
Abstract
Nurses need moral courage in their ethical decision-making. As a personal characteristic, moral courage varies between individuals. The aim of this study was to analyse nurses’ self-assessed moral courage, morally courageous acts and associated individual factors in older people care in one large city in Finland. The data of this cross-sectional study were collected with the ‘Nurses’ Moral Courage Scale’ (NMCS) and the main analyses were conducted with multi-way ANOVA. A total of 205 nurses responded. Respondents’ self-assessed moral courage was 4.16 on a Likert scale of 1 to 5. Higher moral courage was associated with a higher knowledge base in ethics, more frequent encountering of ethical conflicts and having several sources for knowledge of ethics, suggesting that providing ethics education for nurses in the care of older people is important. The STROBE checklist was used as the reporting guideline for the manuscript.
Background
The present study focuses on nurses’ moral courage in ethical conflicts in the care of older people. Moral courage forms an important part of nurses’ ethical and professional competence1,2 and is a personal characteristic and a virtue. 3 Moral courage has been defined as the courage a person has when acting according to ethical principles in ethical conflicts, even at the risk of negative outcomes for the acting person. 4
Registered nurses and practical nurses need moral courage as a part of their ethical competence 5 in their ethical decision-making, for fulfilling their ethical responsibilities in the care of older people.6,7 Despite their different responsibilities in clinical work, both professional groups have an ethical responsibility to promote patients’ health, provide care with ethical quality, and ease and prevent suffering. Responsibilities, however, can vary according to their professional duties.8,9
In the care of older people, ethical conflicts are often related to challenges with shared decision-making, with patients regarding their treatment, lack of care or treatment, or inequity in accessing adequate care. 10 Ethical conflicts directly related to patients can be the patients’ compromised autonomy and conflicts of opinion between professionals and patients or their next of kin. 11 Morally courageous nurses can identify and solve ethical conflicts. Nurses’ moral courage can promote the ethical quality of the care of older people 7 because the care focuses on basic needs and support in daily activities. 10
Research regarding nurses’ moral courage has increased in recent years. 12 It has been studied in tertiary level hospitals, 5 education, 13 and in a combination of contexts 1 from the perspectives of registered nurses1,14 and registered nursing students. 15 Earlier research on nurses’ self-assessed moral courage has indicated that nurses have a rather high level of moral courage in varying contexts, but thus far the research has not been focused on the care of older people as a part of public primary healthcare. The higher level of nurses’ moral courage has been associated with age, 16 professional competence, 15 knowledge base in ethics 14 and earlier experiences in life and work. 1 Personal interest in ethics and self-studying has also been related to a higher level of self-assessed moral courage. 14 On the other hand, work-related exhaustion, 1 moral distress 17 and negative experiences from earlier ethical conflicts 1 have inhibited nurses’ moral courage.
The present study focuses on analysing nurses’ moral courage in older people care, which is a central part of primary healthcare. 18 Ethical conflicts in the care of older people and the importance of moral courage have been discussed in the literature, thus it is justified to study moral courage in this context. 10 Nurses can stand up for patients’ rights and safeguard quality care with morally courageous acts, making moral courage an important part of ethically sound nursing.1,11 Thus, it is relevant to study nurses’ moral courage and to analyse which individual factors are associated with higher levels of it. Understanding the associated individual factors is relevant because nurses’ individual ethical decision-making is an essential part of their morally courageous acts.1,7 Furthermore, identifying associated individual factors enhances the understanding of nurses’ moral courage, which is important from the perspective of maintaining and promoting both quality care and nurses’ moral courage.
Aim and research questions
The aim of the present study was to describe nurses’ self-assessed moral courage in the care of older people as part of public primary healthcare.
Research questions
What is the nurses’ level of moral courage in care of older people?
Which individual factors are related to nurses’ moral courage in the care of older people, if any?
Methods
Research design
This was a descriptive cross-sectional study, set in the care of older people in a public primary healthcare organisation in a large Finnish city. The reporting follows the STrengthening the Reporting of OBservational studies in Epidemiology guideline for cross-sectional studies (STROBE). 19
Study context
The data were collected in a large Finnish city in municipal hospital wards, home hospice and home care, which are targeted mainly for older people. These services are provided in publicly funded primary health- and social care in Finland. A large city was selected to obtain respondents from diverse contexts of older people care. 20 A variety of nursing professionals work very close to the patients in the selected long-term and short-term wards and home care units.21,22 In home care, the clients need care and assistance in many areas of everyday life, such as medication, nutrition and mobility, and most of the clients need long-term care. 22 Studying nurses’ moral courage in this context is important because of its central role in primary healthcare. Nurses can solve ethical conflicts with morally courageous acts, and thus promote ethical quality of care. 12
Population
The population in this study comprised registered nurses and practical nurses. Both professional groups were included, because they work closely together in the care of older people, sharing responsibilities of the patients’ daily basic care. In addition, in this context, the number of practical nurses exceeds that of registered nurses. 21 In Finland, approximately 21% (15,000) of ∼71,500 registered nurses and approximately 48% (36,500) of ∼75,500 practical nurses work in municipal primary healthcare. Of the registered nurses in primary healthcare, 63% (∼9500) and of the practical nurses, 41% (∼15,000) work in municipal hospital wards, home hospice or home care, which were the types of nursing units included in this study. 23 In Finland, education for registered nurses in universities of applied sciences, being public limited companies, follow the EU directive that regulates the contents and duration of the studies. 24 The studies comprise 210 ECTS, which equals 3.5 years of studying and leads to a registered nurse degree and registered nurses are licenced professionals. 25 Practical nurses, then, are educated in municipally arranged vocational institutes. The training comprises 180 competence points, equalling three years of full-time studying and leading to a vocational qualification and a protected occupational title. 26 Practical nurses’ work is focused mainly on basic care and assisting patients in their daily activities. 27
Sampling
A purposive sampling method was implemented to gain a representative dataset large enough for statistical analyses. 28 The sample size estimation of 270 respondents, achieving a confidence interval of ±0.06 from the sample mean, was based on the confidence interval width of moral courage in the scale validation study of ‘Nurses’ Moral Courage Scale’ (NMCS; ©Numminen). 29
All 680 nurses working in the municipal hospital wards, home hospice and home care units in the selected city were offered a possibility to participate in this study, if they assessed themselves to meet the eligibility criteria: (1) registered nurse or practical nurse; (2) working in the selected primary healthcare units; and (3) a sufficient level of Finnish language needed to complete the questionnaire, which the respondents self-assessed. The researcher (E.P.) visited each organisation before data collection, informed the contact persons about the study and provided information about the study for the potential respondents.
Data collection
The data were collected with paper-and-pencil questionnaires in October 2020, during a four-week period in each ward and home care unit. Contact persons, appointed by the organisation from each unit, informed potential participants about the study, handed out the questionnaires and collected them after the data collection time was over. Participation was voluntary. Contact persons reminded possible respondents about the study and allocated time to complete the questionnaire during working hours as an attempt to avoid non-response biases. It was also possible to complete the questionnaire at home and return it in a sealed envelope.
The data were collected with the NMCS, which measures nurses’ moral courage. The NMCS was developed for the nursing context and has been shown to be reliable and valid.14,30 The NMCS comprises 21 items, and the responses were given on a Likert scale from 1 to 5, as follows: 1 = does not describe me at all; 2 = describes me a little; 3 = describes me on average; 4 = describes me fairly well; and 5 = describes me very well. The NMCS was divided into four subscales according to dimensions of moral courage: Compassion and true presence (5 items); Moral responsibility (4 items); Moral integrity (7 items); and Commitment to good care (5 items). 29
Individual factors in the questionnaire were age, gender, highest educational degree, length of work experience in healthcare, current work position, current working unit, knowledge base in ethics, sources of the knowledge, participation in ethics-related activities in work and frequency of encountering situations requiring moral courage. The variables ‘highest degree’, ‘current work position’, ‘sources of the knowledge of ethics’, ‘description of participation in ethics-related activities’ and ‘different ways of acting morally courageously’ also included the option ‘other’. Additional items in the questionnaire were easiness or difficulty to confront other professionals or organisation, patient or patients’ next of kin and ways to act morally courageously: discussion with care team; filing a notification within one's organisation; blowing the whistle to an outside body; or other action, which were also assessed with a 5-point Likert scale. These items were also included in the questionnaire with the originally published NMCS, 29 and they were included in this study to add knowledge about easiness or difficulty to act morally courageously when confronting different individuals or organisations and acting morally courageously in different ways.
Statistical analyses
The categorical variables were summarised with frequencies and percentages and the continuous variables with means, standard deviations (SD) and range. Age and work experience were categorised. The overall moral courage score was generated as the mean value over 21 items; similarly, four subscales were programmed based on the subscales determined in the scale validation study. 29 The higher the mean value for the total or subscale, the higher the moral courage. In addition, even though individual items were collected on a 5-point Likert scale, only total and subscale means for moral courage were analysed. Then, the mean values behaved as continuous variables, and after modelling fulfilled the needed assumptions.
The level of moral courage was estimated using means and 95% confidence intervals, and one-way analysis of variance (ANOVA) and covariance were used to analyse the associations between moral courage and individual background factors. For multivariable modelling, significant explanatory variables were included as follows: self-assessed level of knowledge base in healthcare ethics (excellent, good, satisfactory); how often the participants encountered ethical conflicts (never/rarely; often/very often as combined); and the number of sources of the knowledge of healthcare ethics (1–4) was analysed using multi-way ANOVA. The same model was applied to respondents’ Numeric Rating Scale (NRS) assessment of moral courage, which was used as a confirmation about the participants’ self-assessment of their moral courage after answering all items in the main NMCS.
If a respondent had a missing value either in his/her response or in the explanatory variables, the respondent was automatically removed from the analysis concerning that item or subscale. The assumption for normality was checked with studentised residuals. No imputation for missing values was made. No sensitivity analyses were performed. The reliability of the instrument was assessed with Cronbach's alpha. p < 0.05 (two-tailed) was considered to be statistically significant. The data were analysed with SPSS for Windows version 26 30 and SAS version 9.4 of the SAS System for Windows software. 31
Ethical consideration
Ethical principles for research were followed. 32 Ethical approval was received from the ethics committee of the university (dated 27 January 2020) and research permission was granted by the participating organisation. Permission for using the instrument and editing background variables regarding gender, working unit and professions was received from the copyright holder. All invited respondents received an information letter and a PowerPoint presentation with an explanatory video about the study process, voluntary participation, data protection and their right to withdraw from the study. Completing the questionnaire was considered a voluntary informed consent of participation. 32
Results
Respondents
A total of 205 nurses completed the questionnaire (response rate = 30%). At the item level, there were 0–5 missing values. However, when subscales were calculated as the mean values of item responses, respondents with missing value(s) also received the value for the subscale. The respondents’ mean age was 42.1 years and their mean working experience in healthcare was 12.6 years. Three-quarters (n = 153, 74.6%) worked in home care or home hospice. The majority (n = 139, 69.8%) assessed their knowledge base in ethics to be good, and more than half (n = 118, 57.6%) assessed that they sometimes encountered ethical conflicts. Ethics-related activities in the respondents’ work were discussion forums for ethics, lectures on ethics and development projects (Table 1).
The respondents’ characteristics (n = 205).

Note. Values are given as n (%).
Self-assessed level of moral courage
The levels of registered nurses’ (mean = 4.14 ± 0.53) and practical nurses’ (mean = 4.18 ± 0.62) moral courage did not vary significantly (p = 0.679), thus the groups were analysed together. In the combined group, the mean level of nurses’ moral courage in the 21-item NMCS was 4.16 ± 0.58, with the highest (4.38 ± 0.61) being ‘Compassion and true presence’ and the lowest (3.96 ± 0.7) ‘Moral responsibility’ (Table 2). On the item level, the highest mean (4.65 ± 0.59) was in ‘I admit my own mistakes in care’ and the lowest (3.70 ± 1.03) in ‘If I observe evident shortcomings in someone else's (colleagues, other health care professionals, physicians, patient's next of kin, the patient, or the organisation where the nurse works) professional competence I bring it up for discussion’. The mean NRS (scale of 1–10) assessment of moral courage was 8.20 ± 1.27 (range = 5–10).
Moral courage in the combined group of nurses (n = 205).
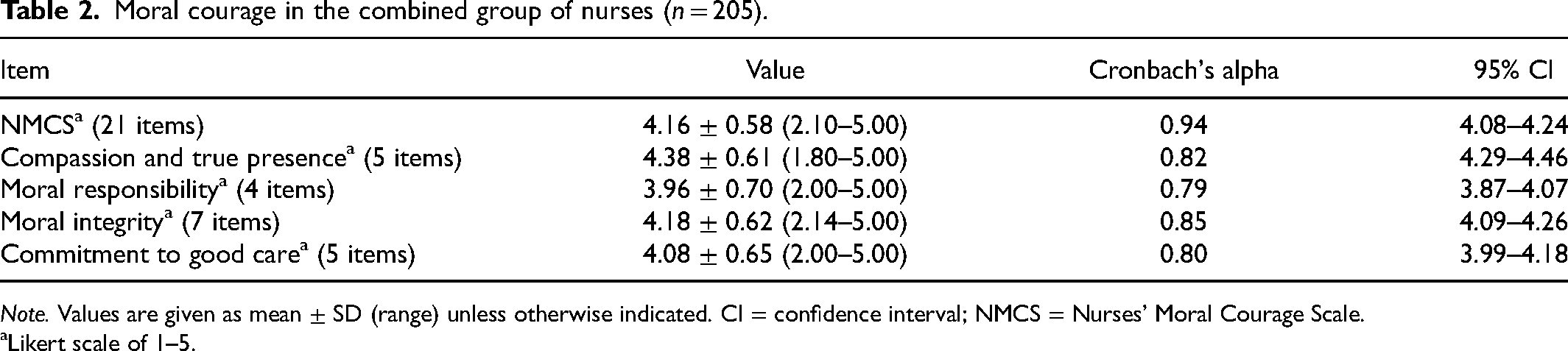
Note. Values are given as mean ± SD (range) unless otherwise indicated. CI = confidence interval; NMCS = Nurses’ Moral Courage Scale.
Likert scale of 1–5.
As for nurses’ morally courageous acting, defending ethical principles against another nursing professional was assessed as the easiest (4.18 ± 0.76) while defending ethical principles against the organisation, for example an executive nurse, while where one works was the least easy (3.22 ± 1.04). Furthermore, opening discussion with care team was the easiest (4.26 ± 0.76) way to act morally courageously, with the least easy (3.06 ± 1.16) being to ‘blow the whistle’ to an outside body, such as the public authorities. Informing and discussing with patients’ next of kin and informing staff nurse or managers higher in the organisation were other ways of acting courageously mentioned in answers to the open question (Table 3).
Additional items regarding easiness or difficulty to act morally courageously in the combined group of nurses.
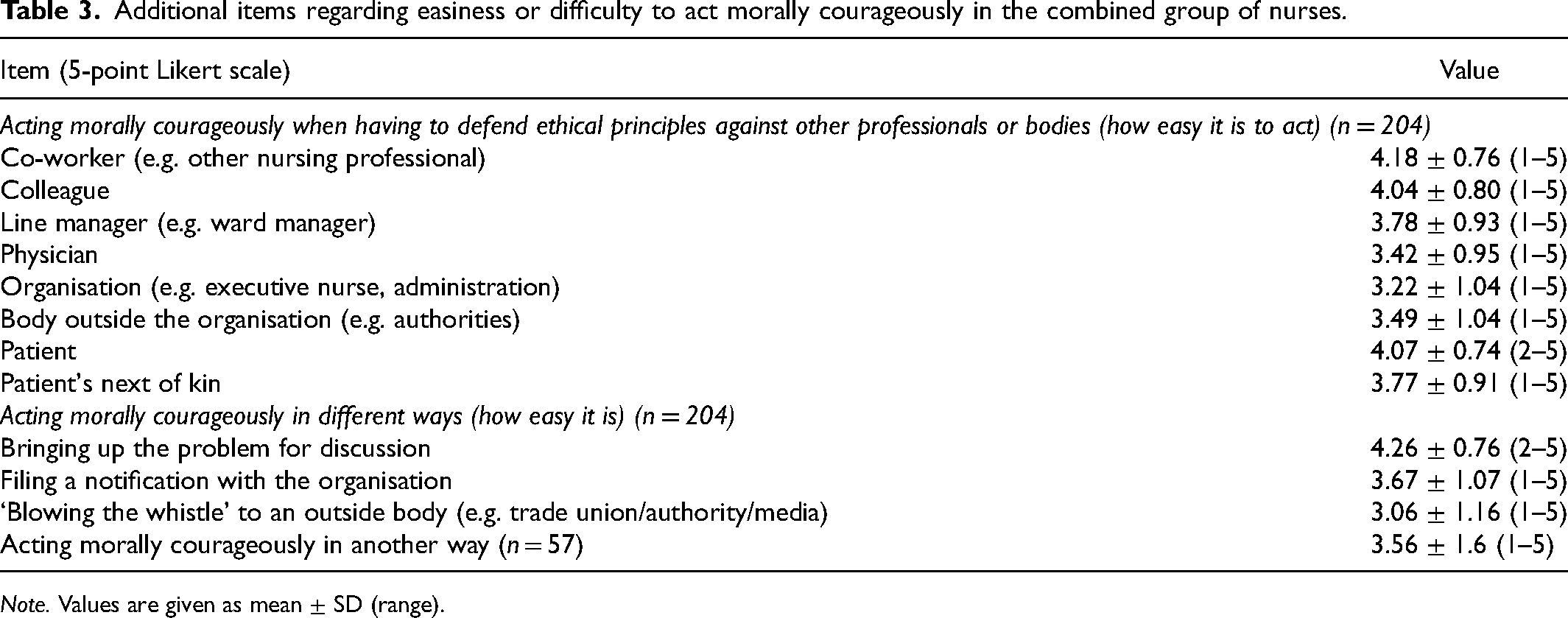
Note. Values are given as mean ± SD (range).
Relationship between moral courage and individual factors
In univariate analysis, the respondents’ age was significantly positively (p = 0.034) associated with their NRS (scale of 1–10) assessment of moral courage and their moral responsibility (p = 0.023). In addition, a higher level of moral courage in the NMCS was associated with a higher level of knowledge of ethics, obtaining knowledge of ethics from self-study, from ethics education and in practice, and encountering ethical conflicts frequently. These associations remained prominent in the multivariate analysis where sources of the knowledge were examined as a sum of how many sources were used (range = 1–4) (Table 4).
Associations between higher level of moral courage and ethics-related background factors (multi-way analysis of variance).

Note. NMCS = Nurses’ Moral Courage Scale; NRS = Numeric Rating Scale.
As for associations in univariate analysis between individual factors and self-assessments regarding morally courageous acting, respondents who had a higher knowledge base in ethics also assessed their moral courage to defend ethical principles against a co-worker (p = 0.034), line manager (p = 0.021), patient (p = 0.017) and patients’ next of kin (p = 0.001) as higher. They also assessed opening a discussion with the care team (p < 0.0001) and filing a notification with the organisation (p = 0.001) as easier.
Discussion
The present study produced new knowledge of moral courage of the combined group of registered and practical nurses, working side by side in the care of older people. In addition, new knowledge was produced of individual background factors associated with nurses’ moral courage, and their self-assessed easiness or difficulty to act morally courageously in varying ethical conflicts. Studying nurses’ moral courage in this context was essential because moral courage has been suggested as one solution to achieving individual people-centred care, which is a goal in primary healthcare. 18 Selecting this context was also relevant because patients’ health and well-being is maintained there, which often prevents a need of specialised treatment. Thus, quality care promoted with nurses’ moral courage can decrease patients’ suffering and prevent unnecessary use of society's resources.11,18
The main results are the strong associations between moral courage and knowledge base in ethics, sources of the knowledge of ethics and encountering situations requiring moral courage frequently. It is notable that the respondents’ self-assessed moral courage was at a rather high level, which indicates the respondents’ high responsibility in ethically sound practice.14,33 It is also encouraging that nurses in older people care had the confidence to try to solve ethical issues with morally courageous acts. It suggests that nurses are willing to provide care with good ethical quality, even at the risk of negative consequences for themselves. In the studied context, working close to the patients provide a viewpoint for identifying ethical conflicts, such as the inability to provide quality care according to older people's needs 34 or problems in communication with patients or their next of kin.11,34 Having skills and abilities to solve ethical conflicts have been indicated to be important in primary healthcare, 34 making nurses’ moral courage a key element in safeguarding quality care when courage is needed. 5
The subscale means and NRS assessments of moral courage were both rather high and in line with earlier research; 35 the NRS assessments thus strengthen the findings from the 21-item scale. However, the samples are not fully comparable due to the respondents’ different educational backgrounds, because practical nurses were not included in earlier studies. 12 Furthermore, all subscales had a relatively high mean, including the lowest, moral responsibility. This is an important finding from the perspective of nurses’ work-related well-being, as nurses in older people care have earlier been reported to feel successful and satisfied after being able to solve ethical conflicts with the help of professional codes of ethics and their own competence. 7
As for acting morally courageously when confronting different individuals or organisation, confronting a co-worker was the easiest. It seems logical, because opening a discussion regarding ethical conflicts with colleagues has been identified as easier compared to more distant professionals 5 and it is often the first morally courageous act when a wrongdoing is identified. 36 Thus, collegial teamwork in ethical conflicts is also crucial in older people care. Making decisions to act morally courageously in a team can be beneficial for nurses’ moral courage. 37
However, confronting line managers and physicians was assessed as more difficult, suggesting that developing organisational structures that enhance different professionals working together in ethical conflicts could be beneficial for nurses’ moral courage.1,38,39 In addition, physicians and line managers being more distant in the organisation can make it more difficult even for morally courageous nurses to open a discussion about ethical conflicts. 38 Thus, it is important to ensure that organisational structure and collaboration between professional groups enhance nurses’ morally courageous acts when promoting quality care. 7 However, it is good to remember that ethical conflicts between people always have a topic or a reason. This was not the focus of this study, however, and would be an important topic for further research.
As for the associated individual factors, the strong associations between moral courage and ethics-related factors indicate the importance of adequate ethics education 29 and individual motivation for moral courage. 1 Nurses’ moral courage in the care of older people can benefit from both theoretical and practical education in healthcare ethics, which nurses themselves have indicated to want. 34
Furthermore, moral courage can be a natural part of a self-regulative nurse who believes in oneself, thus a nurse's own motivation and will to do good to others is very important for their moral courage. 1 Working independently, taking responsibility of the patients’ care and earlier successful actions in ethical conflicts can add to the nurse's strength to act morally courageously in older people care. 7 Thus, as a morally courageous act requires moral deliberation and an individual decision, 1 nurses themselves can promote their own moral courage, for example in the following ways: they can listen to their co-workers and discuss ethics with them; develop their own skills in ethics by participating in ethics-related education; and take responsibility for maintaining good ethical quality of their work. 2
Implications for clinical practice
Education, such as workshops, focusing on solving ethical conflicts with a multi-professional care team could be beneficial and enhance a good ethical climate in older people care.11,34 In the workshops, nurses and other professionals with both positive and negative experiences from acting with moral courage could share their experiences and the learners could gain more confidence for acting morally courageously. 34 In addition, a multi-professional collaboration in ethical conflicts in older people care and a functioning interaction between professionals could be beneficial for nurses’ moral courage and thus promote the actualisation of patient's rights. 34
Implications for further research
First, studies with large samples in different contexts could identify potential contextual and organisational differences in nurses’ moral courage, enhancing the development of environments that could promote nurses’ moral courage. Second, designs with smaller samples, such as case studies or narrative studies, could enable gaining new knowledge of how and why a nurse’s morally courageous act manifests itself. Finally, multidisciplinary studies, for example to gain an educational, philosophical, psychological or sociological perspective, could provide new viewpoints of nurses’ moral courage and enhance developing support for maintaining it.
Topics for further research with the above-mentioned designs could include nurses’ inner motivation for moral courage, associated organisational factors and educational interventions for promoting nurses’ moral courage.
Strengths and limitations
The strengths and limitations of this study are related to sampling, instrumentation, and handling and analysing the data. The purposive sampling method contributed to the aim of gaining a sample consisting of a typical nurse workforce in the care of older people in Finland. With women as the dominant gender, practical nurses was the largest group of professionals, and the mean age of the sample corresponded to nursing in public primary healthcare in Finland. 40 In addition, the definition of moral courage was given twice in the questionnaire to clarify what is meant by the concept in this study. This contributes to the reliability of the results, and has a specific importance related to the rather complicated concept.
As for the data analysis, all tests were conducted rigorously in cooperation with a biostatistician, acknowledging both the analysis in general and the missing values. In addition, our biostatistician checked the residuals after modelling, and they did follow normal distribution. There were only a few missing values in the data, which allowed us to include all returned questionnaires in the analysis. 41 The internal consistency of the NMCS in this study was at a desirable level based on Cronbach's alpha 42 and the study reached a satisfactory accuracy for assessing moral courage. 42
As for the limitations, the response rate was relatively low, which is a rather common limitation in contemporary survey studies. 43 However, the sample size was large enough for statistical analyses. The data were collected during the COVID-19 pandemic, which may have contributed to the relatively low response rate as the participants were nurses who may have been working with COVID-19 patients and been under an uncharacteristically heavy workload. 44
The possibility of social desirability bias should be acknowledged when drawing conclusions from the results. Nursing care aims for good quality and the best possible outcome for the patients, which may have made the respondents answer according to what they thought was desired of them instead of what they think or do. 45 In addition, it is possible that nurses who are especially interested in ethics decided to participate in this study, which can be related to the rather high self-assessments.
Conclusion
It is encouraging that the respondents assessed their level of moral courage to be rather high, suggesting that they are willing to promote a good ethical quality of care. Based on these results, it is important that nurse management is open for discussion about ethical issues and that adequate training in ethics is provided in organisations to maintain nurses’ moral courage. Furthermore, nurses themselves can boost their own moral courage with motivation and self-education as well as handling ethical conflicts in multi-professional cooperation in the care of older people.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.