
Abstract
Contact nurses in cancer care were vital in sustaining cancer care in Sweden during the COVID-19 pandemic. The aim of this study was to investigate their experiences of providing care to people with cancer in these exceptional circumstances to identify emerging challenges and opportunities that must be addressed moving forward. A survey distributed to contact nurses was supplemented with questions regarding the pandemic. The study design was a cross-sectional survey, analyzed with descriptive statistics and content analysis, reported in accordance with STROBE. Almost half of respondents (n = 337) reported not being able to provide the same support as before the pandemic. Analysis of open-ended question responses (n = 232) revealed a main theme: Altered prerequisites for providing care. Three categories related to altered interaction, accessibility, and nursing reality were revealed. Thorough reflection is needed to make use of lessons learned and avoid sustaining the short-term solutions needed to cope with the acute phase of the pandemic.
Background
The COVID-19 pandemic has affected cancer care worldwide, with rapid reorganization, modified risk management strategies and changes in decision-making structures.1–3 Paterson et al. 4 describe how oncology nurses have a pivotal role in providing care and management to people affected by cancer during the pandemic. In Swedish cancer care, contact nurses in cancer care (henceforth referred to as contact nurses) 5 are interesting stakeholders to consider when exploring how cancer care has been affected by the pandemic. Contact nurses occupy a unique and central position in the care team and their insights are invaluable as we approach a new post-pandemic era of cancer care.
Advanced nursing roles in the oncology field have been developing in many parts of the world in an endeavor to improve patient satisfaction and health outcomes.6,7 In Sweden, a national cancer strategy was launched in 2009. 8 Based on the principles outlined in the strategy, which emphasized the importance of continuity of care and patient participation, the systematic implementation of the new contact nursing role was initiated and formalized through the formation of six regional cancer centers, which support the 21 regions in Sweden in charge of healthcare provision. There is a national description of what constitutes the contact nurse assignment: it includes being directly available to their patients, informing patients of the coming steps in the clinical trajectory, making evidence-based assessments of patients’ needs, supporting patients and significant others in normal crisis response, and ensuring patient participation. 9 The contact nursing role is specifically adapted to the Swedish cancer care organization but bears a resemblance to the role of an oncology nurse navigator or clinical nurse specialist in cancer care in other settings.7,10 For example, core competencies of an oncology nurse navigator include coordination of care, communication and education, 7 and important tasks for the clinical nurse specialists have been described as eliminating barriers to care, being accessible to patients and their relatives, involving patients in the planning of care, and assessing needs. 10 Previous evaluations have shown that patients diagnosed with gynecological, hematological, head and neck, and upper gastrointestinal cancers benefit from having access to a contact nurse. 11 Notably, another Swedish study points to the fact that only 50% of patients reported having access to a contact nurse. 12 The care provided by contact nurses has been shown to be unequal across Sweden, where some regions and institutions have provided opportunities for staff to work in accordance with the national description of the contact nurse assignment, whilst others are far from promoting this. 5 Even if ongoing work to improve the quality and implementation of this function in cancer care is in progress, further information on which prerequisites are needed to fulfil the assignment with high quality is required. Many of these prerequisites were also affected by COVID-19. This study thereby aims to investigate Swedish contact nurses’ experiences of how COVID-19 has affected their ability to provide care and support to persons affected by cancer, in order to identify challenges and lessons that need to be addressed as the pandemic subsides.
Method
Setting
The national study, Quality in care, Organization and Pre-requisites for Contact Nurses in cancer care (QOPCoN), is investigating the prerequisites, work tasks and effects on care of the contact nurse function, aiming to inform decision-makers and to further the contact nursing role in Sweden. This study is based on survey responses from contact nurses in Sweden and is part of QOPCoN. Other findings from the larger QOPCoN study will be presented elsewhere. The manuscript is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 13
Sample
The aim was to conduct a total survey of all contact nurses in Sweden during the study period. The inclusion criterion was therefore those having the special assignment of contact nurse in Swedish cancer care. The estimated number of contact nurses working in cancer care in Sweden is approximately1500–1800. However, this figure fluctuates constantly and there is no register available, making it difficult to provide exact numbers and contact details.
Data collection
The initial survey consisted of a study-specific set of questions and the Stress of Conscience Questionnaire (SCQ). 14 The study-specific questions concerned the demographic and educational variables of the contact nurses, and questions regarding their employment, working conditions and work tasks.
With the intention to reach all contact nurses, a modified convenience sampling method combined with additional snowball sampling was applied. The survey was distributed electronically to contact nurses between March and April 2020. The means of distribution varied across regions. In some regions, the link to the survey was passed on to eligible participants through the regional cancer centers, in other regions, via managers at the hospitals. Managers had given their approval prior to the survey's distribution. Participation was accepted by opening the link after receiving written electronic information about the study. Participants were encouraged to suggest other contact nurses to be invited. If a new participant was suggested, a separate email with the link was sent to that person.
Just after the launch of the QOPCoN study, COVID-19 spread globally and gained momentum in Sweden during March of 2020. Consequently, researchers were restricted from collecting data from staff in clinical work, and the study was forced to pause. As it became clear that the COVID-19 pandemic would have substantial effects on cancer care provision, the survey was supplemented with a set of questions relating to the pandemic's effect on the contact nurses’ care provision. When the ban on reaching out to clinical staff was lifted, the survey was distributed again between September and December 2020. Two reminders were sent through the same channels of distribution.
Data analysis
Quantitative data
The subset of data covering the effects of COVID-19 on cancer care included closed questions combined with one open-ended question. Closed questions were analyzed using descriptive statistics. Descriptive statistics were performed using SPSS (IBM Corporation, 2019).
Qualitative data
The open-ended question was analyzed using qualitative content analysis inspired by the method proposed by Graneheim and Lundman 15 and previous studies using qualitative analysis for analyzing open-ended survey questions.16,17 The software utilized for analysis was Microsoft Excel (version 13127.21348). All answers were read through multiple times to get a sense of the whole. Longer replies were condensed into meaning units based on the manifest content. Meaning units were then further condensed with the ambition of maintaining the core meaning from the original statements. Meaning units were coded in an iterative manner, where suggested codes were checked against both the condensed meaning and, when deemed useful, the original meaning unit, to assure a logical connection. Codes were sorted into subcategories and categories based on their manifest content. In accordance with Graneheim and Lundman, 15 categories were developed to sort data into exhaustive and mutually exclusive groups. The categories and subcategories were revised and developed in a dialogue between all authors and the data. Through this, a main theme emerged, defined as a thread of underlying meaning, found through condensed meaning units, codes and categories. 15
Ethical considerations
The study was approved by the Swedish Ethical Review Authority (Diary number 2019-04958).
Results
Respondents
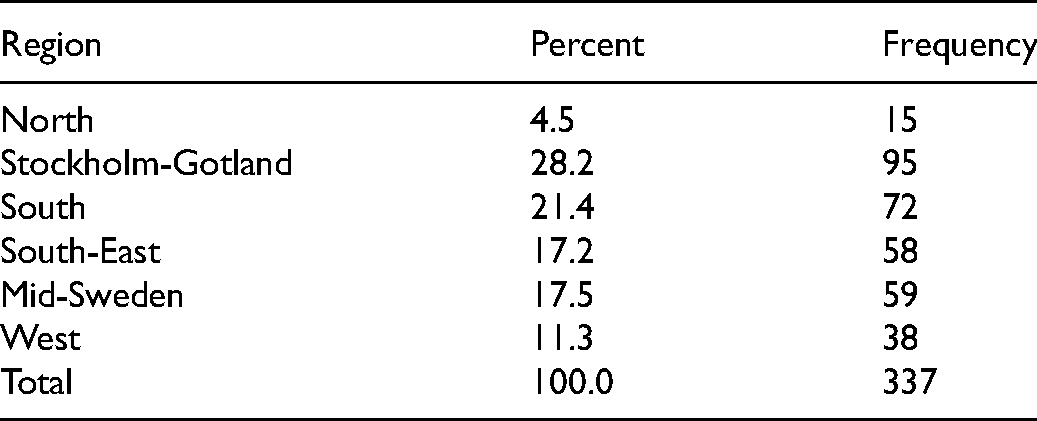
A total of 535 contact nurses answered the survey. After the re-launch of the survey with the addition of the COVID-19 questions, 337 respondents replied. Respondents were distributed across the country and served different diagnosis groups. They were employed at both university and county hospitals. The characteristics of respondents are presented in Table 1, and distribution of respondents across the six regional cancer center regions is shown in Table 2.
Characteristics of survey respondents.
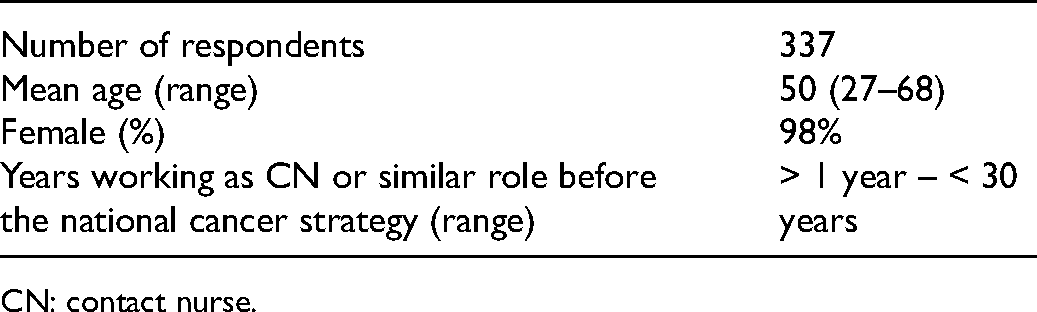
CN: contact nurse.
Distribution of participants across Sweden.
The contact nurse function during the pandemic
One-hundred-and-sixty respondents (47.5%) reported that they were either only partly able (n = 120, 35.6%) or unable (n = 40, 11.9%) to fulfil their assignments as contact nurses to the same extent as before the pandemic (see Table 3).
Descriptive statistics of closed survey questions.

CN: contact nurse.
One-hundred-and-fifty-four respondents (45.7%) reported that they could not provide the same level of psychosocial support to patients as before the pandemic. Furthermore, 178 respondents (52.8%) reported that they could not provide the same level of psychosocial support to significant others (see Table 3).
Two-hundred-and-twenty-two respondents (65.9%) reported that they were in charge of roughly the same number of patients during the first half of 2020 as prior to the pandemic, 47 (13.9%) were in charge of an increased number of patients, and 100 (20.2%) were in charge of fewer patients than usual.
Deepening the understanding of the contact nurse function during the pandemic
Of the 337 respondents, 232 provided answers to the open-ended survey question: ‘How did the COVID-19 pandemic affect the care that you as a contact nurse provided to your patients during the spring and summer of 2020?’ An overview of the qualitative content analysis of the open-ended survey question is presented in Table 4. It consists of three categories (Altered interaction, Altered accessibility and Altered nursing reality) and seven subcategories. The categories and subcategories are encapsulated in the theme, Altered prerequisites for providing care, elucidating how the game plan for cancer care was suddenly altered, forcing its parties to relate to the rapidly evolving and uncertain situation posed by the pandemic. The results are described in more detail below and are enhanced with illustrative quotations from respondents for each category.
Overview of qualitative results: theme, categories and subcategories.

Categories and subcategories
Category: altered interaction
The most pronounced alterations caused by the pandemic were found in the shift in interactions between contact nurses, patients and their significant others.
Subcategory: altered means and quality of interaction
A recurring experience was the shift in how contact nurses interacted with patients and significant others. Face-to-face interactions were mainly restructured to take the form of phone calls and, in some instances, video meetings. Although some noted benefits of such distance meetings, other testimonies highlighted difficulties in providing sufficient care and support through these modes of interaction, affecting the quality of care. Foremost to not be able to give physical contact, to console by placing a hand or a hug … (Contact nurse in cancer care, district hospital)
Furthermore, the alterations in communication made some respondents increasingly uncertain in their assessments of the patient's symptoms, invoking a fear of missing significant clinical findings.
Another aspect of alterations in interaction concerned significant others specifically. Contact nurses described how their interactions with significant others were significantly reduced due to restrictive visitation policies and the general changes in modes of communication. The otherwise natural physical access between significant others and respondents in the hospital setting was eliminated to prevent the spread of the disease.
Subcategory: altered support needs
The second subcategory concerned contact nurses’ perceptions of patients’ support needs. Because of the many uncertainties of the pandemic and the fact that opportunities for significant others to support patients during treatments and visits were limited, respondents experienced that both patients and significant others were more worried and had greater and different support needs than prior to the pandemic: It is not the same thing as having a personal contact. Many patients were very lonely, isolated, and had a greater need for emotional support. (Contact nurse in cancer care, private hospital|)
Category: altered accessibility
The data suggest that care accessibility was altered due to the pandemic.
Subcategory: alterations initiated by healthcare
A recurring experience described by the respondents was that the pandemic altered healthcare processes, affecting accessibility and the care that patients received in various ways. Respondents described decreased accessibility and impaired overall continuity. A common experience was that personnel were relocated to other assignments, either partially or fully, resulting in delays and cancelled care. There were also accounts of changes to routines and to the medical treatment provided to patients in order to decrease interaction and to prevent the spread of disease. Examples of changes in treatment included switching to administering chemotherapy in tablet form instead of intra-venously, having patients carry out wound care at home with support from a contact nurse over the phone, and using less precise image diagnostic tools to avoid trips to a larger hospital.
Subcategory: alterations without impact on patient care
Although many respondents suggested that care provision had been greatly affected, a common experience was also that care provision to cancer patients was not affected by the alterations imposed upon healthcare because of the pandemic, and that care could be provided as before: Not when it came to the patients, but there was a lot of re-arranging in order to be accessible to the same degree, since colleagues were relocated … (Contact nurse in cancer care, district hospital)
Additionally, there were also a few accounts of increased efficiency in care processes, as cancer patients were highly prioritized.
Subcategory: alterations initiated by patients
Alterations were not only initiated by the healthcare system, but also by patients. Respondents described that many patients were afraid or unwilling to visit the hospital, considering the risk of infection and the new regulations prohibiting significant others from accompanying them. This prompted providers to explore new ways of catering to their patients’ needs. Exemplifying this is the account of a respondent describing how patients wished to die at home, where they could be with their significant others, rather than alone at the hospital: More support, coordination, with the home care units so that they (patients) could remain at home at the end of their life, since admission to hospital meant no visitors allowed. (Contact nurse in cancer care, county hospital)
Category: altered nursing reality
Respondents reported having been personally affected by changes in their work situation brought on by the pandemic. Accounts of stress, stress of conscience, increased workload, relocations, and new tasks were identified throughout the data. Practical issues, such as new and troublesome safety equipment, affected the contact nurses and their everyday working conditions: A bewildering situation. I hope my patients have received the care and support they have a right to. I did my best to be there for them and for everyone I have been in contact with. (Contact nurse in cancer care, private hospital)
Everything went much faster. Our unit got all the accessible capacity for surgery in the region, which meant we processed all patients much faster than normal and ‘chased’ through preoperative processing. Incredibly stressful and associated with fear of missing something and that something would go wrong. (Contact nurse in cancer care, university hospital)
Main theme
Altered prerequisites for providing care
A latent undertone identified throughout codes, subcategories and categories is that the care provided by contact nurses during the spring and summer of 2020 was given in the shadow of the threat of the pandemic – it altered the prerequisites for providing care. Even though adaption seems to have been unavoidable, there was significant variation regarding the degree to which these adaptions affected care provision and the people involved. In some instances, it provoked huge shifts, both practically and emotionally, whilst other respondents recounted experiences of a healthcare system that was able to carry on practically as usual.
Discussion
Study results in relation to previous research
In this study, contact nurses from across Sweden have given their views on how cancer care was affected by the COVID-19 pandemic. Contact nurses can provide a unique and important perspective, as they are in close contact with patients and significant others and they coordinate with all team members in the multi-professional team involved in patient care. Our findings indicate that the prerequisites to provide care were altered by the pandemic in various ways; not least regarding how patients and healthcare providers interact, and in care accessibility. Contact nurses also report having been personally affected by the strains of the pandemic. Our findings are aligned with those of Krok-Shoen et al.'s study, 18 which identified the following barriers for providing care during the pandemic: organizational challenges, decreased patient access to resources and support, patients’ mental health, telehealth challenges, and patients’ physical status. When asking care providers about their personal experiences of care provision during the pandemic, the responses were similar to the findings of this study. Similarly, Jørgensen et al. 19 investigated nurses’ experiences of work at non-COVID-19 units and reflect on the difficulties in navigating the need for both closeness to and distance from patients during this time; a challenge addressed in this study as well.
Altered means of interaction
Respondents report a radical shift in the ways in which they had contact with patients and significant others. They described phone consultation as the most common mode of communication. Darcourt et al. 20 analyzed the implementation of telehealth visits for cancer patients during COVID-19 and found that, overall, it worked well. In agreement with the results of this study, Darcourt et al. 20 described an increased number of phone meetings, with some providers worried about the risk of missing significant clinical findings and inadequate patient interaction. Video and phone meetings will likely remain an important mode of communication after the pandemic, and it is important to distinguish when and with whom this is of most benefit and when a physical meeting is preferrable. As suggested by Drury et al., 21 telephone contact and telemedicine may not adequately address the complexity in supportive needs for people affected by cancer when implemented as rapidly as these services sometimes were during the pandemic.
Although not being a principal question of investigation of this study, we note that very few respondents report using digital tools to communicate with patients, whilst phone calls seem to have been very common. Contradictory to this finding, other sources describe the pandemic as a digital accelerator, explaining that a big leap in the digitalization of the Swedish public sector has been made, not least when it comes to telehealth and video meetings.22,23 Our data concern a relatively early phase of the pandemic – the spring and summer of 2020. It is possible that the implementation of telehealth methods has increased since then, but our data suggest that, at least during that time period, the respondents did not seem to have taken the described digital leap, which prompts further investigation, not least because oncology nurses have reported that the use of video conferencing enhances accessibility and quality of care for home-living patients. 24
Altered interaction with significant others and altered support needs
Person-centered care, a prominent aim in Swedish healthcare, 25 is described as ‘an approach to practice established through the formation and fostering of healthful relationships between … service users and others significant to them in their lives’. 26 (p.3) Giusti et al. 27 highlight that person-centered care must value the social network of each patient, especially in the case of serious illness. Significant others are thus identified as potential resources, receivers of care, and team members who surround the person affected by cancer. In this study, a tripartite role of significant others was found in the attestations from the contact nurses: they were supporters of the cancer patient, they were partners of the care providers, and they were subjects affected by the cancer diagnosis of a loved one. All these roles were greatly affected by new rules and guidelines resulting from the pandemic.
In the endeavor to decrease the spread of disease and to protect vulnerable patients, the decision to exclude significant others from physical visits seems straightforward, but it is worth noting the ripple effects this might cause. If their input and needs are not identified at the same time as those of the patients, their need for support might increase due to isolation and stress, and thus the wellbeing of both patients and significant others could be affected in the short and long term. Simultaneously, care providers experienced having less access to a potential ally or team member.
Whilst patients in Sweden have extensive formal rights to support, 28 the rights of significant others are more complex. 29 Even if there seem to be consensus that significant others can be a valuable resource that should be acknowledged, that notion is not translated into formal rights (children under 18 years of age are exempt). Previous research shows that partners of people diagnosed with cancer are at higher risk of developing different kinds of illness.30,31 We hypothesize that the situation described here might increase those risks further.
We have, to date, not been able to identify other studies covering the perspective of significant others in the cancer pandemic context, which is an addition to existing knowledge that we warmly welcome.
The pandemic – a stress test for health equity
A key finding is that contact nurses’ perceptions of whether and how cancer care was affected by the pandemic vary significantly. Some respondents reported no changes, whilst others identified various degrees of negative effects on care provision. About half of the respondents in this study reported that they were not able, or were only partly able, to carry out their assignments as contact nurses after the pandemic hit, and that their ability to provide psychosocial support decreased. Even before the onset of the pandemic, there were significant differences regarding the degree to which contact nurses could carry out their role in different settings, 5 which was in fact the stimulus for the QOPCoN study. This finding is important to discuss in relation to health equity, 32 a political goal in Swedish healthcare. 33
The Swedish political model, where 21 regions have a comprehensive mandate to adjust supply after regional needs and prerequisites, is frequently discussed from an equity point of view. The National Board of Health and Welfare published guidelines for prioritizations during COVID-19, 34 but it was deemed a regional and local issue to make the prioritizations based on specific conditions. 35 Our outlook is national, and we do not provide data that can shed light on whether variations can be grouped by region or diagnosis group. The pandemic has turned out to be an interesting ‘stress test’ of how structures thought to support equity work in a strained situation. Could it be that the pandemic has caused an increase in inequities by forcing regions and hospitals with different prerequisites to make their own priorities and assessments of how best to deal with the crisis?
Perhaps the pandemic has merely highlighted and exacerbated already existing differences between regions, or perhaps it has been responsible for creating new ones. This warrants further investigation.
If limited to the tumultuous time of the pandemic, some differences are likely unavoidable and, to a degree, understandable. We fear that, as the acute phase of the pandemic subsides, acute solutions become permanent solutions. In the specific context of the contact nursing function, this could mean that the role is hollowed and notched at the edges, as it is not an essential role, in the coarsest meaning of the word. Considering the beneficial effects seen when implemented properly, it is of great importance that the contact nursing role is protected and continues to be implemented broadly and thoroughly, in accordance with the national cancer strategy to support the endeavor towards person-centered care. It will be central to thoroughly evaluate and remediate the alterations that negatively affect equity in care post pandemic. The pandemic also provides opportunities to reconsider some established truths regarding cancer care provision – if well harnessed, the lessons learned from this crisis can instead improve cancer care.
Strengths and limitations
Survey, sample and data collection
A limitation of this study is that the survey questions regarding the pandemic were validated only by a judgment of face validity in discussion between authors. However, the questions are coherent with the aim of the original questionnaire (i.e. organizational prerequisites).
The fact that there are no formal qualifications for or register of contact nurses in Sweden makes a national survey such as this somewhat problematic in terms of reach. We had to rely on help from devoted co-workers at the regional cancer centers to gain permission to send the electronic survey to the line managers of identified clinics. Lists of possible respondents were difficult to keep updated, and sometimes the link was not passed on as expected. Moreover, there were clinics and an entire region that refused to let their contact nurses participate.
Convenience sampling strategies carry inherent weaknesses regarding representativity, as respondents may differ in unknown but essential ways from the total population. 36 Our method of data collection also carries with it a risk of bias, as participation may be dependent on personal relationships. We were not able to monitor the distribution of the electronic survey in detail and are thus not able to report an exact response rate. Considering the estimated number of contact nurses in Sweden (1500–1800), the number of respondents can be considered small. Still, taking the issues described above into account, the data set consists of a large number of respondents (n = 337 closed questions, n = 232 open-ended questions), from a variety of Swedish regions, working with different patient groups, and in both smaller and larger hospital settings (see Table 2).
Data analysis and results
A survey does not inspire respondents to provide elaborate, rich answers, in the same way as, for example, a qualitative interview would. Whilst many respondents shared their experiences by using generous wording, some answers to the open-ended question were short or even single-worded, which affected the possibility to interpret the data in a qualitative manner. This could be an argument in favor of choosing a different methodological approach. Utilizing qualitative content analysis, as we did in this study, means departing from some principles of the method in the data collection phase; it is not possible to ask participants to elaborate or ask follow-up questions, and there is no way of identifying when saturation is achieved. However, this approach was deemed suitable, as the free-text accounts required in-depth analysis to be understood in a comprehensive way, and, as of the initiation of the data analysis phase, the method can be applied properly. As we were investigating one specific question and had a large group of respondents, this methodological approach was considered to be as valuable as having performed in-depth interviews with fewer respondents. Further, a similar methodological approach has been successfully used in previously published research,16,17 and is, if handled appropriately, seen as a valuable addition to complement a survey.
Implications for the contact nursing role and further research
The extraordinary situation posed by the pandemic has shed light on vulnerabilities regarding the contact nurse role, indicating a need for further investigation and reflection. Specifically, the important role and needs of significant others would benefit from further scrutiny in relation to the contact nursing assignment, a question that will be further investigated in the larger QOPCoN project. Continuous evaluation and improvement of the contact nurse role and function is essential to meet the needs of people with cancer and in the push towards equity in health.
Even if the role of the contact nurse is specific to Swedish conditions, it bears resemblance and thereby importance to other similar roles held by nurses in cancer care in other settings.6,7,10 This makes the results also valuable for cancer care providers internationally, and for other nursing specialties affected by COVID-19.
Conclusion
Contact nurses report that the COVID-19 pandemic has affected their prerequisites of work, their patients, and significant others in various ways, not least when it comes to means of interaction and accessibility. These findings are important to deliberate as cancer care transitions into a post-pandemic phase, in order to avoid sustaining the short-term solutions put in place to cope with the acute situation, and instead make use of the lessons learned from this pandemic in relation to the contact nurse function.
Future studies would benefit from considering the perspective of patients and significant others directly, rather than these being filtered through the lens of the contact nurses.
Footnotes
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Author contributions
Ellen Brynskog: conceptualization, methodology, investigation, data curation, validation, visualization, writing – original draft. Maria Larsson: conceptualization, methodology, funding acquisition, investigation, resources, data curation, validation, visualization, project administration, writing – review & editing. Kaisa Bjuresäter: conceptualization, methodology, funding acquisition, investigation, resources, data curation, validation, visualization, project administration, writing – review & editing. Linn Rosell: conceptualization, methodology, funding acquisition, investigation, resources, data curation, validation, visualization, project administration, writing – review & editing. Frida Smith: conceptualization, methodology, funding acquisition, investigation, resources, data curation, validation, visualization, project administration, writing – original draft, review & editing, supervision.
Acknowledgements
The authors wish to express their sincere thanks to participating contact nurses in cancer care.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The work was supported by Regional cancer centre West.