test (PUPK; ©2015 Eriksson, Hietanen) 7 with a paper and pencil method was used to evaluate nursing staff's knowledge of PU prevention practices at the facility level. Developed based on the international PU prevention practice guidelines, 21 but not validated, the test consists of 34 items in seven subscales of PU prevention knowledge areas: (1) PU development and risk factors; (2) PU classification; (3) PU risk assessment; (4) PU prevention with repositioning; (5) PU prevention with pressure-relieving devices; (6) PU prevention with nutrition; and (7) skin assessment and skin care. Each subscale includes four or five items with answer options ‘yes’ or ‘no’. Scores of areas were min 0, max 5, except PU risk assessment, which included four items, were min 0, max 4.The instrument does not specify the level of good knowledge, but in this study we used the following interpretation: 5 (4.51–5) = high knowledge level; 4 (3.51–4.50) = good knowledge level; 3 (2.51–3.50) = moderate knowledge level; 2 (1.51–2.50) = satisfactory knowledge level; and 0–1 (0–1.50) = poor knowledge level; except in PU risk assessment: 4 (3.51–4) = high knowledge level; 3 (2.51–3.50) = good knowledge level; 2 (1.51–2.50) = moderate knowledge level; 1 (0.51–1.50) = satisfactory knowledge level; and 0 (0–0.50) = poor knowledge level). The background questions included the nursing staff's current position, education, length of experience, participation in additional training, self-evaluation of own PU prevention skills and self-evaluation of additional training needs.
Intervention
The intervention involved a development and implementation of a renewed consistent PU prevention practice in LOPC, 22 based on international PU prevention guidelines 1 and by using the OMEBP model with four phases (Figure 2). 23 The four phases were as follows: 1 = ‘Development needs for current practice’ (2 months); 2 = ‘Plan for consisting practice’ (1 month); 3 = ‘Consistent practice’ (10 months); and 4 = ‘Evaluation and follow-up of the practice’ (up to 1 year). The content of the renewed consistent PU prevention practice was a bundle of six PU prevention areas: risk assessment; skin assessment and skin care; nutrition; repositioning; pressure-relieving devices; and documentation. Written instructions were produced for the renewed PU prevention practice named ‘Procedure for PU Prevention in LOPC Facility’. 22 In the intervention, education for nursing staff had a strong role in the development phase, and also as a supporting structure during the implementation phase of the renewed consistent PU prevention practice (Table 1).
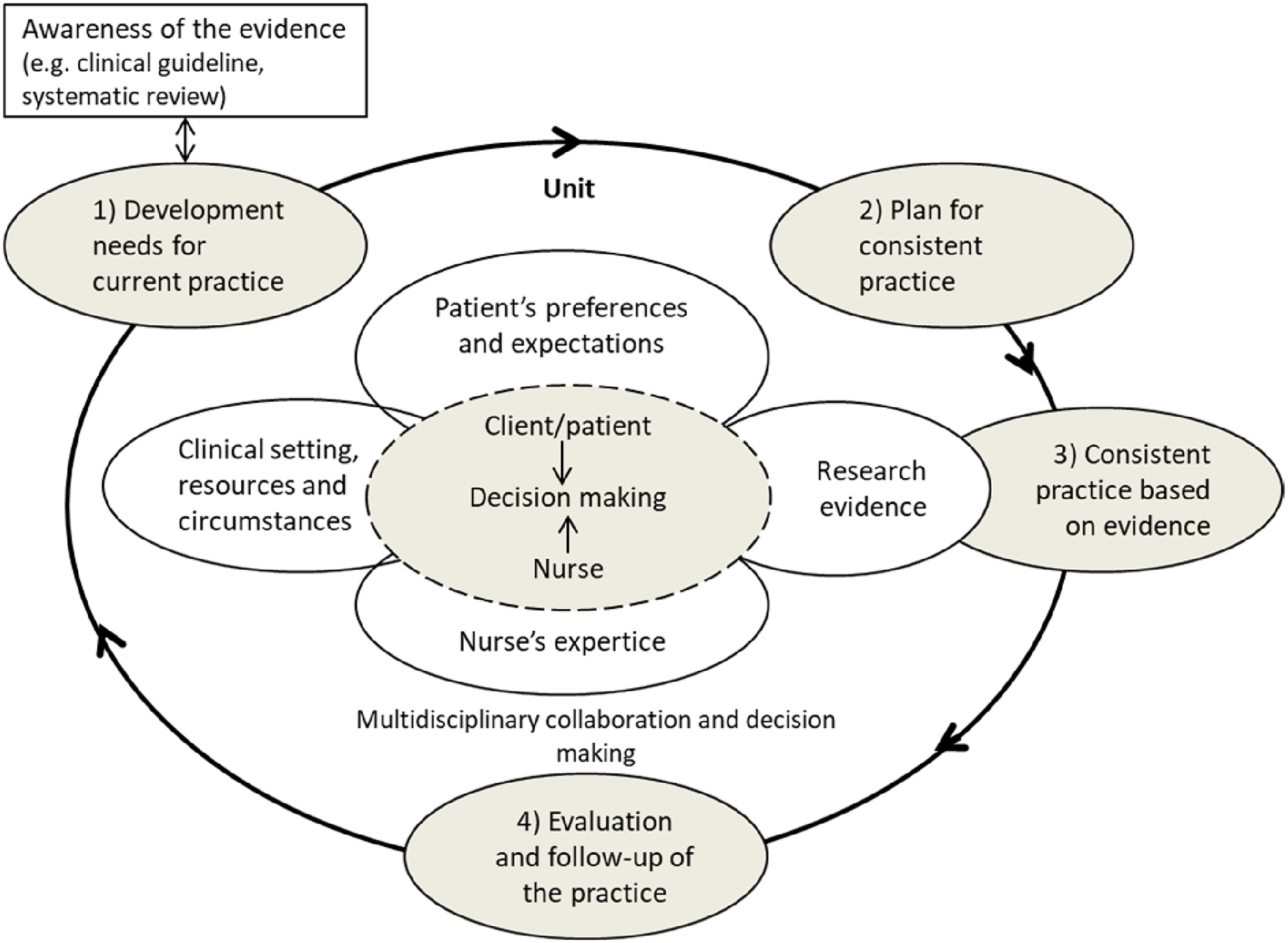
The operational model for evidence-based practices, OMEBP (Nursing Research Foundation, 2022). 23
Education for PU prevention for nursing staff (Phases 1 and 3 in intervention).
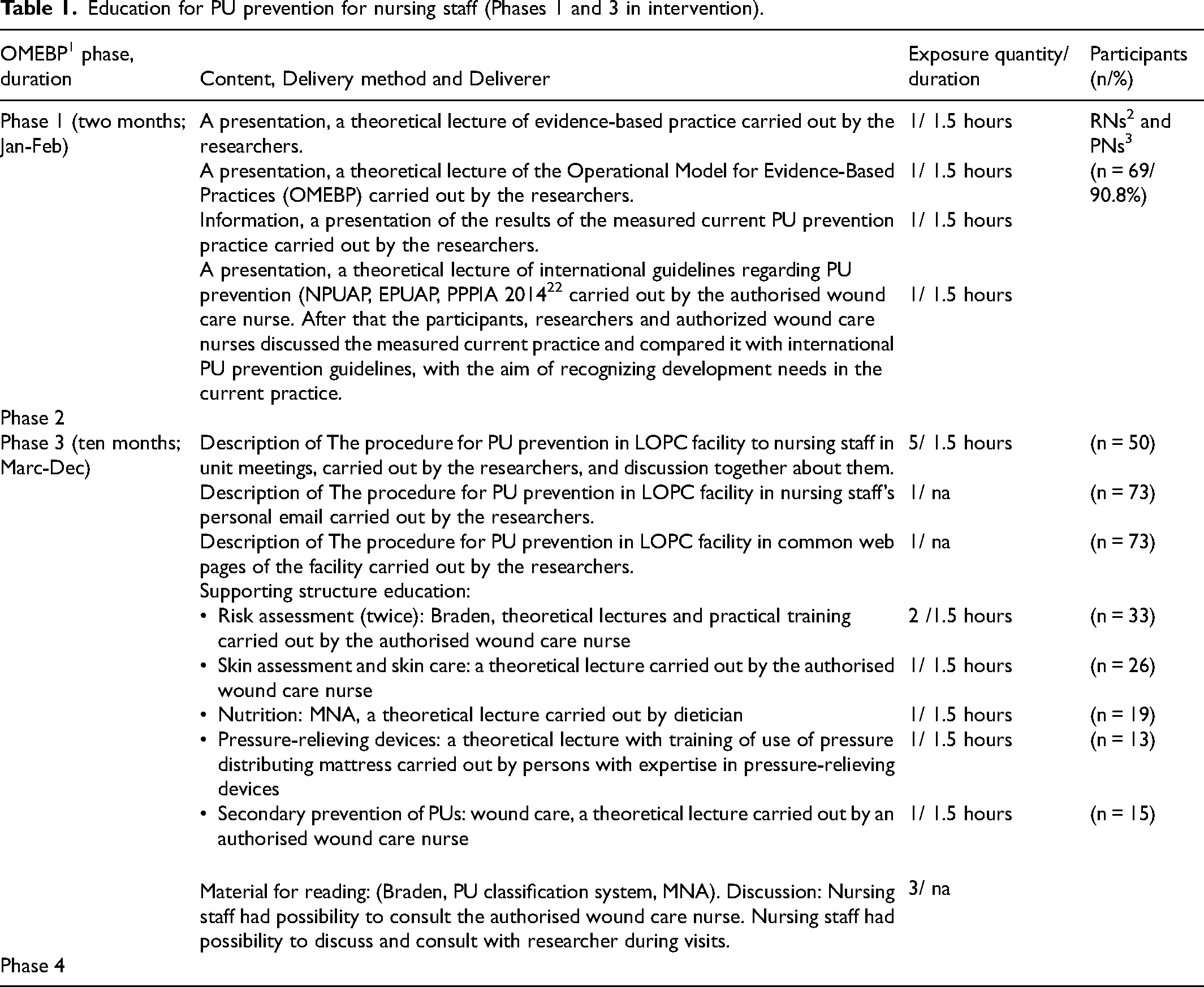
In the first phase of education, theoretical lectures to nursing staff, consisting of head nurses, RNs and PNs, was carried out in two meetings about evidence-based practices, the OMEBP model, 23 international guidelines for PU prevention and early identification, 21 and the international PU classification system. 21 Education in the first phase started 2 weeks after the current PU prevention practice was identified with the Pressure Ulcer Prevention practice (PUPreP) instrument, a questionnaire developed for this study based on international PU prevention guidelines. 22 The nursing staff also completed a baseline knowledge test 2 weeks before the start of the first phase of education. Based on the first phase of education, and after informing the staff of the results of measurement of the current PU prevention practice in the facility, development needs in the current practice were identified by the nursing staff jointly with the researcher.
The second phase, consisting of head nurses and two wound contact persons from each unit in the facility, included two meetings for planning of the renewed consistent PU prevention practice, tailored in the facility and written out in the ‘Procedure for PU Prevention in LOPC Facility’. 22 In the third phase, the education first included unit meetings, during which the researcher went through the renewed consistent PU prevention practice together with the nursing staff. The written procedure was also sent to the nursing staff members’ personal email addresses for private study. After unit meetings, nursing staff immediately started to work according to the new, renewed procedure. During this third phase, education was used as a support structure in the intervention, and nursing staff took part in 6 monthly 90-min education sessions on topics such as PU risk assessment, skin assessment and skin care, nutrition, pressure-relieving devices, and, as secondary prevention of PUs, wound care. Three of these education sessions were theoretical lectures; risk assessment included a theoretical lecture with practical training and pressure-relieving devices included a theoretical lecture with training of the use of a pressure-distributing mattress. The fourth phase was the evaluation phase of the intervention including second assessment of the current PU prevention practice and PU prevention knowledge test.
Analysis
Data were analysed using SPSS Statistics for Windows version 26 (IBM Corp., Armonk, NY, USA). The Mann–Whitney U-test for non-normally distributed continuous variables and Pearson chi-square test or Fisher's exact test for categorical variables were used to compare the participants’ characteristics between the groups.
The total sum and subscales of the PUPK test 7 were calculated by summing up the correct answers of items. A correct answer was scored as 1 point and a wrong or missing answer as 0 points. If all the answers of a subscale were missing, the subscale was scored as missing. If one or more subscales were missing, the total sum was scored as missing (four participants).
Differences in subscales of PU knowledge before and after the intervention within groups were tested using the Mann–Whitney U-test, and in the total scale of PU knowledge using the independent sample t-test. Frequencies and percentages of correct answers in single items of the PUPK test were calculated before and after the intervention, and differences before and after the intervention within the groups were tested by using the Pearson chi-square test or Fisher's exact test. Differences in changes in total sum of PU knowledge between the groups was tested using a two-way analysis of variance (group × time interaction effect) and differences in changes in subscales of PU knowledge between the groups using ordinal logistic regression (group × time interaction effect). The level of significance was set at p < 0.05.
Ethical considerations
The research followed good scientific practices as determined by the Finnish Advisory Board on Research Integrity 24 and it conforms with the Declaration of Helsinki. 25 Ethical approval (43/2015) was obtained from the Ethics Committee of the University of Turku. The participating organisations gave permission to conduct the study. The nursing staff were informed about the voluntary nature of participation and the possibility to discontinue without consequences, provided informed consent to participate and had an opportunity to ask questions before and during the research.
Results
Characteristics of the participants
The total number of RNs and PNs who participated in the study at the two LOPC facilities was 141 at baseline and 112 after the intervention; in the intervention facility, there were 69 participants at baseline and 61 after the intervention, and in the comparison facility, there were 72 at baseline and 51 after. In the beginning, 21 RNs/PNs and were not willing to participate in the study. At the follow-up, the corresponding number was 50. All the participants were educated healthcare professionals. Most participants were PNs. The characteristics of the participants are shown in Table 2.
Characteristics of participants, before (baseline) and after the intervention.
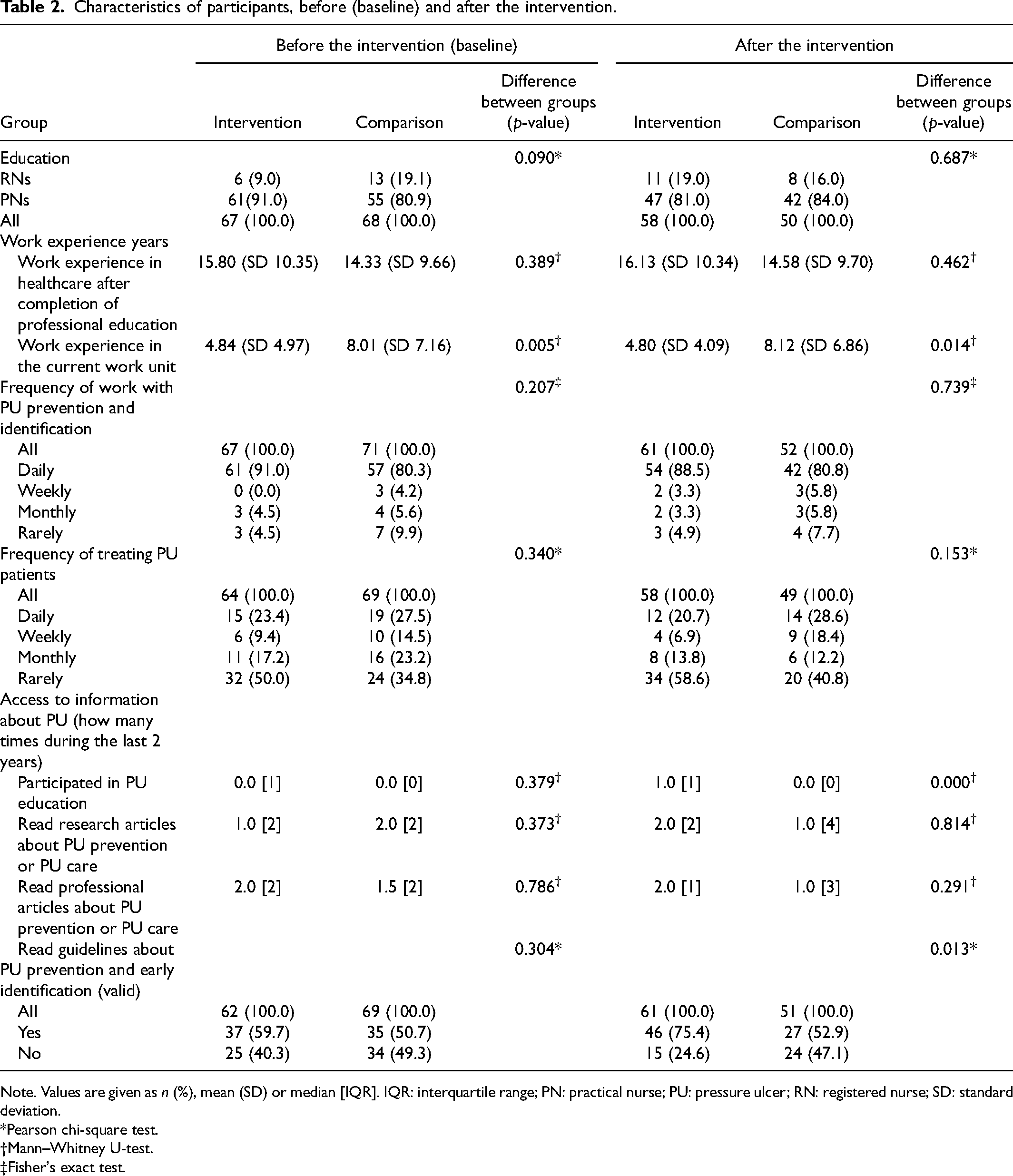
Note. Values are given as n (%), mean (SD) or median [IQR]. IQR: interquartile range; PN: practical nurse; PU: pressure ulcer; RN: registered nurse; SD: standard deviation.
*Pearson chi-square test.
Mann–Whitney U-test.
Fisher's exact test.
Nursing staff's PU prevention knowledge
The PU prevention knowledge areas were measured in seven subscales using the PUPK test (Table 3). At baseline, the total sum of the PU prevention knowledge of the participants (n = 68 intervention/69 comparison) was 26.85/27.03 (range 0–34, p = 0.702), and after the intervention (n = 61 intervention/52 comparison), 28.66/27.83 (p = 0.079). At baseline, the comparison group had better knowledge in PU risk assessment (p = 0.011) while the intervention group had better knowledge in nutrition (p = 0.004). No other differences in subscales were found between the intervention and the comparison group at baseline.
Pressure ulcer prevention knowledge.
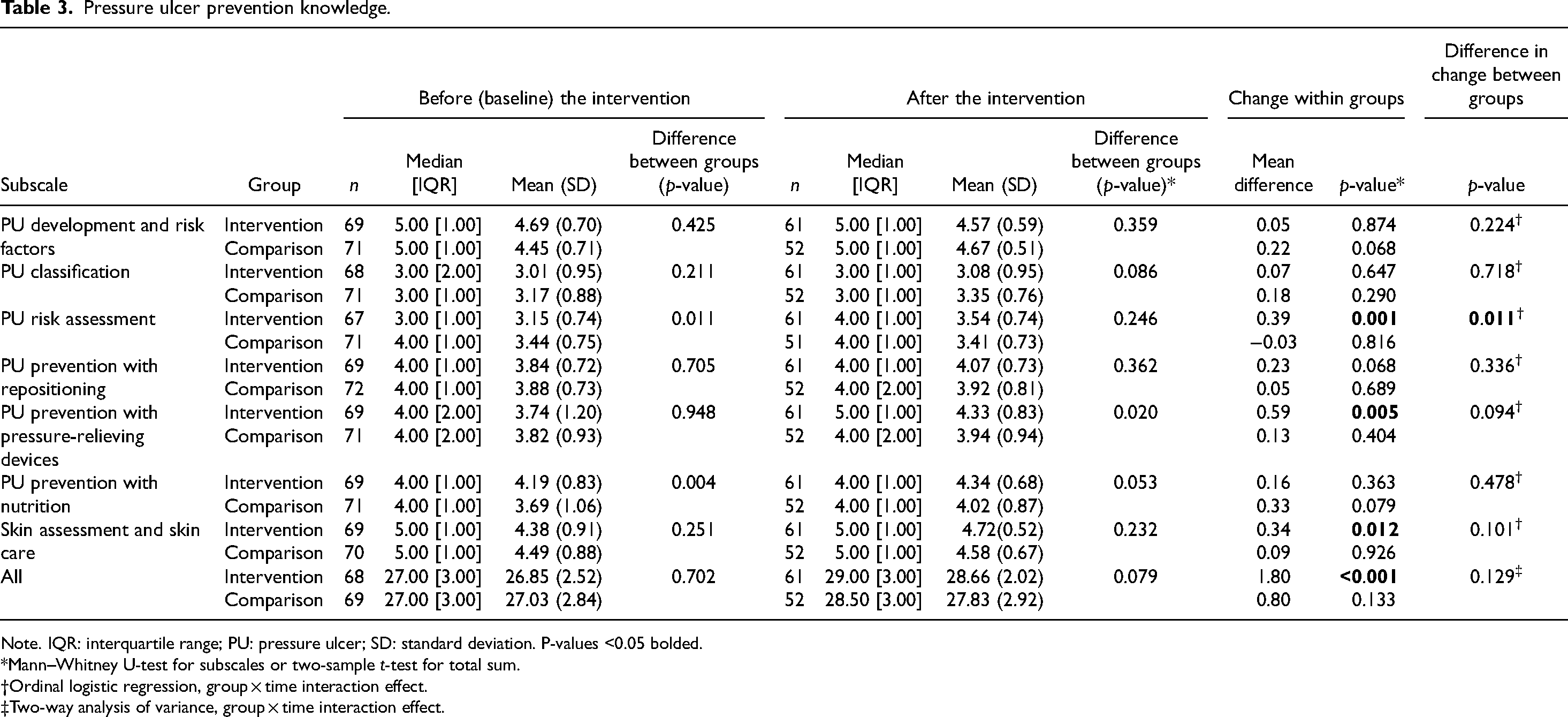
Note. IQR: interquartile range; PU: pressure ulcer; SD: standard deviation. P-values <0.05 bolded.
*Mann–Whitney U-test for subscales or two-sample t-test for total sum.
Ordinal logistic regression, group × time interaction effect.
Two-way analysis of variance, group × time interaction effect.
At baseline (Table 3), the intervention group had high knowledge in PU development and risk factors (mean 4.69, SD 0.70). Both groups had moderate knowledge in PU classification (mean 3.01, SD 0.95; mean 3.17, SD 0.88).
The difference in change in total sum of PU knowledge between the groups was not significant (group × time effect, p = 0.129). However, in the intervention group, the PU prevention knowledge improved significantly (p < 0.001) while it did not improve in the comparison group (p = 0.133). In PU risk assessment, the knowledge improved significantly more in the intervention group compared to the comparison group (group × time effect, p = 0.011). In the intervention group, a statistically significant improvement was seen in PU risk assessment (mean change 0.39, p = 0.001), PU prevention with pressure relieving devices (mean change 0.59, p = 0.005), skin assessment and skin care (mean change 0.34, p = 0.012) and in the total sum (mean change 1.80, p < 0.001) (Table 3). In the comparison group, no statistically significant improvement was seen in any of the subscales (Table 3).
After the intervention (Table 3), both groups had high knowledge in PU development and risk factors and skin assessment and skin care (mean 4.57–4.72, SD 0.59–0.52; 4.58–4.67, SD 0.59–0.67). The intervention group also had high knowledge in PU risk assessment (mean 3.54, SD 0.74). Both groups had moderate knowledge in PU classification (mean 3.08, SD 0.95; 3.35, SD 0.76).
In single items of the PUPK test, the percentage of correct answers was reported (Supplement 2). The most well-known items among the participants did not differ much between the groups. However, both groups had ‘perfect knowledge’ in only a few items. At baseline, 100% of the participants (n = 65–69) in the intervention group gave a correct answer to three items in the subscales PU development and risk factors, PU classification and PU prevention with nutrition. Meanwhile, in the comparison group, 100% of the participants (n = 70–72) gave a correct answer to three items under subscales PU prevention and risk factors (two items) and PU prevention with nutrition.
In the intervention group, after the intervention, PU prevention knowledge had improved significantly (p = 0.010–0.048) in six items. They were in the subscales PU risk assessment (two items), PU prevention with repositioning (one item), PU prevention with pressure relieving devices (two items), and skin assessment and skin care (one item). The knowledge worsened (p = 0.042–0.050) in two items: both were in the subscale PU classification. Meanwhile, in the comparison group, PU prevention knowledge had improved significantly (p = 0.043–0.046) in two single items that were in the subscales PU prevention with pressure-relieving devices and PU prevention with nutrition.
After the intervention, 100% of the participants in both groups gave correct answers to the items in the subscale PU development and risk factors; the intervention group to two items and the comparison group to three items. In addition, 100% of the participants in the intervention group answered correctly one item in the subscale PU prevention with repositioning and the comparison group one item in the subscale PU prevention with nutrition.
The least well-known items among the participants, both at baseline and after the intervention, were in the subscale PU classification: two items in both the intervention and the comparison group (Supplement 2).
Discussion
The aim of this study was to evaluate the impact of nursing staff's renewed consistent pressure ulcer prevention practice intervention on their PU prevention knowledge in LOPC. The content of the renewed consistent practice, based on international PU prevention guidelines, comprised a bundle of six PU prevention areas: risk assessment; skin assessment and skin care; nutrition; repositioning; pressure-relieving devices; and documentation. In the intervention, education for nursing staff was in the development phase, and during the implementation phase it was used as a supporting structure.
As hypothesised, in the PU risk assessment, the nursing staff's PU prevention knowledge improved more in the intervention facility compared to the comparison facility. In addition, in the intervention facility, the nursing staff's knowledge improved in pressure-relieving devices, skin assessment and skin care, and in the total sum of PU prevention. In PU classification, nutrition and repositioning knowledge did not improve significantly, but a tendency of improvement was seen. However, in two of these areas, knowledge was at a good level before and after the intervention. On the other hand, in the PU classification, knowledge remained at a moderate level. In the PU development and risk factors, knowledge did not improve, but it was already at a high level at baseline. In the comparison facility, none of the PU prevention knowledge areas improved significantly. These results of the study are in line with earlier recommendations to use educational interventions to improve nursing staff's PU prevention knowledge.4,11,14 Earlier studies have concluded that in long-term care, the possibility to provide education programmes concerning PU prevention knowledge is the basis for properly planned PU prevention. 4 In addition, to guarantee an adequate level of PU prevention knowledge, it was concluded that continuing PU prevention education is needed and appropriate educational interventions to improve PU prevention knowledge should be conducted.11,14 Contrary to the findings of this study, one earlier review concluded, due to the low-certainty evidence provided by the included studies, that further information is needed to clarify the impact of education of nursing staff on the prevention of PUs. 12 To add evidence about effective interventions in the LOPC context, where most of the nursing staff are PNs, it is necessary to conduct more interventions suited for this context and focused on improving PNs’ knowledge to prevent PUs.
In the present study, in both facilities, the nursing staff's PU prevention knowledge was mostly at a good level at baseline. The results are in line with an earlier study of nurses conducted in long-term care 4 but opposite to a study reporting nursing staff's PU prevention knowledge to be insufficient in hospital.2,6 In this study, most of the nursing staff were practical nurses with vocational education in a long-term care setting. These results are contrary to earlier studies of the knowledge improvement need mentioned, especially among employees with lower levels of education.5–7,9
In the study, nursing staff's PU prevention knowledge was highest at baseline in PU development and risk factors, PU risk assessment, skin assessment and skin care, and nutrition. These results are in line with earlier studies regarding high PU prevention knowledge in nutrition,3,9 but contrary to the study reporting low PU prevention knowledge in risk assessment. 3 The results are partly in line with the results of PU knowledge studies conducted in long-term care reporting nutrition,4,5 with PU development 4 and risk assessment 5 having the highest scores but those studies also reported the inability to identify lack of oxygen in the tissue as the primary cause of the mechanism of PU formation, or confusion about the difference between a risk factor and a causative factor in PU etiology.4,5 In this study, the least well-known single items in both groups both at baseline and after the intervention were items in PU classification. These results are in line with those from an earlier study that also reported the lowest score in PU classification. 4 A lot of variation occurs in the results in earlier studies; this may be caused by differences in the research context, characteristics of participants or formulation of questions. To ensure a high level of nursing staff's PU prevention knowledge in all prevention areas in a certain context, research for effective interventions is still needed.
In this study, the context-tailored intervention was effective in improving PU prevention knowledge. This is in line with an earlier study 18 where, in the nursing home context, after identifying PU prevention problems, discussing suitable education for PU prevention and assessing barriers to use of knowledge, an educational programme was designed. 18 In line with the current study, the importance of understanding the environmental context in the implementation of PU prevention guidelines was also seen in an earlier study 16 where an educational intervention that allowed organisations to implement PU prevention guidelines in hospitals and nursing homes improved the PU prevention knowledge of hospital nurses, but not of nursing home nurses. Similarly to the earlier study, 16 this study also adds evidence that research tailored interventions within different frameworks are needed for the improvement of PU prevention practice knowledge.
In this intervention, knowledge was improved by face-to-face PU prevention education. In earlier studies, face-to-face education, face-to-face training sessions and virtual education training sessions for nurses about PU topics improved their PU knowledge.13,14 On the other hand, the use of a computer programme involving an electronic clinical decision support system for PU prevention in a nursing home did not improve PU prevention knowledge. 15
Research on PU prevention has been ongoing for decades. For this reason, there is a lot of evidence-based information about it. The European Pressure Ulcer Advisory Panel (EPUAP), the National Pressure Injury Advisory Panel (NPIAP) and the Pan Pacific Pressure Injury Alliance (PPPIA) have drawn up international PU prevention guidelines. 1 National translations and summaries have been made. Today, evidence-based methods are available, and the implementation of a national patient safety programmes has decreased the prevalence of PUs; however, still not all PU prevention methods are widely adopted and used in practice. 26 There is a need for more evidence to reduce the gap between PU prevention research and practice. Furthermore, shorter, concise, and clear unit-specific instructions of PU prevention guidelines are needed for practical work, which will also facilitate the development of much-needed local education programmes. In addition, more evidence of educational interventions in the context of LOPC is needed because earlier educational interventions were often based on very low evidence or small samples. 12 These shortcomings may contribute to lack of PU prevention knowledge, affect the quality of care provided to patients and, as a consequence, lead to the development of PUs, suffering for patients and costs for healthcare. Education for professionals is one of the most commonly employed strategies for translating PU prevention guidelines into practice, and thus, by disseminating scientific evidence to practice, influence positively care outcomes as prevalence of PUs. 27 In order to guarantee effective PU prevention, healthcare staff must have regular education about PU development, risk factors and the implementation of PU prevention. This means that continuous training and evaluation and development of practice are needed.
The intervention improved PU prevention knowledge. Most PU prevention areas improved or were at a good level before and after the intervention. However, in the PU prevention area, PU classification knowledge remained at a moderate level. The explanation could be that PU classification was not one of the prevention areas in the intervention, but also that although it was described in a presentation of international guidelines regarding PU prevention, during implementation, it was not an item supported by face-to-face education.
Education as a supportive structure seemed to improve the implementation of the consistent PU prevention practice. However, the impact of the education used in the study as a supporting structure during implementation requires more research. It seems that dosing times may affect the improvement of the PU prevention knowledge: risk assessment, which was dosed twice, was the most improved PU prevention area, whereas knowledge in PU classification, which was not dosed as supportive education, did not improve. The other supporting structure education sessions were dosed once. However, the development of a cognitive structure of education and learning analytics could also be a topic for future research.
Study limitations
This study had some limitations related to the reduction of nursing staff, nursing staff's participation in the monthly supportive education sessions, the difference between the intervention and comparison group at baseline in terms of work experience in the current work unit, and validity of the instrument.
The reduction in nursing staff was carried out in both the intervention and the comparison care units during implementation in the third phase. In addition, long-term substitutes rotated between institutions and this caused some changes in the composition of the nursing staff. In this situation, the ‘Procedure for PU Prevention in LOPC Facility’, i.e., the written instructions for the renewed PU prevention practice, had already been produced and used for 3 months. They were also used as part of the orientation for new workers. However, it is possible that the situation may have increased the haste and stress caused by a greater workflow and new nursing staff members and might thus have caused bias to the results. The strength of this study was that the intervention facility and the comparison facility were located in different cities, more than 50 km apart. For this reason, there was no chance that the staff at the intervention facility would start to work at the comparison facility or risk of spillover effect.
Not all nursing staff members participated in the monthly supportive education sessions. Some worked in the care units or were off duty. However, these facts were known, and the target was that as many nursing staff members as possible would participate in these supportive education sessions and ‘share the message’ in their own units. Otherwise, the intervention reached the nursing staff well, as planned, via the orientation day, the development days, unit meetings, personal emails and common web pages of the facility.
Although the content of the PUPK instrument was based on international PU prevention guidelines and had been used and evaluated previously, there were some deficiencies. In particular, some questions needed to be updated. Today, this development work has been completed, and a new, updated and validated version of the instrument is available. 7
The difference between the facilities relating to the length of work experience at baseline is also a limitation. Longer work experience in the current work unit at baseline among the comparison facility compared with the intervention facility was also a limitation. However, longer work experience in the current work unit did not mean better PU prevention knowledge at baseline, maybe because the length of work experience in healthcare after completion of professional education did not differ between the facilities. The limitations of the study should be considered when generalising the results. The strength of this study was the high participation rate of nursing staff (88%), which increases the reliability of the results.
Conclusions
The context-tailored consistent PU prevention practice intervention improved PU prevention knowledge in LOPC. In the intervention facility, the nursing staff's PU prevention knowledge improved in PU risk assessment, pressure-relieving devices, skin assessment and skin care, and in the total sum of PU prevention. Most PU prevention areas improved or were at good level after the intervention. The results of this study are generalisable to LOPC in Finland, but the intervention may also be used internationally in long-term older people care.
For the prevention of PUs to be effective, context-tailored education for nursing staff for the development of PUs, risk factors and implementation of PU prevention could be a solution to increase staff's knowledge and succeed in implementing evidence-based working methods. This means continuous education, evaluation and measuring of PU knowledge and prevention practice by the management in LOPC. Context-tailored PU prevention practice interventions focusing on nursing staff in LOPC facilities should be developed and these aspects should also be included in the education for lower-level nursing staff.
Relevance to clinical practice
The context-tailored intervention improved nursing staff's PU prevention knowledge in LOPC. The intervention in this study has the potential to be used and reproduced. The ‘Procedure for PU Prevention in LOPC Facility’, written instructions for the renewed PU prevention practice are a useful tool for head nurses in LOPC as a concise guideline for evidence-based PU prevention practice in the LOPC context.
Supplemental Material
sj-docx-1-njn-10.1177_20571585241265430 - Supplemental material for The impact of consistent pressure ulcer prevention practice on nursing staff's pressure ulcer prevention knowledge: A quasi-experimental intervention study
Supplemental material, sj-docx-1-njn-10.1177_20571585241265430 for The impact of consistent pressure ulcer prevention practice on nursing staff's pressure ulcer prevention knowledge: A quasi-experimental intervention study by Sirpa Mäki-Turja-Rostedt, Helena Leino-Kilpi, Tero Vahlberg and Elina Haavisto in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
Sincere thanks to the nursing staff of the facilities for taking part in this study. Anna Vuolteenaho is acknowledged for editing the English language.
Author contributions
SM-T-R, HL-K and EH conceptualised and designed the study; SM-T-R and EH developed consistent practice; SM-T-R collected the data; SM-T-R, TV and EH analysed the data; SM-T-R, HL-K, TV and EH wrote or revised the manuscript. All authors approved the final manuscript.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The corresponding author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partly funded by the Finnish Cultural Foundation; Betania Foundation; The State Research Funding: Satakunta Hospital District, Pori, Finland; the Wellbeing Services County of Satakunta, Finland and Finnish Wound Care Society.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.