
Abstract
During COVID-19, an increased incidence of out-of-hospital cardiac arrests was seen, resulting in decreased outcomes. In addition, altered attitudes to performing cardiopulmonary resuscitation among first responders were reported. The aim of this study was to explore ambulance personnel's experiences of, and lessons learned from, out-of-hospital cardiac arrest missions during the COVID-19 pandemic, in a Swedish context. Nine Swedish ambulance personnel were interviewed, and the data were analysed using thematic content analysis. The analysis illuminated professional, personal and relational consequences as well as lessons learned reported by the informants. The COREQ guideline was used to report the important aspects of the study. The ambulance personnel experienced several challenges, mainly due to the personal protective equipment. To enhance patient safety, they strived to remain resilient despite the challenges. The informants also expressed positive aspects of their experiences, such as having acquired increased competence through working under these circumstances. To strive for resilience and competence became the overarching theme. The experiences and the lessons learned described in the study, could contribute to helping ambulance organisations initiate new routines and/or improve existing ones, as well as developing a protective equipment that does not obstruct any aspect of an out-of-hospital cardiac arrest mission.
Introduction
During the COVID-19 pandemic, the incidence of out-of-hospital cardiac arrests (OHCA) increased in several countries worldwide. 1 An OHCA is defined as a cessation of cardiac mechanical activity, without signs of circulation, occurring outside of a hospital setting. 2 The ambulance personnel are essentially the first responders in emergency care, such as an OHCA event. 3 In Sweden, specific ambulance nursing care is defined as immediate prehospital medical actions or treatments given in, or in connection with, an ambulance. 4 The ambulance personnel in Sweden normally work in pairs and include one registered nurse (RN) with a 3-year bachelor's degree and/or an advanced specialised RN in ambulance nursing care or a nurse anaesthetist, with a 1-year advanced education at university level. Additional personnel could be a basic emergency medical technician (B-EMT) with a vocational education or equivalent. 5 Dependent on the nature of the emergency event and how life-threatening it is, different aspects of patient safety and different levels of nursing care are applied for the patient and their relatives in each situation. A review study found that more research focusing on unpredictable encounters on the openness and sensitivity in the professional–patient relation, and especially on the conflicts in emergency caregiving situations, is important. 6
The treatment of a time-critical event such as an OHCA, namely, cardiopulmonary resuscitation (CPR), primarily focuses on the life-saving intervention, including chest compressions and ventilations, combined with a shock from an automated external defibrillator. Advanced CPR additionally involves medical treatment and sometimes a more advanced airway technique as well as a defibrillation strategy. 3 CPR is an aerosol-generating procedure, which puts emergency responders performing this task during the pandemic at very high risk of exposure to the coronavirus. 7 During the COVID-19 pandemic, the European guidelines regarding resuscitation were therefore altered, and directions to the public were to withhold ventilations during CPR. 3 Ambulance personnel were advised to use a filter on the advanced ventilation equipment, as well as personal protective equipment (PPE). The PPE consisted of an apron, gloves, some sort of safety mask and/or a visor. 7
Previous research has shown that fewer attempts with CPR were initiated by bystanders or continued by the ambulance personnel during the COVID-19 pandemic. The number of patients with shockable rhythms was smaller, 8 and the arrival time of the ambulance was longer. 3 Furthermore, the prognosis of OHCA during COVID-19 was worse and the short-term survival, as well as the survival rate at hospital discharge, was lower than during the pre-pandemic period.8,9 In Sweden, the incidence of OHCA increased during the first half of 2020, and the outcome among the COVID-19 positive patients was worse than among those without COVID-19. 10 Furthermore, in the early stages of the pandemic, the first responders’ willingness to perform CPR during OHCA was altered. A study from the United States and Saudi Arabia reported that 58 of 501 first responders were unwilling to perform CPR during OHCA events, due to the following: 1) a fear of contracting COVID-19; 2) the risk of transmitting the infection to others; 3) absent PPE; and/or 4) a lack of effective treatment and/or vaccines. 11 A British study reported that emergency medical services had challenging experiences of OHCA missions during COVID-19, 12 and difficulties working in PPE were reported by an American study. 13 However, there is a lack of qualitative studies about ambulance personnel's experiences of, and the nursing care challenges involved at, OHCA events during the pandemic. There are, to the best of our knowledge, no such studies published in a Swedish context. Therefore, an exploratory study could offer a deeper understanding of the ambulance personnel's experiences of OHCA missions in Sweden. The lessons learned could help optimise ambulance personnel's conditions for continuing to help save lives. The aim of this study was thus to explore the ambulance personnel's experiences of, and lessons learned from, OHCA missions during the COVID-19 pandemic, in a Swedish context.
Method
Since the phenomenon under study was poorly understood, a qualitative study design was chosen. To be able to develop a rich understanding of the phenomenon 14 and capture the detailed perspective of a few informants, 15 an explorative, individual interview study was conducted.
Recruitment and context
The inclusion criteria were ambulance personnel, that is, RNs, specialised RNs and B-EMTs, who had experienced OHCA missions during the COVID-19 pandemic. A consecutive and convenience sampling approach, including all types of ambulance personnel, was chosen to ensure finding enough informants, since there is a general low rate of OHCA missions per year in Sweden. 16 Initially, informants from one region in southern Sweden were approached. Permission to conduct the study was granted from the operation managers of the ambulance service in the region, who also provided contact information to local managers of all ambulance stations in the same region. These local managers acted as gatekeepers and assisted in sending emails to all types of ambulance personnel in the region, with information about the study and contact information to the first author. The original three informants accepted participation after two reminders. In order to increase the number of informants, several requests were sent to two Facebook groups for national ambulance staff. This generated six more informants, resulting in nine informants (seven men, two women). Six informants had an advanced degree in nursing, one RN had a bachelor's degree and two informants were B-EMTs with 4.5 and 8 years of experience, respectively, of working as ambulance personnel. The informants worked in both public and private ambulance settings, and the specialised nurses were ambulance nurses and nurse anaesthetists. One of the informants had a current position as a specialised RN in an assisting medical first responder unit but was included due to a long previous experience as a specialised ambulance nurse.
Data collection
Directed by the aim of the study, a semi-structured interview guide was constructed by the first author (ES). A semi-structured interview method was chosen to ensure that the questions made the informants speak freely of their experiences, while still answering the aim of the study. 14 The semi-structured interview guide included 12 open questions encouraging the informants to describe their experiences of OCHA missions during the COVID-19 pandemic. The guide focused on questions about what worked well, what was challenging and which lessons learned could benefit future OHCA missions during similar circumstances. Whenever applicable, probing questions were used. To make sure that the questions answered the aim, one test interview was conducted before the commencement of the study 14 and this did not result in any alterations of the interview guide. The test interview was not included in the study. The nine interviews were conducted during September, October and November 2022, by the first author (ES). Due to preferences expressed by the informants and for geographical reasons, eight of the informants were interviewed online (Zoom). One face-to-face interview was conducted at the informant's place of work. After informed consent was collected, the interviews started with background data, such as age, sex, years as ambulance personnel, type of ambulance personnel and the approximate number of OHCA missions per year before the pandemic. The interviews followed the semi-structured interview guide and were audiotaped by mobile phone in flight mode. They lasted 23–39 min (median 28 min) and were transcribed verbatim by the first author (ES), shortly after the interviews. 14 An overall redundancy of information was achieved during the interviews,14,17 with some variation regarding the lessons learned by informants from working during the pandemic.
Data analysis and rigour
The total duration of the interviews was 269 min, generating 124 A4 pages of transcribed text. Data analyses were conducted inductively, 14 in several stages and including verification, using a thematic content analysis, according to Burnard et al. 18 The method of thematic content analysis is appropriate when semi-structured interviews have been carried out, recorded in full and transcribed as a whole. 19 The first author read each transcript to get a sense of the whole, and then wrote down initial codes in the margin. The initial coding involved a word or short summary that explained the specific text, in all parts of the transcript. Dross 18 was not coded since it did not answer the aim of the study, and all duplications were crossed out. The initial codes (n = 573) were regrouped (n = 31) and refined (n = 18) in many stages, and eventually became the final four categories (coloured marking pens were used). 18 During the process, efforts were made to understand the broader meanings that underpinned the data, and the analysis moved from manifest codes to latent categories and one theme (Supplementary material 1).
To achieve rigour and to increase credibility and confirmability, 20 the informants were asked to participate in member checking in the later stages of the analysis. 18 The member checking was conducted via email so as not to inconvenience the informants and consisted of returning analysed synthesised data to the informants and explored whether results were in line with the informants’ experiences. 18 The intended codes and categories, including representative quotes, were sent to the informants, encouraging them to provide critical feedback about errors and misinterpretations, as well as confirmation of the findings. 21 Although all nine informants initially accepted participation in the member checking, only five responded after one reminder. One informant declined to participate due to lack of time, and the four that participated agreed with the general picture of the codes and categories and did not want to add or change anything. Therefore, no alterations due to the member checking were made. However, to get a shorter and more comprehensive coding list, one final refinement of the codes was made after the member checking. Furthermore, the second author (AMW), who is an experienced researcher, read the transcripts and discussed the codes, categories and theme with the first author (ES), before and after the member checking. In addition, the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist 17 was used to report the important aspects of the study (Supplementary material 2).
Ethical considerations
Even though this study did not require ethical approval according to the Swedish Ethical Review Act, 22 an advisory statement from the local ethical board of the University was obtained (Reg. No. STUD 2022/1630). The advisory statement included no objections to the study but a recommendation that we specify for the informants the kind of working experience that the study sought to explore. Therefore, deeper feelings and emotions were not sought. In accordance with the Declaration of Helsinki, 23 ethical considerations were made. Before the interviews commenced, written informed consent was obtained from the informant who was interviewed on site, and the rest gave oral informed consent. All informants were informed that participation was voluntary and that they could withdraw from the study at any time. To ensure confidentiality, each quotation was assigned the informants’ professional background. Data were stored securely and anonymously, in compliance with the General Data Protection Regulation. 24
Results
The informants had worked within the prehospital setting for 2–30 years. Their age range was 26–50 years and the annual number of OHCA missions was in the range of 4–70. Table 1 shows the demographic data of the informants. Table 2 presents the results after the thematic content analysis.
The background data of the informants.
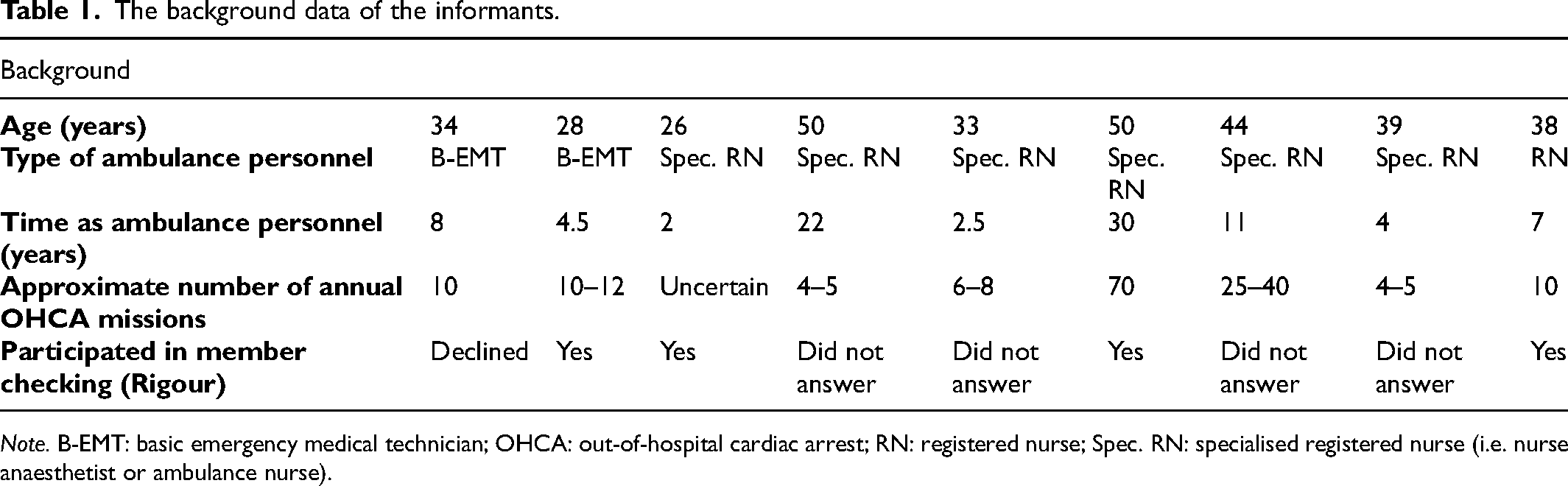
Note. B-EMT: basic emergency medical technician; OHCA: out-of-hospital cardiac arrest; RN: registered nurse; Spec. RN: specialised registered nurse (i.e. nurse anaesthetist or ambulance nurse).
Results after thematic content analysis.
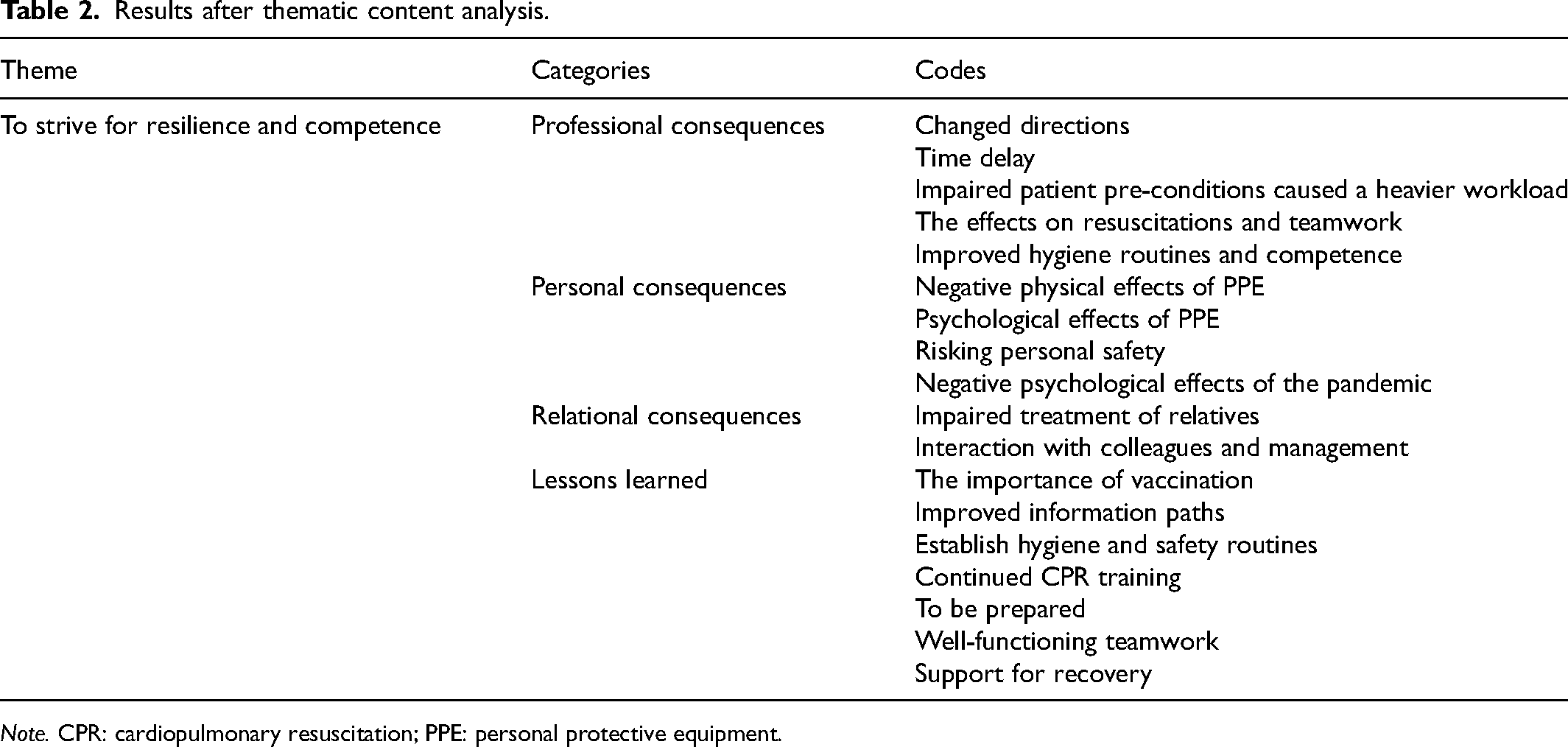
Note. CPR: cardiopulmonary resuscitation; PPE: personal protective equipment.
Theme and categories
The final coding stage consisted of 18 codes, emerging into four categories: Professional consequences; Personal consequences; Relational consequences; and Lessons learned. From these categories, the overarching theme emerged: To strive for resilience and competence. This main theme demonstrated that OHCA missions during the pandemic made work more difficult than usual. It was chiefly the impact of the PPE that caused many challenges, jeopardising patient safety, but also the fear the ambulance personnel had of getting infected themselves. However, the ambulance personnel worked harder despite the difficulties. They also learned from their experiences, which improved their performances during the OCHA situations as well as increasing their competence for the future.
Professional consequences
This category included experiences that had an impact on the ambulance personnel's work during COVID-19. When the pandemic started, the directions about how to conduct OCHA, and about what type of PPE to wear, often changed. Some informants felt that the constantly changing information was a great challenge. There was sometimes information from different authorities, which gave rise to confusion regarding the latest directions. Furthermore, due to the directions about the PPE, the response time increased. The informants, as well as the assisting units, such as the police force and the fire rescue squad, had to spend extra minutes putting on the PPE, which caused a delay in starting the CPR, which also jeopardised patient safety. ‘First you had to put on a safety mask or a visor and an airway protection mask and also put on a surgical gown and then the gloves and THEN we could enter.’ (Spec. RN) ‘There were a lot more non-shockable rhythms during COVID, under normally good circumstances, and it felt typical for these patients, that they didn’t have any good [health] conditions for surviving despite the rest of the circumstances being good.’ (Spec. RN) ’Yes, but the communication was difficult. There's a bigger risk of miscommunication between us as caregivers—in that we didn’t understand each other's directions properly. And there could obviously also be a risk of impaired treatment.’ (B-EMT)
There were, however, also positive experiences among the informants, who described how the OHCA missions during the pandemic led to improved hygiene routines and an increased adherence to them. Moreover, the informants expressed that they felt more competent after experiencing working with PPE and with infected patients. They felt that they now knew that they could manage working in PPE again if necessary. ‘/… / people have learned how to use their PPE, and /…/ they have regained a respect for working with contagious diseases that might have been at bit lacking.’ (RN)
Personal consequences
This category described how the informants in various ways were also personally affected by the changes in their working conditions. The PPE sometimes caused physical problems, such as difficulties breathing, increased warmth and sweating, as well as a lack of energy. This was especially difficult during the summer when it was already hot. ‘You get so much warmer in these plastic aprons, much sweatier. Then the working environment gets worse. Really much worse… I was sooo exhausted after having done these tasks, so when it was time to carry the patient down, it was tough.’ (B-EMT) ‘You feel the stress, that you want to, you sort of want to get inside as quickly as possible, and then to have to wait outside knowing that it will take a few minutes to get dressed.’ (Spec. RN) ‘It's positive to be protected against getting infected yourself as well as [against] spreading the disease, really positive.’ (Spec. RN)
Moreover, negative psychological consequences due to the pandemic itself were described. Some of the informants expressed an initial fear of not knowing how infectious the virus was and an ensuing fear of treating infected patients. ‘You were afraid, you didn’t know what it was, what was COVID, how dangerous it was, you had only heard that it came from China.’ (Spec. RN)
Relational consequences
This category demonstrated that besides having both a professional and personal impact, the pandemic also affected the relational interactions. Sometimes, due to the pandemic, more relatives were at home during the OHCA missions. The ability to give them a good personal treatment decreased due to the safety mask. The informants said that the PPE made them feel like ‘aliens’ and that it made them impersonal and distant towards the relatives in times of losing a loved one. ‘And to take care of relatives when you’re in plastics. That is also so insensitive.’ (B-EMT) ‘It's sad not to be able to have the communication and closeness with the person that might need it the most.’ (Spec. RN)
Lessons learned
This category showed what the informants found useful and learned during the pandemic, lessons that could help manage OHCA missions in future pandemics. Some informants expressed that vaccination of the ambulance personnel could help make the personnel feel safe during work, and that could potentially lead to less need of all the PPE. This would reduce the time lost while getting dressed. Furthermore, one informant stated that vaccinating the public could improve the possibilities of succeeding with the resuscitations, since the respiratory symptoms connected to COVID-19 impaired the conditions for surviving an OHCA. In addition, to improve the management of OHCA missions, the informants expressed that updated information should be managed by just one person or one specific authority. ‘I find it very important to coordinate information to the staff!’ (Spec. RN) ‘If we should need a similar safety equipment in cardiac arrest situations, then it's above all important to find good equipment that we can work in, without it becoming an obstacle for us.’ (Spec. RN)
The informants found that the teamwork between all other professionals involved in the OHCA mission was important. They described how the communication when wearing PPE was improved by talking as clearly and as loudly as possible and by making sure eye contact was made. The communication with colleagues was sometimes difficult, but if you tried to stay focused and listen to the one that was talking, as well as communicating using a closed loop, it was less challenging.
Despite the challenges of working during COVID-19, the informants in general felt that they received informal support from talking with their colleagues about their experiences. However, the formal support for recovery after the missions could have been better handled by the organisational management.
Discussion
The aim of this study was to explore the ambulance personnel's experiences of, and lessons learned from, OHCA missions during the COVID-19 pandemic, in a Swedish context. Despite their professional background, the ambulance personnel expressed feelings of stress and frustration as well as experiencing physical consequences. The ambulance personnel knew the CPR algorithm beforehand and had previous experiences of OHCA missions where everyone knew their role. This enhanced their ability to provide as safe care as possible, given the changed circumstances. However, the frequently changed directions that the personnel received were challenging, and the adherence to new protocols for the PPE sometimes faltered.
Professional consequences included the changed patient presentation, with impaired preconditions, and an increased number of OHCAs, a younger clientele and less shockable rhythms, as reported by others.1,8,12 The personnel often adjusted to this by working harder and sometimes longer during resuscitations. Wearing the PPE caused a time delay and was a great challenge, as it jeopardised patient safety as well as impairing communication between the team members.12,13 In addition, some informants experienced decreased defibrillation by bystanders, since the dispatch centres’ text messages to lay responders were paused during the pandemic causing a further delay in the start of CPR. 25 In addition, a prolonged arrival time of the ambulance was seen during the pandemic. 26
Moreover, the early stages of the pandemic sometimes caused emotional responses resulting in personal consequences, which might have been due to the insecurity of not having enough knowledge of the virus or how dangerous it was. In addition, the vaccine had not yet been developed, which could further explain these feelings. Similar findings have been demonstrated in another study, 11 but, in contrast, the attitudes against performing CPR shown in that study did not emerge in the present study. Instead, the informants reported an ability to be resilient by developing different ways to improve their work during the OHCA mission. For example, to decrease the time delay for a more successful resuscitation, the team saved minutes by taking the seat belt off and donning the PPE while getting to the site. This meant putting the life of the patient first while risking their own safety, as also reported by others.12,13 Some informants also risked their own safety by taking parts of the PPE off during resuscitation. All this demonstrates how personnel strived to maintain patient safety to be able to save lives, which was paramount during the OHCA missions.
Still, informants found that the communication and the nursing care involving the relatives were impaired, as wearing the PPE caused relational challenges and consequences – especially, after a failed OHCA mission, when the patients had died. A recent British study found that both physical and emotional fatigue sometimes emerged during and after an OHCA mission, and that wearing the PPE added to the personnel's stress and frustration. In addition, the study demonstrated that ‘change fatigue’ was common and that new directions were not always followed. 12
Further, the informants in the present study perceived that their competence had increased by having been through a pandemic, and that they had learned important lessons and acquired various insights about how to confront a new potential pandemic. In fact, an increased adherence to the new and improved hygiene routines was important to maintain, and wearing PPE had been a useful experience, as they felt safe and protected by the PPE. 13 However, wearing PPE was also a physical challenge to endure, particularly in hot weather. When the workload was heavy or the environment was stressful, the ambulance nursing care risked being affected. This could mean withholding of, or failure to conduct, necessary nursing care because of limited resources to perform person-centred care. 27
In line with a pre-pandemic study 28 the informants in the present study expressed that both a mental and a practical preparation were helpful during the missions. For example, both personnel and patient safety would be enhanced if the staff at the dispatch centres could inquire more in depth, when someone called, whether the patients had a suspected or confirmed contagious disease before dispatching the ambulance. Surprisingly, only a few informants in our study mentioned the need of general vaccinations. This could be due to the fact that the informants had experienced the OHCA missions at different stages of the pandemic.
The informants did not express any specific lack of support for physical and mental recovery from the management. However, the fact that they sometimes had to risk their personal safety in donning the PPE because of the need to decrease the time delay for the sake of patient safety is something that should be addressed by the organisation in the future. Since ambulance systems vary between countries, more studies in different contexts are required. The lessons learned during the pandemic should be further explored to help establish new routines and/or improve existing ones. Therefore, to enhance the resilience and competence of the personnel, 29 the organisational management need to learn from the experiences of the informants in this study and improve their support for the ambulance personnel in the future.
Strengths and limitations
The chosen design helped to explore the ambulance personnel's experiences of the OHCA events during COVID-19. 14 The semi-structured interview guide and probing questions made the informants talk freely of their experiences as well as providing the information needed to answer the aim of the study. 14 However, this study has some limitations. A consecutive and convenience sampling method was chosen due to the scarce incidence of OHCA events, and only nine informants were included due to difficulties in recruitment. Thus, owing to the relatively small sample, the findings cannot be generalised. However, the aim of this qualitative study was to explore the experiences of the ambulance personnel, and the purpose was not to generalise the findings to a population. 14 The informants came from different regions, had various levels of education and previous experiences of OHCA missions, and they also had different guidelines for PPE, CPR and CPR training, which may decrease the dependability and the transferability 20 of this study. Nonetheless, the variation of informants led to rich data that answered the aim, which is a strength in the study. 14
The study was performed at the end of 2022, when the pandemic had receded; therefore, there was a potential risk of an impaired recollection. However, the experiences were similar among the informants, which may mean that the main things that changed with regard to their OHCA missions, due to the pandemic, were the things that had made an impact on all of them and were remembered.
From the analysis, categories emerged supported by numerous codes. However, the categories based on a smaller number of codes were still included to give voice to all aspects of the informants’ statements and thereby enhance authenticity.17,30 According to Polit and Beck, 14 confirmability is enhanced when the findings reflect the informants’ voices, and those voices are presented through quotes in the present study. During the analysis, the authors’ pre-understanding might have influenced the interpretation, entailing a risk of bias. The first author (ES) is a specialised ambulance nurse with prior prehospital experience in the ambulance setting. Therefore, to enhance credibility, 20 a reflexive journal was maintained at all stages of the study 31 (accessible on request from the corresponding author). Confirmability was aimed at by the member checking, 18 and credibility was further enhanced 20 by having the second author (AMW) oversee the analysis process at all stages. There were only four member-check responses, but three responses are normally sufficient, 19 and the informants agreed with the codes and categories, which increases transferability and can be considered a strength of the study.18–20
Conclusion
Despite a limited sample, the experiences and the lessons learned described in this study could contribute to improvements of PPE guidelines during OHCA missions in similar situations in the future.
The ambulance personnel acquired increased competence that helped them remain resilient despite the COVID-19 challenges, while experiencing consequences on professional, personal and relational levels.
However, the management should support the ambulance personnel in providing PPE that does not hinder any aspect of the OHCA missions or risk either patient safety or the safety of the personnel.
Moreover, the organisation needs to support personnel in ensuring improved information paths, establishing or updating hygiene and safety routines, and offering formal routines for recovery after the OHCA mission.
The dispatch centres could also support and enhance the mental preparedness of the ambulance personnel before and during the OHCA missions.
The experiences of the relatives, particularly when losing a loved one in dire circumstances, is an area that needs to be further explored. Elucidating these experiences would contribute to an improved ambulance nursing care, for relatives as well, during OHCA missions when PPE is used.
Supplemental Material
sj-docx-1-njn-10.1177_20571585241231309 - Supplemental material for Ambulance personnel's experiences of, and lessons learned from, out-of-hospital cardiac arrest missions during the COVID-19 pandemic: An interview study
Supplemental material, sj-docx-1-njn-10.1177_20571585241231309 for Ambulance personnel's experiences of, and lessons learned from, out-of-hospital cardiac arrest missions during the COVID-19 pandemic: An interview study by Emma Sjöberg and Anne-Marie Wangel in Nordic Journal of Nursing Research
Footnotes
Acknowledgments
The authors wish to thank the informants in the study. We also want to express our gratitude to the Swedish Resuscitation Council for financial contribution for the language editing process, after the study was completed.
Author contributions
Study design and data collection: ES. Data analysis, manuscript preparation and critical review of the manuscript: ES, AMW. Both authors approved the final manuscript.
Conflict of interest
The authors declare that there is no potential conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profits sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.