
Abstract
Child-centered care is based on the fact that children are individuals with their own rights. Since January 2020, The United Nations Convention on the Rights of the Child (CRC) is law in Sweden. Children's meeting with professionals is important because it becomes the children's impression of healthcare that may reflect the children's future image of and feelings about the whole healthcare system. This prospective cross-sectional study aimed to explore child healthcare competence among nurses within primary healthcare. Data were collected through a web-based questionnaire among 101 primary healthcare district nurses, specialist nurses, and registered nurses. The study was compliant with the STROBE checklist. The results showed that the nurses have a good ability to apply child-centered care during children's visits to primary healthcare. To further implement a child-centered approach in primary healthcare, nurses need to have access to workplace educational opportunities continually, to enhance their child competence throughout their nursing careers.
Keywords
Introduction
Child-centered care is based on the fact that children are individuals with rights of their own. 1 Since January 2020, the United Nations Convention on the Rights of the Child (CRC) 2 is the law in Sweden. 3 The CRC recognizes children's (0–18 years old) rights to protection, meaning that children's needs should be in focus and their right to integrity and dignity must be respected in healthcare situations. The Swedish Patient Act 4 states that children have the right to receive information about their care and that such information should be adapted to the specific child. According to the CRC, 2 children's best interests should always be prioritized, including the right to participate in issues concerning and affecting their lives. Furthermore, Article 12 of the CRC 2 highlights children's right to express their opinion and have it respected.
Children understand, perceive, and interpret reality differently from adults, which is important to consider in care and treatment. 5 According to Harder et al., 6 it is the healthcare professionals and parents together with the unique child and situation that determine how children can participate in healthcare situations (e.g. in checkups and procedures). Research shows that children of all ages want to participate dynamically in healthcare situations, even though they require and have a desire for support.7–9 To promote meetings that are perceived as satisfactory by the child within healthcare situations, professionals need to have child healthcare competence, which means that they have to possess knowledge of children's development and how children of different ages perceive varied situations. Child healthcare competence also means that professionals should be able to understand children's signals and to meet their needs in order to strengthen security. Professionals who possess child healthcare competence can support children and increase their well-being.10–12 If professionals lack child healthcare competence, children may experience healthcare situations negatively, which in turn could cause visits within care environments to be perceived as daunting or intimidating. When children are restricted during a clinical procedure and not involved in healthcare, parents may feel guilty about being participants in inflicting hurt on their child and may regret their actions. 13 Furthermore, healthcare professionals may also experience their behavior as harmful and abusive of the child. 14
Professionals working in primary healthcare encounter persons of all ages and with a wide variety of health problems and are often a person's initial contact with the healthcare system. Swedish primary healthcare can be public or private. Nurses working in primary healthcare in Sweden are registered nurses with a bachelor’s degree and specialist nurses with a second-cycle level of higher education, including a master’s degree, often with the orientation as district nurse (75 credits) or other orientations such as, for example, care for older persons (60 credits), similar to nursing standards in several other counties. Specialist nurse education places emphasis on critical thinking and working in an evidence-based way, as well as on ethics, in both theoretical and practical aspects, 15 which can enhance professionalism when personal confidence increases. 16 A completed specialist nurse education acts as a resource in daily work. Professionals, within primary healthcare often come into contact with sick children, children with rashes or pain in their ears for example.
However, research about professionals’ skills in caring for children using a child-centered approach needs to be conducted. 1 A child-centered approach in healthcare situations requires recognition and a focus on the children's agency and rights and respect for children's voices, as well as experiences and participation.17,18 Shier's 19 model for improving children's participation in caring situations contains five levels of participation: at the first level, children are listened to, and at the fifth level, children have their own responsibility for decision-making. Furthermore, Shier 19 also describes three stages of commitment: opening, opportunities, and obligations. Each stage describes the prerequisites for working in a child-centered manner. During the opening stage, the professionals make a personal commitment to work using a child-centered approach, while at the opportunities stage, professionals have skills and knowledge as well as time to work using a child-centered approach. In the obligations stage, the organization follows a child-centered work policy. 19 When nurses and specialist nurses within primary healthcare apply the CRC and follow a child-centered approach, care can be characterized as child-centered. 20 According to Harder et al., 6 the challenges professionals face when having to take the child's perspective into account are related to attentiveness, understanding, time frame, imagination, and determination to meet the unique child in his/her state of being. In healthcare encounters it is necessary to ensure children and their parents are well-informed and prepared, by scheduling enough time for the encounter. 11 Research discloses that aspects such as color on walls and furniture affect children's well-being. 21 One way to make an environment child friendly is to use colors such as blue and green, which children prefer. 22 A child's meeting with professionals is important, as it becomes the child's impression of healthcare, which may, in turn, influence the child's future image of and feelings about the entire healthcare system. According to the Ombudsman for Children in Sweden, 23 children often experience deficiencies in responsiveness, information, and dialogue with professionals within primary healthcare, which may, in turn, lead to interruptions of intervention or care for the children. Furthermore, research is needed on regional and national infrastructures in pediatric care, 24 and little is known about the skills of professionals in primary healthcare in terms of respecting the child's opinion and facilitating active participation. For these reasons, research is needed on child healthcare competence and the approach that professionals within primary healthcare adopt in care meetings with children.
Aim
This study aimed to explore child healthcare competence among nurses within primary healthcare.
Method
The present study had a prospective, cross-sectional, descriptive design and focused on the child healthcare competence of district nurses, specialist nurses, and registered nurses within primary healthcare. This study was compliant with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist. 25
Questionnaire
To gain an understanding of the child healthcare competence of district nurses, specialist nurses, and registered nurses, a face validity questionnaire was created including questions inspired by the CRC and Shier's model, 19 since there is no standardized questionnaire on understanding the child healthcare competence within primary healthcare. The questionnaire included general questions regarding level of education, working experience in a primary healthcare setting (2–5 years, 6–10 years or > 10 years), and whether the nurses had a public or private primary healthcare employer. The questionnaire also included 19 questions about the participants’ experiences of working with children in primary healthcare (i.e. specific working environments adjusted to children; how district nurses, specialist nurses, and registered nurses approach and give information to children and/or their parents in primary healthcare; and knowledge about the CRC). Several questions were assessed using a five-point Likert-type scale ranging from 1 = ‘no knowledge’ to 5 = ‘much knowledge’. Other questions were to be answered as ‘yes’ or ‘no’. The questions were grouped into organizational aspects, pedagogical and social competence. 26 The content in the organizational aspects group involved how knowledge and experience are utilized, how time is planned and questions on the care environment design. Pedagogical competence sheds light on nurse education, how to provide information, how to prepare and carry out activities and procedures in order to create security and participation, and where the child has continued confidence for healthcare. Social competence illuminates attitudes in meetings with children and their parent(s).
The questionnaire also included four open-ended questions that enabled richer descriptions: ‘How do you encourage the child to be involved and express their opinion?’, ‘What do you do if you notice that the parents do not support their child?’ ‘Do you use any aids to inform the child about what is going to happen and if so which ones?’, and ‘What colors do you have on the walls in the waiting room and on work clothes?’ The questions were entered into a computer system called Education Survey Automation Suite (EvaSys), a web-based program to support data collection.
Setting and participants
Primary healthcare personnel from three different regions in the south, west, and east of Sweden were contacted by phone and asked to participate in the study. After written approval from the responsible head at both public and private primary healthcare centers, 135 email addresses were obtained for district nurses, specialist nurses, and registered nurses who met the inclusion criteria: to have at least two years’ experience working with children with illnesses in a primary care setting. Exclusion criteria was primary healthcare personnel working within child healthcare service.
Data collection
Data were collected between February and March 2019. The questionnaire was sent as a web link to the 135 nurses’ email addresses. Answers were to be entered directly into EvaSys. After a couple of weeks, only 45 answers were received. Therefore, a purposive sampling approach 27 was adopted, using bulletin board notices on healthcare professionals’ social media platforms, inducing 101 persons to answer the questionnaire.
Analysis
The data to be analyzed included 101 questionnaires. The data were automatically entered into IBM SPSS version 25, from EvaSys, and analyzed by means of the same program. Descriptive analyses for comparing differences in knowledge between district nurses, specialist nurses, and registered nurses in child healthcare competence were conducted using the Mann–Whitney U test and the chi-square test, respectively. Sub-analyses were conducted comparing differences in answers among registered and specialist nurses grouped together, to those of district nurses as their education includes a broader child healthcare perspective. In addition, differences were compared among participants with different working experiences as well as different employer organizations (i.e. public or private primary healthcare employers). The significance level was set at 0.05.
The open-ended questions were analyzed using a conventional qualitative content analysis according to Hsieh and Shannon. 28 Answers to the open-ended questions were read repeatedly by the authors (JH, CB and ML). Based on differences and similarities, the content was organized into themes through a back-and-forth process until agreement was reached among the authors. The themes are illustrated with quotations representative of the participants’ views. The analyses were conducted in Swedish and further translated into English in the final stage of the analyses.
Ethics
This study was designed, planned, and performed in accordance with Swedish law stating that ethical approval is not needed when healthcare professionals are invited for participation in questionnaires regarding work-related issues. 29 The participants were not considered as vulnerable, and their health was not considered negatively impacted by taking part of the questionnaire. Even though the study followed national ethical regulations, the Declaration of Helsinki 30 was followed, and the four ethical principles – respect for autonomy, beneficence, non-maleficence, and justice – were taken into account. The first page of the questionnaire included written information about the study aim, information that emphasized the study's confidentiality and the voluntary nature of participation, and the right to withdraw from the study at any time.
Findings
Among the 101 questionnaires returned, 60 (59.4%) were answered by district nurses, 12 (11.9%) by specialist nurses, and 29 (28.7%) by registered nurses , of whom 99 (98.0%) were women. In all, half of the participants had experience working in a primary healthcare setting for more than six years. One third of the participants worked in primary healthcare centers that were privately run and the others in publicly run centers. Among the district nurses, 38.3% had more than 10 years of working experience. Among the registered nurses, 42.9% had more than 10 years of working experience (Table 1).
Participants’ working conditions.

We have sorted items from the questionnaires and present the results section based on Shier's 19 description of the three stages of commitment in this way: the heading ‘Organizational aspects’ describes obligations, opportunities is addressed under the heading ‘Pedagogical competence’, and openings under the heading ‘Social competence’.
Organizational aspects
Organizational aspects revealed that the registered nurses had received less education in their workplace about children's development and how they perceive their surroundings, compared to participants who were district nurses and/or specialist nurses. Only 27.7% of the participants stated that children were given more time at scheduled appointments than they gave adults (Table 2). When comparing district nurses to other nurses, a statistically significant difference was found, indicating that district nurses more often stated that children were given more time at scheduled appointments than adults for similar conditions (p = 0.004) (Table 3). The majority of the primary healthcare centers had no separate waiting room for children or study rooms adapted for children. Few primary healthcare centers had guidelines on how care workers could promote a good care meeting with/for a child (Table 2). When comparing the answers of the district nurses to those of registered and specialist nurses, no significant differences were found in regard to organizational aspects.
Results from the questionnaire, stratified on profession and years in profession.
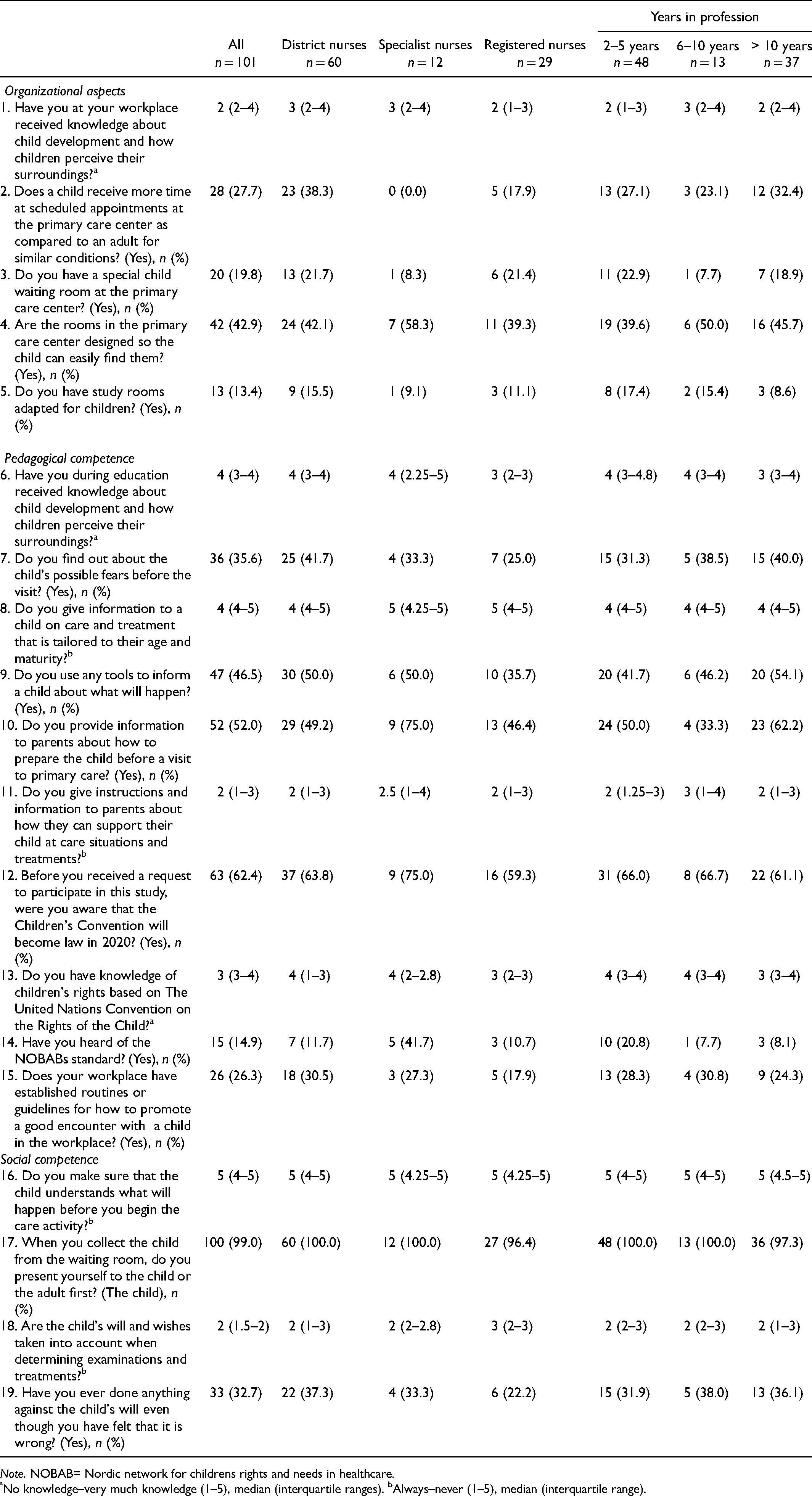
Note. NOBAB= Nordic network for childrens rights and needs in healthcare.
No knowledge–very much knowledge (1–5), median (interquartile ranges). bAlways–never (1–5), median (interquartile range).
Differences between district nurses vs. specialist and registered nurses, between private and public provider, and working experiences between district nurses vs. specialist and registered nurses.

See questions in full in Table 2.
Pedagogical competence
During telephone counseling and booking of appointments for primary healthcare, 52.0% of the participants stated that they informed the parents how to prepare their child for a care situation. Among the whole sample, 35.6% of the participants, when booking an appointment, examined the children's fears. Among district nurses, 41.7% (n = 60) asked children about their fears, as compared to registered nurses, of whom 25.0% (n = 28) asked about children's fears. The results revealed that the registered nurses had received less knowledge on children's development and how children perceive their surroundings in their basic education (Table 2). A statistically significant difference (p < 0.001) was found, which indicated that district nurses had received more education on how children perceive their surroundings compared to the other nurses (Table 3). However, all participants stated that they considered the child's age and maturity when providing information. Compared to district nurses and registered nurses, more specialist nurses (75.0%) were aware that the CRC would become a law in Sweden in 2020. Regarding knowledge of the CRC, registered nurses stated that they had less knowledge of children's rights (Table 2).
Social competence
The results showed that 99.0% of the participants tried to involve children during appointments and presented themselves to the child before they presented themselves to the parents. All participants also ensured that the children had understood what was going to happen before they started a care activity. More than a third of district nurses and specialist nurses, somewhat fewer among registered nurses, stated that they had done something against a child's will even though they had felt that it was wrong (Table 2). No statistical differences were observed when comparing the district nurses with the registered and specialist nurses in regard to social competence (Table 3).
Public versus private providers
Participants working in public primary healthcare answered to a higher extent that they had received knowledge on child development and on how children perceive their surroundings in their workplace (p = 0.035) (Table 3). Furthermore, participants working in public primary healthcare stated that children were given more time at scheduled appointments compared to participants working in private primary healthcare (p = 0.048). Publicly employed participants also stated that they make sure that the child understands what will happen before they begin a care activity (p = 0.018), compared to a greater extent participants working in private primary healthcare.
Working experience
Differences were found in answers between participants with more or less working experience. District nurses with more than six years of working experience perceived that they had received knowledge on child development and on how children perceive their surroundings in their workplace to a larger extent than the district nurses with less than six years of working experience (p = 0.016). They also used tools to inform a child about what would happen during a care situation more frequently than the district nurses with less than six years of working experience (p = 0.038). Specialist and registered nurses with less than six years of working experience answered that they had knowledge about children's rights based on the CRC more frequently than those with more than six years of working experience (p = 0.007). They also stated that they had examination rooms adapted for children to a higher extent (p = 0.045) compared to specialist and registered nurses with more than six years of working experience (Table 3).
Open-ended answers
Among the 101 participants, 93 answered the open-ended questions. Many answers were short, about a couple of sentences, ranging from one sentence to six sentences at the most. Conventional content analyses resulted in three themes: Focus on the child, Prepare the parents, and Child-friendly environment not a priority.
Focus on the child
In order to apply child healthcare competence, the participants emphasized the importance of focusing on the child and their needs. Having a child-centered approach was described as focusing on the child's needs in relation to age and situation. This could be done by getting on your knees and being on the same level as the child and listening to what the child has to say, according to the participants. Sometimes it was necessary to reschedule the time and prepare the child in a different way for the next visit: Sometimes I address the child directly, sometimes we simply have to cancel and they have to come back another time; for example, blood sampling procedures.
Several participants described the importance of planning the appointments at an appropriate time for the child, which could be when the child had eaten and/or was well rested. In order to increase children's feeling of security, children were encouraged to bring a pacifier or a teddy bear that the child perceived provided them with security. Prior to a planned care meeting, many participants advocated lidocaine/prilocaine cream as a preventive care action with the intent to decrease pain from blood sampling.
Prepare the parents.
The participants perceived that for the child to feel safe in a care situation, the participants had to prepare the parents to feel safe. This could be done by alternately listening to the adult and then to the child. The participants described how they sometimes had to ask the parents to try to be calm and instruct them on what to do for the sake of the child: The interaction with the child is most important, and it is important to involve the parent as well. Information! If it works with the child, it usually works with the parent as well.
When asked what advice the participants, regardless of profession, provided to parents before a care meeting, several participants recommended websites tailored for children, while others recommended films, books, and other sources of advice. Among the participants who provided other advice to the parents, the majority reported that they informed the parents what would happen at the primary healthcare appointment. Some participants responded that they used to send home pictures or brochures to be used as informative support, adapted for children before a care meeting. This was to make it possible for the child to prepare at home, together with the parent.
Child-friendly environment not a priority.
Participants reported that the environment at the primary care center was seldom adapted specifically for children. Few centers had special waiting rooms for children, but there was often a corner in the waiting room that was child-friendly with toys and books for children. According to the participants, the reason for not having a special waiting room for children was a lack of space, plus the participants did not experience a need for a special waiting room for children: We have a small area in the waiting room that is adapted for children, with toys, etc. But I think we never reflected on the fact that a separate room would be needed for them.
When asked about the color of their working clothes, the majority answered that they wore white trousers together with either a blue or gray blouse. Few participants described their working clothes as ‘colorful’. Waiting rooms were described as colored beige, white, light green, or gray. Few participants answered that they had pictures or patterns specifically intended for children on the walls of the primary healthcare centers.
Discussion
In this study, child healthcare competence among nurses within primary healthcare was explored. Based on Shier’s 19 model, child healthcare competence was divided into the following three different areas: organizational aspects, pedagogical aspects, and social competence.
Concerning organizational aspects, the results showed a potential for improvement, since merely one third of the participants gave more time for scheduled appointments to children than to adults. The length of an appointment is, according to Sahlberg et al., 11 important to take into consideration when planning for an appointment, because the child's ability to participate within the care is crucial for the child's feeling of being secure. The need for further improvements regarding organizational aspects was observed since several of the participants responded that they worked at primary healthcare centers that did not have separate play corners for children. Instead, play corners were integrated within the larger public waiting room at the different centers. In order for a primary healthcare center to promote children's rights, awareness of children's rights should be permeated throughout the whole organization in the way healthcare professionals plan appointments and care meetings, respond to children, and in the physical environment. 19 Therefore, nurses need to promote children's feelings of security both before, during, and after a care meeting.
In the current study, a majority believed that their employers did not provide them with enough education about children's development or children's rights under the CRC. 2 Healthcare professionals must be provided with opportunities to deepen their child healthcare competence, since such competence can support children and increase their well-being.10,12 For this to occur, employers need to take responsibility to give nurses the right guidance, time, and resources to provide care in line with the CRC. 2
Regarding pedagogical competence, there was also potential for improvement since only about half of the participants informed the parents about how to prepare their child for a scheduled appointment. According to Söderbäck, 31 it is essential to inform parents about examinations and treatments beforehand. Fear and/or uncertainty are recurring feelings among children,31,32 and nurses should be aware of the child's previous experiences with healthcare. 31 Several of the participants in the present study advocated cream with lidocaine/prilocaine as a preventive care action. Such treatment has previously been shown to be a successful method for reducing pain among children. 33 However, to be able to meet the needs of preventive treatment, it is vital that nurses are sensible of the fears and needs of the child. 31
The results revealed that the registered nurses lacked knowledge about children's rights regarding the CRC 2 to a greater extent than the district or specialist nurses. In Sweden, registered nurses and district nurses have different competence descriptions. Within the competence description for registered nurses, no specific requirement for skills to care for children is expressed, 34 while in-depth skills of normal development in children and adolescents are specified within the description for district nurses. 35 Shier 19 argued that knowledge is a prerequisite to work using a child-centered approach. Hence, since the CRC 2 is current law in Sweden, 3 children's needs should be in focus in care situations, and their right to integrity and dignity must be respected. The Swedish National Board of Health and Welfare states that every child and their parents have the right to be cared for by health professionals with competence within childcare. 36 It might be helpful if the future competence description for Swedish registered nurses were to include specific requirements for knowledge about children's care.
Some participants within this study gave instructions and information to the parents about how they could support their child during a care situation or treatment. From the qualitative answers, it was clear that several of the participants saw the planning of and preparation for appointments and care situations as necessary. The parents were, for example, told to bring a pacifier or a teddy bear that could provide the child with a feeling of security. Previously, it has been revealed that parents are valuable in supporting their children during care situations, 7 and their presence can facilitate reduced feelings of pain among children. 37 There are, however, situations when the rights of the child and the views of the parent separate. In such cases, nurses should attend to the needs of the child.1,20,37 To provide child-centered care, it is important to distinguish between a child perspective and the child's perspective. 31 This is because the first perspective (a child perspective) relates to the adults’ outside perspective with the individual child's best interests in mind. In contrast, the second perspective (the child's perspective) relates to the specific child's insider perspective. 38 Within family-centered care, the parents have the overall responsibility and make decisions on issues that concern the child. 17 This could, however, result in an underestimation of the needs and rights of children regarding the CRC. 1 Sometimes, parents may exclude children from participation, which may result in the child feeling that they are not allowed to express their own will 39 and in parents feeling regret afterward in situations, for example, when they have held their child during an examination or sampling. 13
Regarding social competence, all participants stated that they had ensured that the children had understood the given information correctly before a care activity was initiated. They also focused on the child in care meetings. Within Swedish law, it is stated that patients have the right to understand the information provided by healthcare providers. 4 This also applies to children as patients. Children want to participate actively in care situations8,9 and research has shown that interactive digital communication tools facilitate participation among young children in healthcare situations. 18 Many of the participants in this study were attentive to the child's will and wishes when conducting examinations and treatments. Shier 19 asserts that children need to be included within decision-making processes to reach a higher level of active participation. Our results show that not all nurses or specialist nurses had made a personal commitment to work according to a child-centered approach, which is the basic prerequisite. 19 However, in our study, about one third of the respondents had, at times, acted against the will of the child. Such cases could occur when a physical examination is considered necessary due to the medical condition of the child. Then, the participants thought that they acted in accordance with the child's best interests. Previous research shows that children experience anger or discomfort when physically held by adults during medical examinations or treatments. 40 Also, both parents 13 and professionals 14 report negative experiences from such situations. Sahlberg et al. 11 claim that children may be affected negatively when there is a lack of time or competence during healthcare encounters. Competence, strong leadership, and economic support are encouraged in order for children's rights to be implemented and permeated throughout organizations. Globally, the prerequisites for children's health differ, and the CRC stipulates the children's rights of having determinants for maintaining their health addressed. In their study, Goldhagen et al. 41 claim that the CRC and the principles of child rights could function as a structure for a child-rights-based approach. To be able to meet the CRC in their daily work, nurses are, however, in need of both knowledge and competence, as well as well-functioning organizational structures. Even though this study only represents three different regions, south, west, and east of Sweden, and no national comparison has been carried out, the current results shed light on which types of knowledge and competence need to be improved, and, therefore, the current results might be used as guidelines for leaders in their understanding of how to support nurses’ facilitated knowledge and competence in a global perspective.
Methodological considerations
The questions included within the questionnaire were carefully chosen and in line with the aim of the current study as well as previous research. The construction of the measures was inspired by Shier, 19 which was considered to strengthen face validity, although the questionnaire itself was not validated. To make it possible for the participants to express themselves freely, the questionnaire included open questions. The open questions were considered a study strength, since they made it possible to scrutinize the participants’ understanding of what was asked. Study limitations, however, included lack of information about the participants’ age, the specific length of work experience within primary care, or as nurses. Since the sampling strategy had to be extended by using social media platforms, we also lacked knowledge about the area and city of the workplace for half of the sample. Furthermore, we were not able to analyze the differences between respondents and non-respondents because we lacked information about non-respondents due to the sampling procedure. However, the questionnaire was web-based to enable a broader geographical distribution. In total, 101 nurses answered the questions in the questionnaire, which was considered a study strength, although in some cases this resulted in small groups for comparative analyses. When considering the results, it is important to bear in mind that the nurses who gave their consent to participate might possess a more in-depth understanding of or interest in childcare and children's perspectives. It might be the case that the nurses who declined participation had a lower understanding of or interest in childcare and children's perspective. Nevertheless, there was a relatively small internal dropout rate, which could be considered a study strength. In addition, the sample is considered to represent the different categories of nurses working within Swedish primary healthcare (i.e. registered nurses, district nurses and specialist nurses), and analyses have been carried out to explore child healthcare competence among the different categories of nurses. Furthermore, the finding that district and specialist nurses seem to have a somewhat wider child healthcare competence, compared to registered nurses, is not surprisingly because the specialist nurse education places emphasis on critical thinking and working in an evidence-based manner, as well as on ethics, in both theoretical and practical aspects, 15 which can enhance professionalism when personal confidence increases. 16 Besides, registered nurses and district nurses have different competence descriptions, as mentioned previously.
Conclusion
This study aimed to explore child healthcare competence among nurses within primary healthcare. The results reveal that nurses in primary healthcare, in this sample, have a good ability to apply childcare competence during children's visits. However, the results also showed some needs for improvement in regard to primary healthcare nurses’ child healthcare competence. It seems that specialist and registered nurses had less knowledge about children's rights regarding the CRC, children's development, and how they perceive their environment compared to district nurses. Therefore, the results suggest that there is room for improvement for nurses in primary healthcare regarding their child healthcare competence due to organizational aspects, but also due to pedagogical and social competence. In order to implement a child-centered approach in primary healthcare, nurses need to continually have access to workplace educational opportunities to be able to enhance their child healthcare competence throughout their nursing careers. It is part of nurses’ competence in primary healthcare to take responsibility for improving organizations and their own skills, but it is up to employers to give them that opportunity.
Footnotes
Author contributions
The first, third and fourth authors designed the study. The third and fourth authors were responsible for the data collection. The first, second and last authors were responsible for the analysis and drafted the manuscript. All authors approved the final version of the manuscript.
Acknowledgements
The authors would like to thank the participating nurses.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.