
Abstract
Numerous countries in the world have chosen to allow district nurses to prescribe drugs to streamline the primary care process. This qualitative, systematic literature study aimed to examine district nurses’ experience of prescribing within primary care. The search followed the PRISMA-P search strategy, and the quality assessment of the nine articles was completed using the review template for assessing studies with qualitative methodology, using GRADE CERQual. The databases CINAHL, Pubmed, PsycINFO, and Scopus were used. The result shows that district nurses experience prescribing as crucial for being able to meet patient needs through holistic and person-centered care. Being able to sufficiently and efficiently meet patient needs contributed to increased job satisfaction and professional pride in district nurses. However, district nurses need more collegial support and training in prescribing. The additional burden that the ability to prescribe poses needs to be addressed to prevent limitations in the prescription rights of district nurses. Through an extended prescription right, district nurses can contribute to a more efficient care system that can meet future demand for healthcare services in primary care.
Introduction
Countries worldwide face challenges in reforming their national healthcare system to meet the demands of the aging population, chronic diseases, and increased complexity in primary care. 1 Due to the increasing demands on healthcare, nurses’ prescribing of drugs has been updated in over 40 countries worldwide. 2 A globally shared strategy consists of delegating tasks performed by physicians to registered nurses to increase the availability of care and the efficiency of healthcare cost-effectively. This delegation means allowing district nurses to prescribe drugs to make healthcare more efficient. 3 The benefits of drug prescription carried out by district nurses have resulted in increased availability of care, more efficient healthcare with high-quality care for patients, cost-effectiveness, improved health, and patient satisfaction.4,5 Indeed, research has shown several barriers related to nurses’ prescribing drugs, such as diagnostic uncertainty 6 and lack of organizational support from healthcare clinicians and management. 7 These barriers can result in nurses no longer writing prescriptions. 8
The USA and Canada's implementation of drug prescribing for specialist nurses, in 1975, has inspired and contributed to several countries following suit. Today, nurses prescribe drugs in 44 countries. 2 Education and regulation for district nurses with the authority to prescribe drugs vary in different countries. The type of drugs the district nurses can access differ between the full range of available drugs to a limited scale. The legal responsibility varies between independent prescriptions to a supplementary prescription under the supervision of a physician.9–11 Independent prescribing includes the diagnoses, establishing appropriate treatment plan, prescribing drugs, and performing a follow-up. Supplementary prescribing is performed after the physician has made an assessment. The person prescribing the drugs is responsible for the follow-up and assessment of the prescribed drug.9–11
Two-thirds of the drugs district nurses can prescribe in Sweden are non-prescription drugs and one-third require a prescription.12,13 In comparison to other countries, Swedish district nurses are able to prescribe fewer drugs even though prescriptions for district nurses have existed since 1994. In other countries, the district nurse prescribes drugs such as opioids, diabetes drugs, drugs for high blood pressure, and antibiotics.14,15 Establishing the prescription of drugs for district nurses in these countries showed that visits to a district nurse have increased and have made care more efficient, which also contributes to the planning of future healthcare.14,16,17
To be equipped to meet future healthcare-related challenges and demands, primary care needs to be as effective as possible. 18 Patients perceived that they received faster care and treatment as well as good quality of care.17–19 Nevertheless, nurses’ prescribing authority has not been well studied. Further research is needed on how the prescribing of drugs is perceived and experienced by district nurses, to develop more efficient primary care. Previous research shows the positive effects of district nurses’ prescription of drugs; however, there is a lack of research based on district nurses’ own experiences with prescriptions. This aim of the present literature review was to shed light on the district nurses’ experience of drug prescribing in primary care.
Design
In this systematic, qualitative literature review, the Evans model 20 is used as it is appropriate for the context of nursing research. The Evans model 20 comprises four phases. The phases are in the following order: gather the sample; identify the key findings; relate themes across studies; and retrospection to ensure the interpreted data matches the original data. The chosen model for this qualitative systematic literature review with an interpretive synthesis is suitable for analyzing, interpreting, and compiling already published research. This is supported by the structure that makes it possible to reach a deeper understanding of the studied phenomenon.
Methods
To perform the first phase in the Evans model, 20 gather the sample, a systematic literature search on CINAHL, PubMed, PsycINFO, and Scopus was performed to find relevant articles on the subject. The search strategy was revised by a university librarian. We performed pilot searches using identified keywords based on the research question. We specified the research question in a structured way by using the SPICE model (setting, perspective, intervention, comparison, and evaluation) for qualitative studies. The SPICE model functions as a tool to facilitate the literature search and structure the specified research question. 21
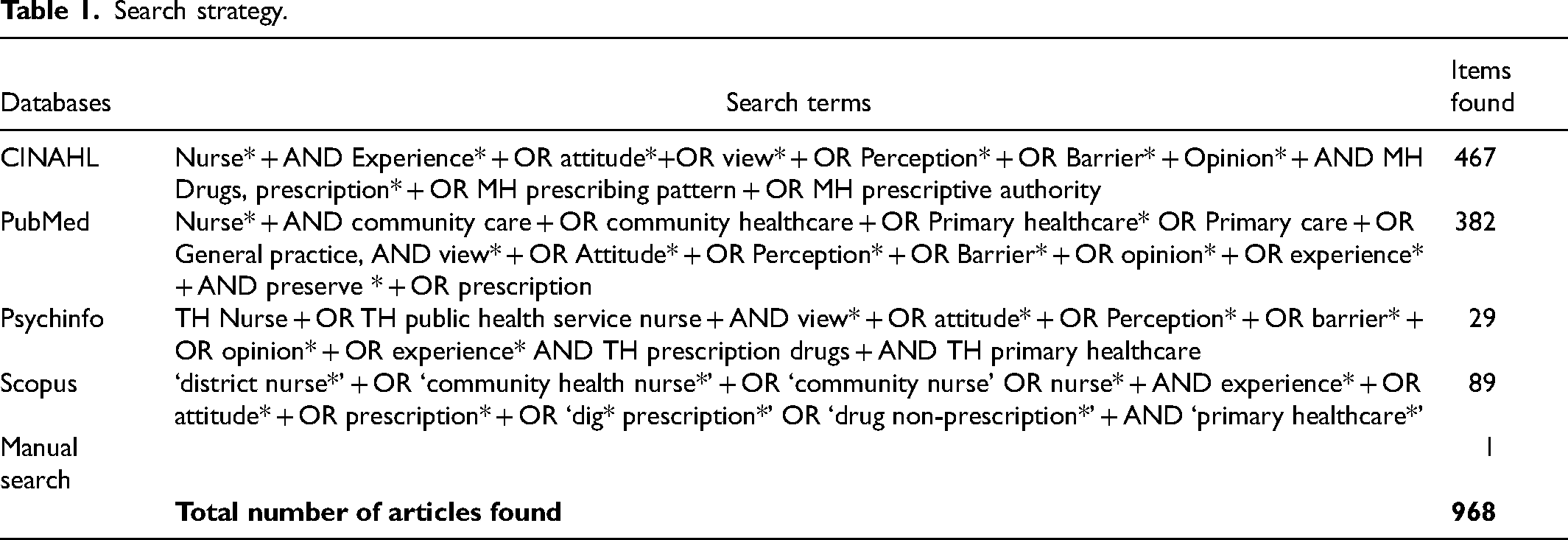
We combined the search terms in free-text, Major Headings (MH), and Thesaurus, further using the Booleska operators AND and OR. Adjustments were made in each database (Table 1). A supplementary search according to SBU was carried out in Google Scholar with a free-text search in Swedish with the following phrase: Articles on the district nurses’ prescription authority. With this method, a Swedish article relevant to the subject was found. 22 The initial literature searches in all databases were conducted in May 2022 and updated in June 2022.
Search strategy.
The criteria for inclusion for this systematic literature review require articles to be peer-reviewed and published between 1 January 2010 and 6 December 2022 in Swedish or English. Articles focusing on the patient perspective or any other profession with a prescription rights perspective, e.g. pharmacists, nurses’ prescribing rights regarding inpatients or hospital care, quantitative studies, systematic literature reviews, and qualitative syntheses, were excluded.
To perform the second phase in Evans model, 20 identify the key findings, with reporting for systematic reviews and meta-analyses according to Moher et al., 23 (Figure 1). A total of 968 articles were identified after the searches on mentioned databases. After removing the duplicates, 960 articles remained. In that step, the authors read all the article titles. The aim was to identify relevant articles established on the inclusion criteria. Further, 831 abstracts were read individually, and 32 articles were selected by the authors in consensus. These remaining 32 articles were read in full text by the authors, resulting in another 23 articles being excluded. A total of nine articles were identified as key findings and were therefore included as they were relevant to the aim and the inclusion criteria of this article (Figure 1). In addition, a manual search was made of the reference lists in the nine articles without any relevant further suitable articles being found.
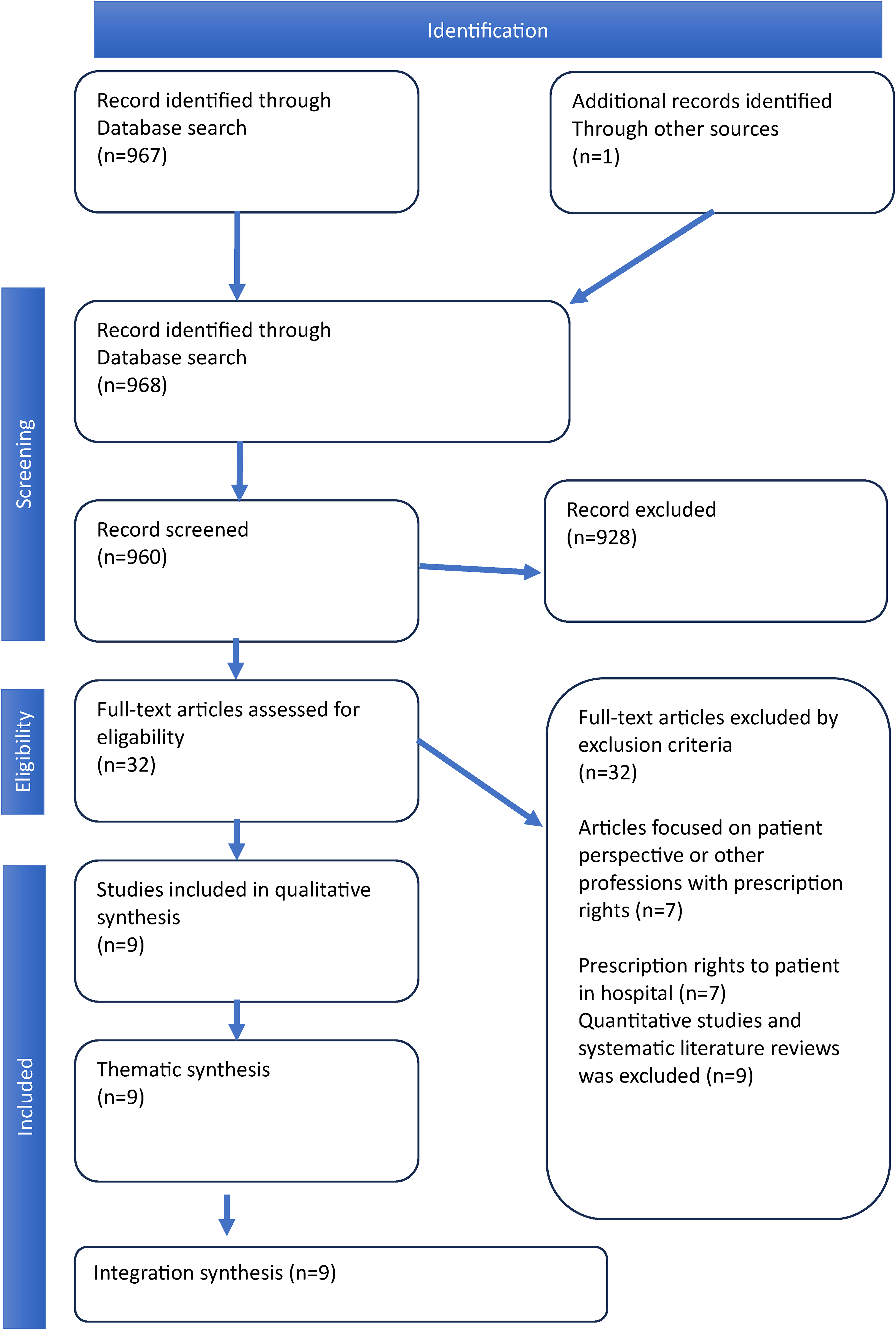
Prisma search strategy.
The quality assessment of the nine articles was completed using the review template for assessing studies with a qualitative methodology, using GRADE CERQual's four assessment areas: coherence; methodological bias; sufficient data; and relevance. 24 The classification according to GRADE CERQual is high reliability, moderate reliability, low reliability, and very low reliability. 24 The quality assessment is important to ensure that the chosen articles are of high quality. Therefore, the authors assessed each article individually, and then the assessments and classifications were compared until a consensus was reached, to increase the credibility of the individual assessment. 24 In total, nine articles were considered high quality.
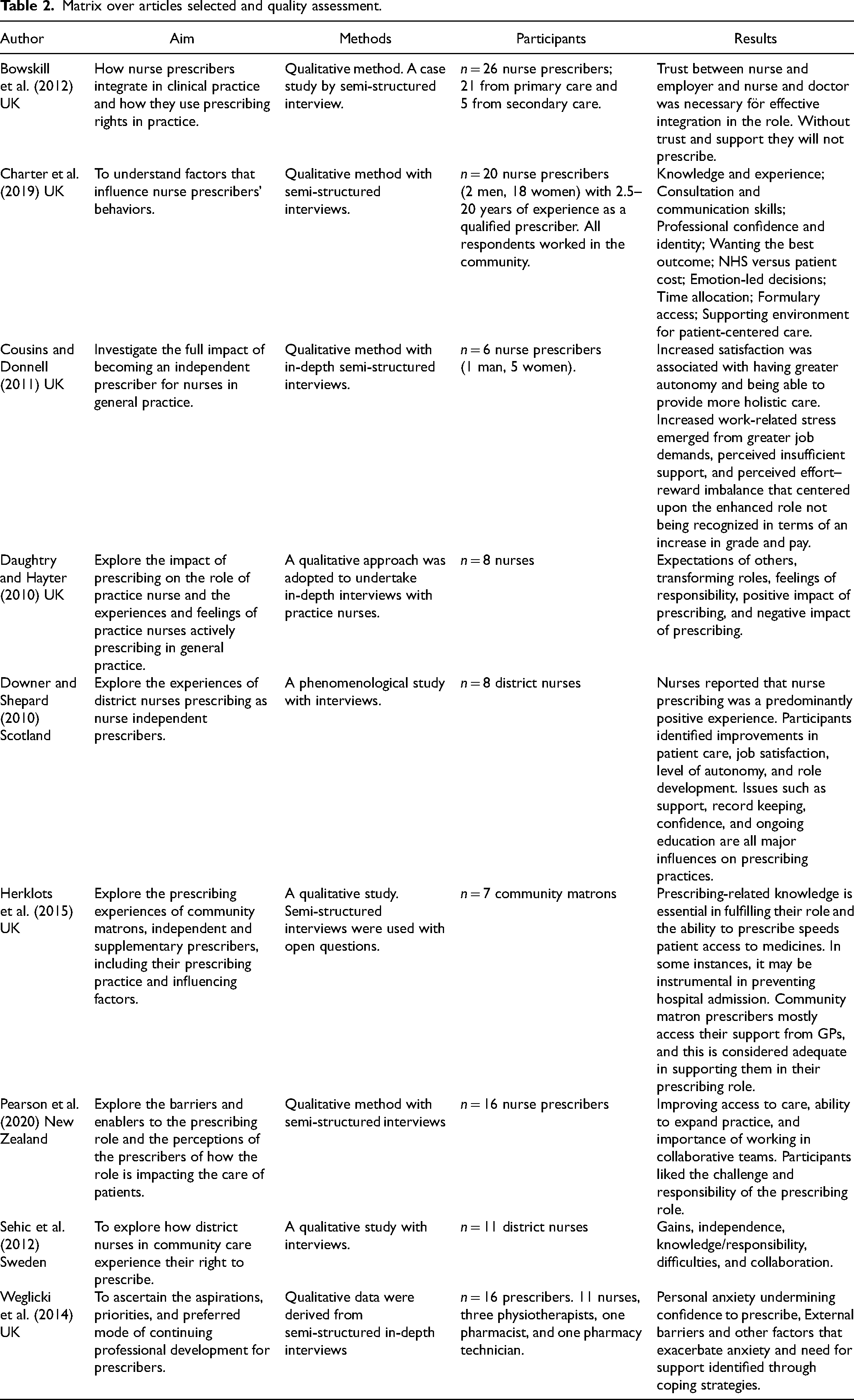
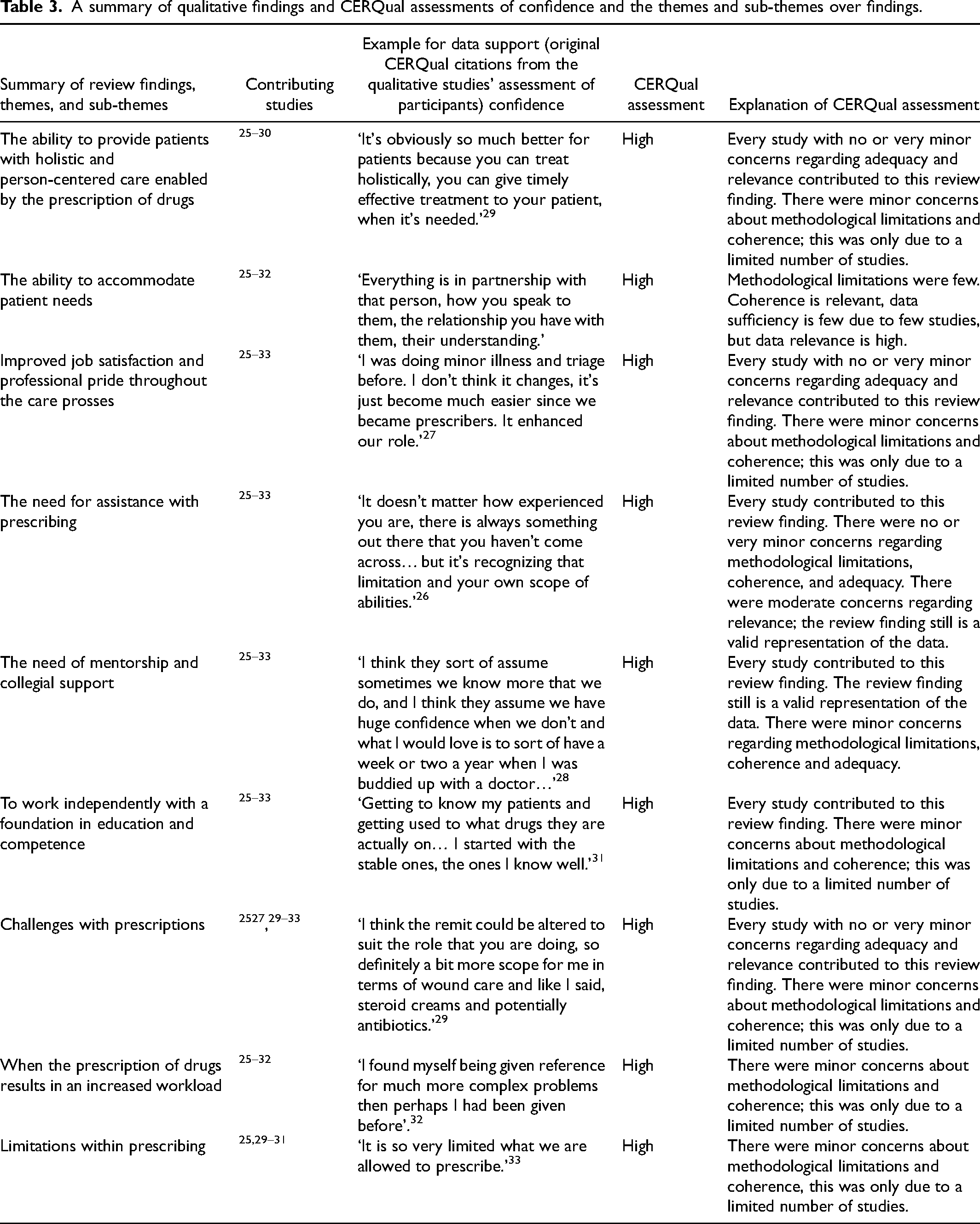
Data extraction was performed and summarized in an article matrix of the nine included articles. 21 The article matrix contains the following categories: authors; publication date; title; purpose; design; data collection; selection; analysis; results; quality; and classification assessment (Table 2). A summary of qualitative findings and CERQual assessments of confidence and the themes and sub-themes in the findings are shown in Table 3.
Matrix over articles selected and quality assessment.
A summary of qualitative findings and CERQual assessments of confidence and the themes and sub-themes over findings.
Data synthesis
Data synthesis, the third phase in the Evans model, 20 relate themes across studies, involves a systematic review of previous research and results in a compilation of data. 20 This entails that the data analysis aims to describe and interpret data in the form of a synthesis of findings. First, all the authors repeatedly read the articles included in the qualitative literature review in full text individually. Second, the authors withdrew the key findings from the selected literature as codes. Third, the key findings of codes and phrases were condensed and placed in groups based on differences and similarities. Lastly, the researchers made their individual syntheses and then compared and discussed them. The comparative process resulted in themes and subthemes compared to the original articles to achieve relevance within interpretations. All texts were read in retrospection to ensure the interpreted data match the original data. All the authors agreed on the final synthesis. In the fourth phase in the Evans model, 20 describe the phenomenon, the results are presented in themes and sub-themes.
Results
The result consists of nine articles with qualitative design. The result is presented under three themes and six sub-themes.
The ability to provide patients with holistic and person-centered care enabled by the prescription of drugs
In a partnership with the patient, the district nurse could make an individual assessment based on the patient's needs. District nurses’ right to prescribe was both preventive and curative; the work was described as more efficient as the waiting time for a physician was eliminated. An increase in job satisfaction was reported as a result of being able to provide person-centered care for the patient. The prescription rights provided a sense of pride in the profession, increased self-confidence, and increased prestige.
The ability to accommodate patient needs
The extended education and competence required from district nurses made it possible to perform a holistic assessment and offer individual treatment for each patient.25–29 District nurses experienced elevated trust from their patients.25,27,29 District nurses created a partnership with their assigned patients based on trust, which was crucial for ensuring the patient's confidence in their nurse. This partnership aided the decision of the best course of treatment with the addition of the patients being able to express their opinions to a trusted nurse. 25
District nurses reported the care being provided as more efficient, which decreased patients’ suffering, for instance, through a larger scale of preventative care solutions. District nurses acknowledged that the number of hospitalizations decreased due to the district nurses' ability to treat patients individually without assistance from a physician.25–27,29–32 The advantage of the right to prescribe, other than the patients receiving care quicker, was the district nurses’ ability to complete assignments faster.25–27,29–32 Time spent on finding a physician available to prescribe medicine was eliminated in the district nurses’ time distribution. The physicians’ time could be spent on complex patients.25–27,29,30,32
Improved job satisfaction and professional pride throughout the care processes
Performing holistic and person-centered care enhanced job satisfaction and professional pride.25,29 Possessing the responsibility of holding consultations with patients and being able to help provided satisfaction and pride for the professional identity.25,26,28–33 District nurses expressed increased job satisfaction credited to the person-centered care, enabled by the right to prescribe. The confidence and self-image of the district nurses heightened as a result.25–27,29,30 District nurses experienced an increased status and the accompanying respect of colleagues. This new work situation, including happiness and pride, was expressed through the district nurses’ desire not to return to not having prescription rights. 26
The need for assistance with prescribing
With the addition of college mentorship and support, district nurses became more secure in their individual prescribing. Collegial support resulted in continuous knowledge development for district nurses. In the circumstances of needing more support from colleges, district nurses chose to prescribe smaller amounts of medication than what they had previous experience with. To increase confidence, the district nurses requested various forms of education. The education extended independence for the district nurses throughout the entire care process. It demonstrated how a lack of support and mentorship could result in a halted development of prescription-related skills.
The need of mentorship and collegial support
District nurses’ confidence in their own ability to prescribe lessened with the lack of support from experienced colleagues and superiors. Lack of collegial support also resulted in flailing self-confidence in district nurses regarding other medical areas needed to complete the prescribing process. If the district nurse experienced support from their peers, a higher level of self-assurance was perceived, facilitating a higher level of security in diagnosing patients.27,30,32,33
Inexperienced district nurses had a greater need for support from peers and physicians to successfully take on the prescriber role.27,33 Without collegial support, a defining fear of causing patients to have side effects became a hindering factor for district nurses’ ability to prescribe medication they had no previous experience with.27–33 Inadequate support from experienced prescribers resulted in district nurses choosing to only prescribe medication in cases in which they had previous experience.26–31
This narrow use of the right of prescription was described as reducing the degree of utilization in which it could have been used. District nurses described how they realized their knowledge gaps and, therefore, lacking peer support, did not prescribe drugs outside of what they felt was their level of knowledge and experience.25–29,31–33
District nurses described how, as opposed to receiving support from doctors, they could work against the resistance from doctors who disliked district nurses prescribing drugs. This resistance negatively affected district nurses in their role as prescriber due to a lack of cooperation and support.27,31 In the case of which doctors were positive about district nurses’ right to prescribe medicine, the result was a well-functioning collaboration that improved the prescription process.25–29,31–33
To work independently with a foundation in education and competence
It emerged that district nurses with prescribing rights requested continuous education relating to prescribing.25–27,29–31 The right to prescribe motivated district nurses to increase their competence as the benefit of their knowledge and capacity was perceived positively by both patients and colleagues.25–27,29–32 More knowledge also led to positive personal development with better job security.28,33 District nurses experienced that the opportunities with the right to prescribe promoted independent thinking through increased knowledge and the possibility of greater responsibility.29,32 The district nurses were responsible for the entire diagnosis process, prescribing treatment, monitoring treatment, and evaluating the treatment.29,32
The patients received a thorough description of the drug treatment 29 as the district nurses had knowledge of the medication and could safely educate patients. Expert knowledge in pharmacology and disease theory strengthened district nurses' holistic approach.25–29
Clinical and theoretical continuous education opportunities were often limited in the workplace. District nurses expressed concern that they did not have time to keep updated on the subject and that they, therefore, did not make the right decisions, which contributed to a fear of feeling incompetent.25–33
The employer had an important role in whether the prescriber, through training, became confident in their prescribing role.26,27,31 The possibility of networking at the workplace, where experiences and knowledge about prescribing were shared, was requested. Lack of time during working hours to attend meetings, training, and networking was mentioned.26,27,31
Challenges with prescriptions
The workload was described as increased when district nurses had prescription rights. By taking over responsibility for more complex patients, the increased demand for competence was experienced as stressful. District nurses’ workload increased even if the patient's visit took longer. A challenge was also presented when there was, what the district nurse considered to be, too narrow of a limitation in the right of prescription. District nurses could then not prescribe the medicine they assessed the patient needed.
When the prescription of drugs results in an increased workload
District nurses experienced that the right to prescribe led to an increased workload in the form of more complex patient cases.25,27 This increased the need for knowledge in pharmacology and diagnostics.25–28,31 The stress increased further when duties were transferred from doctors to district nurses with prescription rights. In addition, the demand from colleagues who did not have the right to prescribe increased the workload and was perceived as a stress factor.25–28,31
The lack of time for consultations with patients was identified and experienced as a stress factor in the prescribing process. District nurses described the need for an extended consultation time with the patients, as prescribing could take longer during a visit to a district nurse.25,29 There were also experiences of administrative difficulties in registering the prescription, which could be time-consuming. 32 The district nurses also learned that the increased responsibility with drug prescriptions did not result in a higher salary or other rewards. They then felt undervalued, which could reduce motivation at work in combination with the increased workload.26,28–30,32
Limitations within prescribing
District nurses experienced the limitations of the prescription rights as a stress factor, culminating in less efficient work that developed into an obstacle to performing work tasks. Patients needed to receive the care and treatment they needed.29–31 The patients could, at times, need an understanding of which medications the district nurse was able to prescribe. The district nurses could then experience stress. Therefore, the desire to extend the right of prescription was brought forward.25,29,31,33 In the treatment of chronic diseases, district nurses requested the possibility of extending these continuous prescriptions.25,30 Studying further to expand their prescribing rights was described as a way of dealing with the existing stress factor. 25
Discussion
The result showed how important the prescription was to meet patients’ needs and provide holistic and person-centered care. The Swedish Nurses Association 37 confirms the results regarding person-centered care to achieve an individual treatment plan. Person-centered care is characterized by patients being seen and understood as individuals with individual needs, resources, values, and expectations. This is also in line with the study by Linmans et al. 35 regarding individually adapting the preventive health work where the district nurse starts from each patient's experiences to meet the patient's needs and conditions in consultation. Wilkinson et al. 36 argue that person-centered care will also lead to an increased long-term effect of treatment. According to Byrne et al., 34 person-centered care cannot be conducted if the nurse does not recognize the patient as unique and form meaningful partnerships, involve, and interact with the patient. In that way, the patient does not gain control and power over their care. Prescription rights make person-centered care more efficient, reducing patient suffering. This supports the results and shows the importance of individual treatment plans. Byrne et al. 34 see an obstacle in conducting person-centered care because modern-day nurses are tasked with more assignments and prescribing takes time away from the patients. As a result of less patient contact, nurses expressed inadequacy and stress, which promoted challenges in the follow-through of the individual treatment plan for the patients.
The results demonstrate how inadequate support from colleagues resulted in a lack of confidence in various medical areas required for prescribing. It is in consensus with Lim et al., 38 who found that clinical experience and mentoring are important to increase skill development in prescribing and should be advocated by all organizations that prescribe district nurses. The prescribing otherwise risks not being utilized, and instead may be associated with anxiety and the fear of making mistakes. 38 In previous studies, it has been shown that support can be crucial for professional growth and the development of clinical competence among prescribers.39–42 Support and feedback are required for all nurses to manage the complexity of care and feelings of incompetence and to develop a professional commitment. 43 The support of a mentor entails guiding a person towards success as it provides access to knowledge and strength. 44 The support from doctors is also an important component in securing district nurses in their role as prescribers through well-functioning teamwork between doctors and district nurses. Primary care does not always have these conditions as there is a shortage of general practitioners and experienced district nurses.19,45–48
It poses a problem if district nurses do not receive support as it can result in a limitation in using the already limited list of medication that district nurses are allowed to prescribe in Sweden. As district nurses have a limited number of medications they can prescribe with insufficient support, there is a risk that the right to prescribe may be eroded in practice. In consensus with the increasing shortage of doctors and nurses, as well as the aging of the population and the increase in the number of chronic diseases, the skills of nurses to prescribe medicines need to be utilized and stimulated to meet the need for care in primary care. In contrast, there may also be a risk with district nurses being given drug prescriptions as a delegated task. The result showed that this transfer of work tasks resulted in an increased workload and an increased experience of stress for district nurses, which was negative. District nurses accept the expanded assignment of work tasks partly due to the profession receiving better validation, with a higher status, when work tasks are moved in a medicine-centered direction, as Richards and Borglin 49 described. The prescription of drugs is also a career opportunity in the administrative department. This administrative career direction must be prioritized against the nurse's care work so that the nurse's core values of fundamental nursing care, according to Richards and Borglin, 49 are safe.
The increased demand for healthcare services coupled with a shortage of physicians leads to the need to transfer assignments and clinical tasks from physicians to nurses. 4 Through Advanced Practice Nurse (APN) training, it is possible to expand the role and function of a district nurse in primary care by being able to prescribe treatments, prescribe drugs, make diagnoses independently, and evaluate the results of the initiated treatment. 50 Today, APN is present in approximately 30 countries even though research shows that if APNs could prescribe drugs and order examinations, the benefit to the patient would be greater. 51
Summary of recommendations
Prescribing drugs is important for the professional development of district nurses. With the authority to prescribe drugs, district nurses can provide holistic and efficient care in which the patient can participate.
Through an extended prescription authority, district nurses can contribute to efficient care that can meet the future demand for healthcare services in primary care.
District nurses require support, mentorship, and continuous education in prescription authority.
The prescribing authority for district nurses should be further reviewed and developed to adapt to the current and future care needs of the population within primary care.
Methodological limitations
The reliability behind the study is that four databases were utilized. 21 As the databases were structured in varying ways, the help of a librarian was taken. The low number of articles found may indicate that there could be a knowledge gap in this domain that may reduce the value of the conclusion. Regarding the searches in the selected relevant databases, there is an imminent risk that all relevant research within the subject has not been included. At the same instance, the number of articles does not determine the value of the literature search. The most important factor is that the articles answer the purpose of the study, which they do. In the articles, similar results appear, which can be seen as a strength. The authors have jointly performed the analysis and interpreted the content, which increases credibility and reliability. A strategic selection was made with only qualitative articles, strengthening credibility.
Conclusions
The result shows that district nurses’ access to drug prescriptions leads to the patients receiving holistic and person-centered care, where the district nurse feels increased job satisfaction and professional pride. Furthermore, the results showed that the patients received more efficient care. The results showed how important continuous education and support from colleagues, doctors, and employers are to develop into a self-assured and competent prescriber. District nurses’ prescriptions of drugs in Sweden have not developed proportionately because the entire healthcare system has made great progress in many areas with task-shifting. The prescription of drugs for district nurses should be further reviewed to adapt to the population's current and future care needs. The district nurse authority to prescribe drugs is important to meet the populations need for care, but as district nurses now experience the prescribing of drugs in the current clinical context, changes need to be made and adapted to the prevailing clinical context. Action needs to be taken by national healthcare policymakers to develop the legalization of drug prescribing, alongside development in primary care and continued research.
Supplemental Material
sj-docx-1-njn-10.1177_20571585241227594 - Supplemental material for Independent and effective care – district nurses’ experiences of prescribing drugs: A systematic qualitative literature review
Supplemental material, sj-docx-1-njn-10.1177_20571585241227594 for Independent and effective care – district nurses’ experiences of prescribing drugs: A systematic qualitative literature review by Christina Hammarberg, Anna Abelsson, Aysel Arslan and Anna Willman in Nordic Journal of Nursing Research
Footnotes
Author contributions
Design: CH, AyAr, and AW; data collection: CH and AyAr; analysis: CH, AnAb, and AW; drafting the paper: CH had the main responsibility, AnAb, AyAr, and AW. All authors read and provided substantial input to the final version of the paper. All authors have approved the version to be submitted.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, private or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.