
Abstract
Involving patients, public and users in health education is currently receiving increased attention. The degree of involvement has changed over time, as have the methods used to involve these groups in nursing education. The purpose of this scoping review was to identify and map available didactic and pedagogical methods for patient, public and user involvement in academic nursing education. Of the initial 9294 articles identified, 21 were included. The PRISMA guideline for scoping reviews was used in the screening process. Data from the included studies were extracted and three thematic categories were identified: 1) Experts by experience, 2) Digital tools and 3) Curriculum planning and development. We identified 16 methods for patient, public and user involvement in nursing education. The findings provide an overview of these methods, which nursing educators may use.
Keywords
Introduction
Patient and public involvement and user involvement are recognised and internationally widespread focal points in modern research, healthcare and education.1–5 The importance of patient, public and user involvement is widely acknowledged, and policymakers and health research increasingly direct attention to this topic internationally.1,2 The terms used to describe patient, public and user involvement vary widely between studies.3,6,7 This inconsistency was identified by Langton et al., who described the use of interchangeable terms such as user involvement, consumer participation, lay participation or partnership and patient participation. 7 This inconsistency challenges investigation of the concept of involvement in health education. The Research Council, based in Australia, and INVOLVE, based in the United Kingdom, define involvement as making research or decisions with or by rather than to or for the relevant parties.1,3 Among other things, patient, public and user involvement ensures relevance and allows us to collect valuable knowledge ensuring that health solutions affect the healthcare system's users as intended.3,8 This is fully in line with the WHO's call for a change in the way healthcare is organised to ensure increasingly people-centred services. 9
Patient involvement in medical education has a relatively long history, as William Osler introduced educators to patient involvement more than 100 years ago. 4 The degree of involvement has changed over the years, as patients have shifted from playing a passive towards having an increasingly active role. The variable degree of citizen participation is captured in the ‘Ladder of Participation’; a concept developed in 1969 by Arnstein. 10 Similarly, Lathlean et al. described a spectrum of participation ranging from User as recipients to User-led initiatives. 11 Subsequently, a considerable body of literature has addressed different methods for, benefits of and barriers to implementing patient, public and user involvement in health education. Numerous reviews have been conducted focusing on involvement in health education, and various reviews have summarised involvement in medical education.12–15 For example, one study aimed to identify involvement in the planning, delivery and evaluation of education for health professionals, 16 and a review synthesised the literature broadly to explore involvement in health education over time. 4 Additionally, other studies have aimed to update the evidence on involvement in health education,17–20 and a recent scoping review conducted by Soon et al. set out to map the literature to determine how consumers are involved, recruited and retained in nursing, midwifery and related health professions. 21 These studies, however, did not provide information on or summarise the various didactic and pedagogical methods used to implement patient, public and user involvement in nursing education. In recent years, however, focus has shifted towards a broader perspective including various health educations.
The purpose of this scoping review was to seek more in-depth knowledge about the various didactic and pedagogical methods used to ensure patient, public and user involvement in academic nursing education.
Methods
This scoping review was conducted in the 2020–2021 period. Scoping reviews are beneficial for mapping research in situations in which it may be challenging to predict the amount of material in a research field.22–24 Generally, the approach affords an opportunity to summarise and disseminate the current evidence within an area to decision-makers and practitioners who may lack the resources to perform this task in their daily work.
This review was conducted in accordance with the PRISMA guidelines for scoping reviews 25 and the five stages identified by Peters et al., Levac et al. and Arksey and O’Malley.22–24 A detailed description of the procedure is provided in the following sections.
Stage 1: identifying the research question
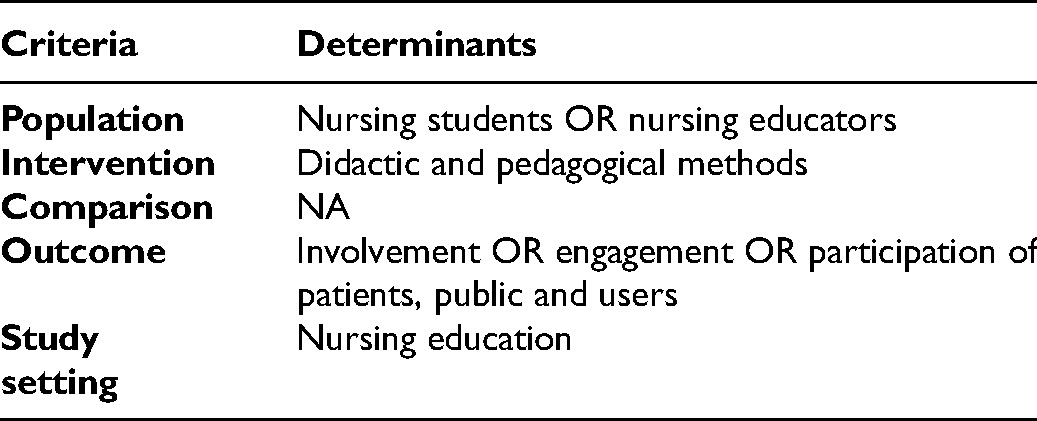
As recommended by Arksey and O’Malley,24 this review maintained a broad approach to ensure breadth of coverage. Subsequently, the search strategy was guided by PICOS to maintain focus on the research question present during the database searches and in the course of the screening process (see Table 1).
PICOS framework used to guide the literature search and study selection.
Stage 2: identifying relevant studies and literature search
A systematic search conducted in August 2020 and repeated in May 2021 covered the databases: CINAHL, ERIC, Education Research Complete and PubMed. Relevant keywords were identified and used as MeSH terms in PubMed and as CINAHL l headings in CINAHL l. Combinations of the identified search terms, both free terms and subject terms, were combined using the Boolean operators OR and AND (see Appendix 1 in the online supplemental material) . A broad search with several synonyms was used to avoid excluding any relevant articles. The search was adapted for each database and was validated by a medical librarian. Additionally, we reviewed reference lists from relevant studies and hand searched key journals. Grey literature and books were not included.
Stage 3: study selection
To eliminate irrelevant studies, we developed a number of inclusion and exclusion criteria. As recommended by Arksey and O’Malley, 24 the criteria were developed ad hoc as our familiarity with the literature increased. The inclusion criteria were: 1) research articles published in English, Danish, Swedish or Norwegian; 2) articles on patient and public involvement in professional healthcare training programmes. Excluded were articles in which the main objective was patient and public involvement in clinical healthcare settings, clinical placement, and also patient and public involvement in research settings and articles from developing countries. During the screening process, it became clear that including all healthcare professionals produced an overly extensive amount of literature. We therefore added the inclusion criteria regarding nursing education, thereby excluding studies focusing on other healthcare professions. Both authors participated in the screening process. In case of disagreement, a consensus was reached by discussions among the authors. The web-based software platform Covidence and the PRISMA for scoping reviews 25 were used in the screening process.
In total, 9294 studies were retrieved by systematic searching. Once duplicates had been removed, 8791 potentially relevant studies remained. Next, the titles of the records were screened thereby discarding an additional 8211 studies. Subsequently, the abstracts of the studies were screened, excluding an additional 548 studies. Additionally, upon full-text screening, an additional 13 studies were excluded. Finally, three studies were included through citation chaining, leaving 21 studies for inclusion in the scoping review.
For a detailed presentation of the study selection process adopted in this scoping review, please refer to the flow diagram in Figure 1. The diagram was adapted from Page et al. 26
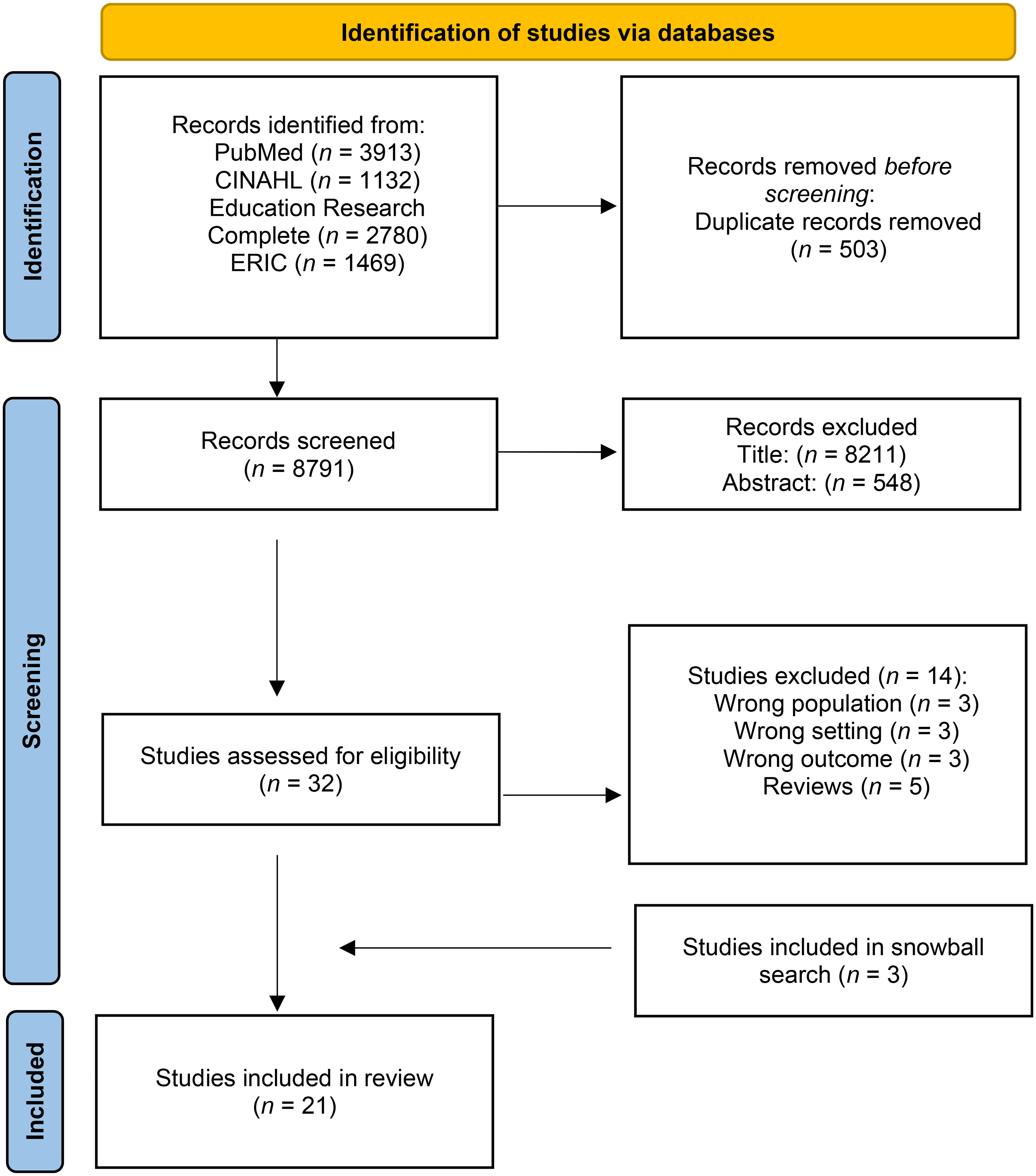
Flow diagram of the study selection process.
Stage 4: charting the data
The data extraction was based on a thematic construction across the studies. When a broad approach to a research question is adopted, Arksey and O’Malley 24 recommend that no synthesis should be made. Instead, data should be presented as themes that emerge from a thematic analysis. The results of this review are therefore based on an inductive thematic analysis inspired by Braun and Clarke. 27 First, all methods reported in the included studies were identified and extracted. This made it possible to identify patterns and themes across the entire data material. Given that the analyses were inductive, the reported methods were coded without making them fit into a predetermined framework. Next, the themes were mapped in relation to each other and Table 2 was developed. The headings in Table 2 are inspired by the Joanna Briggs Institute's recommendations and by Peters et al.22,28 and Arksey and O’Malley. 24 Due to the nature and objective of the scoping review, the quality of the included articles was not appraised.22,24,28 Subsequently, the themes were further described. The three themes that form the basis for the study results emerged in the course of this process.
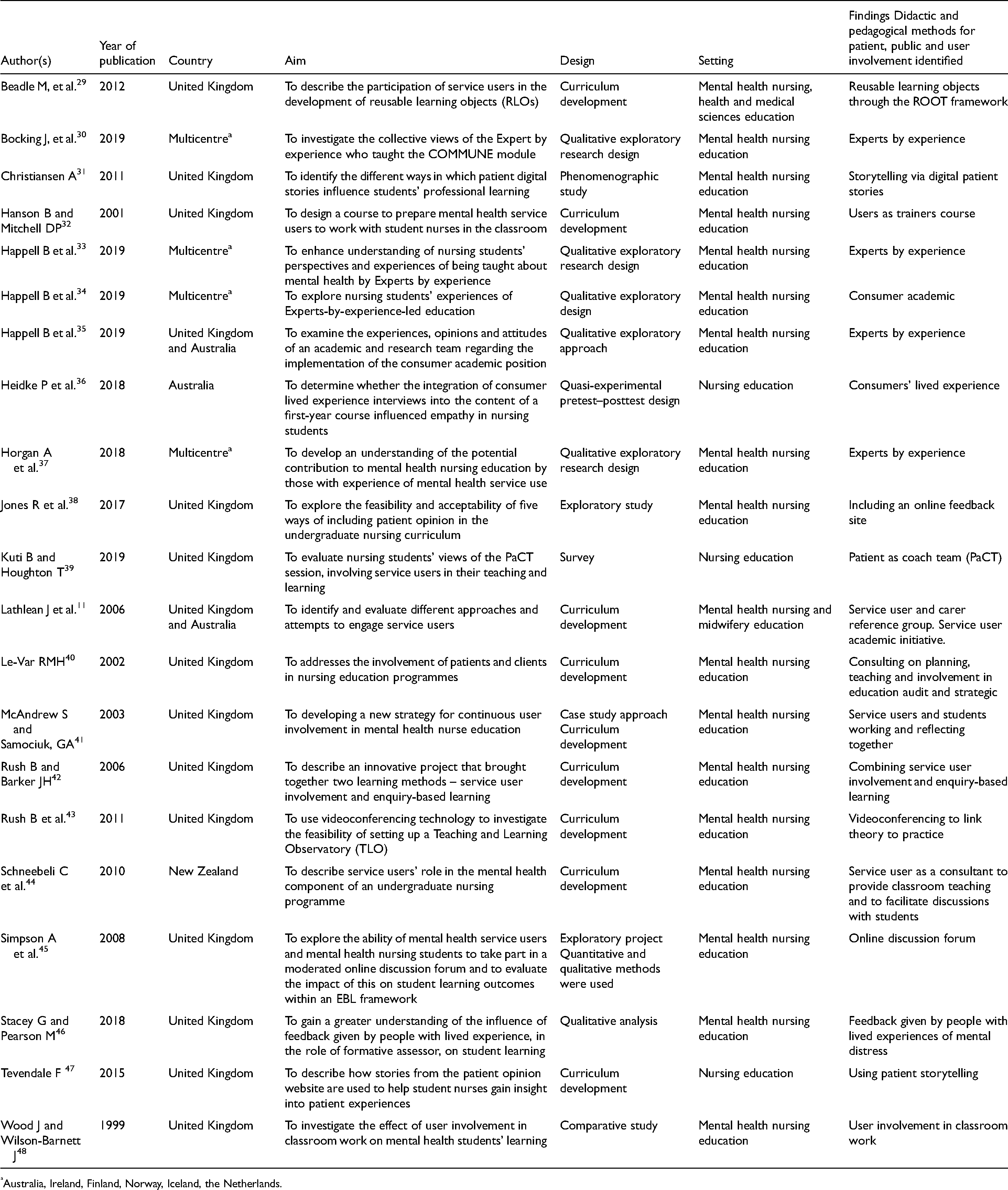
Overview of the included studies and the didactic and pedagogical methods identified.
Australia, Ireland, Finland, Norway, Iceland, the Netherlands.
Ethical considerations
According to the Danish National Committee on Health Research Ethics, 49 ethical approval was not required prior to the execution of this study. However, the Helsinki Declaration, 50 Guidelines for Nursing Research in the Nordic Region 51 and The Danish Code of Conduct for Research Integrity 52 recommend that researchers always include ethical considerations in their research. Inspired by Weingarten et al., 53 we assessed the included studies for ethical considerations.
Results
Stage 5: collating, summarising and reporting the results
The results are presented in two ways based on our thematic analysis. First, the included studies are described with respect to geography, year of publication and setting. Next, the three identified themes are elaborated. The studies were indexed by geography and publication year. This showed that the included studies were published between 1999 and 2019 (see Table 2). Most of the studies were conducted in the United Kingdom (n = 15). The rest of the studies were conducted in New Zealand (n = 1) 44 and Australia (n = 3)11,35,36 and four studies30,33,34,37 were multicentre studies conducted as collaborative efforts comprising researchers in Australia, Ireland, Finland, Norway, Iceland and the Netherlands. Most of the included studies (n = 18)11,29–35,38,40–46,48,54 were conducted within a mental health nursing education setting.
This scoping review identified 16 methods for patient, public and user involvement in nursing education. The studies were organised thematically according to the methods used (see Table 2). Furthermore, based on the included studies, findings were organised into three thematic categories: Experts by experience, Digital tools and Curriculum planning and development.
Experts by experience
This review identified 12 studies30,33,34,36,37,39,41,42,44,46–48 describing the use of service users representing different types of involvement within nursing education. The methods included classroom teaching, joint reflection, patient as coach team (PaCT), feedback and patients or service users talking about their experiences as a patient/user. In some studies, the term Expert by experience33,34 was used. In other studies, the following terms were used: patients, consumers, people with lived experiences,30,36,46 real-life experiences, 39 user involvement in the classroom 42 or patient storytelling. 47 Nine of the 12 studies identified in this category refer to or arise from mental health nursing education. Only three studies do not have this specific focus.36,39,47 Two studies32,40 briefly mention Experts by experience as a method, but included no further descriptions of how the method had been used in their studies.
The four articles by Horgan et al., 37 Happell et al.33,34 and Bocking et al. 30 are all based on the same study – The COMMUNE Project. These studies examined different elements of using Experts by experience within mental health nursing education.30,33,34,37 The study by Horgan et al. aimed to understand the potential contribution of those with experience of mental health service use to mental health nursing education. 37 The study by Bocking et al. aimed to investigate experts’ experiences when teaching in a mental health nursing programme. 30 Conversely, Happell et al. explored this issue from the students’ perspective, investigating how nursing students experienced being taught by people with lived experiences.33,34
In the study by Schneebeli et al., a method was used in which a service user was hired to contribute to classroom teaching. The study showed that the service user served to facilitate discussions with smaller groups of nursing students. 44 Likewise, Wood and Wilson-Barnett described a method to set up user involvement during classroom work. 48 Similarly, Rush and Barker described how they used mental health service users in an enquiry-based learning process with student nurses. The role of the mental health service users was to facilitate learning in the classroom before, during and after mental health placements. 42 Like Schneebeli et al., 44 Rush and Barker described how the service user worked with student groups, each counting 13 group members. The service user discussed with the students their lived experiences as a patient admitted to an acute ward. 42 The method described by Rush and Barker also included a follow-up in which students discussed their learning outcomes with a service user and a facilitator. 42
McAndrew and Samociuk described a method of joint reflection on mental health issues between service users and students. 41 In the course of ten sessions, students, educators and service users cooperated to establish a reflective learning room. Initially, they worked with group dynamics; thereafter, they devised a plan for the contents of the remaining sessions. 41 Kuti and Houghton presented a similar method. They named their method the patient as coach team (PaCT); a method based on the idea that student learning based on service users’ real-life experiences may generate critical learning for student nurses. Kuti and Houghton described how PaCT sessions were embedded into nursing education in which service users were invited to lead some workshop sessions. 39
Stacey and Pearson presented their work on feedback and academic assessment given by people with lived experiences who were entrusted with the role as formative assessors who provided feedback. 46 According to Stacey and Pearson, the method consists of an assessment in which the students are required to conduct an interview in a simulated scenario with an authentic experience of mental distress. An essential part of this method is that the interview is filmed, and that the student receives both verbal and written feedback from the person with lived experiences. 46
Heidke et al. used videotaped interviews to capture lived consumer experiences. 36 Likewise, Tevendale described the benefits of using patient storytelling in teaching and learning in the field of nurse education. 47 Several of the included studies employed more than one of the identified methods. This phenomenon was identified in Tevendale and in Heidke et al. who merged the method Experts by experience with various types of digital tools.
Digital tools
Six studies31,36,38,43,45,47 employed digital tools to involve patient, public and users in nursing education. They focused on different types of involvement facilitated by a range of digital tools such as storytelling via video or digital patient stories,31,36 online feedback sites,38,47 videoconferencing 43 and an online discussion forum. 45 The study by Simpson et al. showed how the students worked with online discussion forums using an innovation method. 45 Adopting an enquiry-based learning approach, the authors used a blended e-learning method to facilitate online interactions between mental health service users and preregistered mental health nursing students. This method established a platform for users to discuss their lived experiences regarding their care and treatment. These discussions encouraged nursing students to reflect on implications for their practice. Simpson et al. described this method as both feasible and highly desirable.
To reduce the gap between theory and practice, Rush et al. suggested using the method they named Clinical Practice Teaching and Learning Observatory (CP-TLO). With this method, nursing students first observe an experienced nurse via videoconferencing and subsequently hear the real experiences of service users; an approach that gives the patients a voice in nursing education. 43 Additionally, Jones et al. suggested a feasible way of embedding feedback sites into academic nursing education. They presented a method in which the students prepared for clinical placements using various options at an online feedback site, e.g. timetabled webinars, video lectures, Tweet chats, self-study and online focus groups. In this manner, the method made non-clinical engagement with patients and service users more feasible. 38 The study by Christiansen indicated that a narrative method using digital patient stories may be a beneficial way to learn. This method created an opportunity for nursing students to transcend their frame of reference and engage with the reality of others. Using digital patient stories may also transform the professional identity of nursing students. 31 Similarly, Heidke et al. used videotaped lived consumer experience interviews in a first-year course forming part of a nursing training programme. 36 Overall, these results suggest that digital tools may be sustainable didactic and pedagogical methods with which to promote patient, public and user involvement in nursing education.
Curriculum planning and development
Five studies11,29,32,35,40 addressed methods that included patient, public and user involvement in the planning and development of the nursing curriculum.
Beadle et al. described a framework (ROOT) that may be used to facilitate service users in their collaboration on the development of reusable learning objects. They describe a process in which service users work with narrative methods where they use their own experiences to construct a narrative. Subsequently, actors with learning disabilities are invited to add additional perspectives to the written story. Finally, the story is filmed and used as part of teaching. 29
As mentioned by Le-Var, service users may be involved in planning the curriculum through consultation in various ways, for example, by participating in forums with local organisations, by face-to-face consultation or by written consultations. 40 Le-Var described involvement at both a strategic and operational level by involving patients and relatives in audits and conferences.
Lathlean et al. presented three initiatives to promote the involvement of service users in mental health education. The initiatives are: 1) implementing a service user and carer reference group, 2) employing service users in academic positions, and 3) creating a cooperative inquiry. 11 Happell et al. also argued for the benefits and value of contributions from a consumer academic in mental health nursing education. 35 Furthermore, Hanson and Mitchell described a course design aiming to prepare mental service users for interacting with student nurses in the classroom. 32 In summary, these results identify a continuum of different methods for involving patients, public and users in the development of nursing education at the strategic level.
Discussion
The aim of this review was to explore methods for patient, public and user involvement in academic nursing education. The study identified and included 21 articles covering this topic. This review identified approximately 16 different methods for involving patients, public and users in academic nursing education. Three thematic categories were identified: Experts by experience, Digital tools and Curriculum planning and development. Patient and public involvement has changed in the past 20 years, and various meta-narratives interact and co-exist. 4 This is reflected in the present study where two thematic categories prevailed: Experts by experience and Curriculum planning and development.
Experts by experience
Experts by experience was identified as the current leading method for involving patients, public and users in nursing education. This is consistent with other research.21,55 Furthermore, a national survey by Happell et al. found that face-to-face teaching is one of the dominant activities used for involving consumers in nursing education in Australia. 55 Based on evidence-based practice, 56 the patient's preference is central to clinical decision-making. Although the method Experts by experience is the most common method identified in this review, it is essential to be aware that the patient represents expert knowledge of the patient's own lived experience. In a nursing professional context and in relationships between, e.g. a patient and a nurse, it is vital to insist on paying attention to identifying the individual's personal preferences concerning joint clinical decision-making. Furthermore, it should be noted that patients, citizens or users who have the resources to participate as ‘experts by experience’ may constitute a selected group holding more health competencies than others with the same disease or disorder. Therefore, a risk exists that the patient or citizen perspective that is presented as part of teaching may be different from the reality that a typical student will encounter in clinical practice. This may be a significant didactic consideration prior to applying this method.
Digital tools
Owing to the ongoing development within the field of digital learning, findings relating to methods using digital tools are expected in this review. These methods come with both opportunities and barriers. Previous research57,58 has shown significant differences between individuals’ ICT competencies/e-health literacy. These differences must also be assumed to apply in the context of patient, public and user involvement in nursing education. An important prerequisite for applying methods that are based on or which comprise the use of digital tools is that the necessary hardware and software are available to all parties involved.
Implementing new methods based on innovation, inquiry-based learning and blended e-learning requires that students are ready for change. Fundamentally, students need to be willing to participate in learning communities in new ways. Therefore, identifying the students’ learning prerequisites is an important didactic consideration in the application of these methods.
In addition, it is pivotal that the educator assesses whether the method considered supports the objective for the learning outcome. It is also crucial that the parties involved in the process are familiar with the user interface of the programs used. Otherwise, a risk exists that students may develop resistance to learning. The use of digital tools can, on the other hand, shorten distances, thereby facilitating the involvement, e.g. of vulnerable or immobile patients or in cases with large distances between clinical practice, patients and the education institution. In addition, online conferences and videos, e.g. may be beneficial in curriculum planning.
Curriculum planning and development
Several of the studies in this review indicated that a possible solution furthering involvement would be to employ patients, public and users as academic staff or consultants. However, funding such activities may be challenging within the training programmes’ budgets. Therefore, it may be a question of patients, public and users having to work voluntarily, or a matter of collaboration with an interest organisation that reimburses the patient. In that case, an inequality may arise with respect to which interest organisations are represented in any specific training programme, and a risk may exist that the largest patient groups or the largest interest organisations will be overrepresented/have more impact on curriculum planning and development. In addition, attention should be paid to the fact that political and strategic decisions and strategies impact the incentive for patients, public and users to be involved in nursing education. An increased political and societal demand for the involvement of patients, public and users may therefore serve to promote the use of the methods identified in this review.
Strengths and limitations
This study is aware of previous studies that have aimed to identify patient, public and user involvement in nursing education.20,21,59 However, these studies adopted a slightly different focus. The study by Soon et al. was not entirely focused on involving patients and the public, but rather on how consumers were involved, recruited and retained. 21 Similarly, Suikkala et al. concentrated on nursing students’ clinical training. 59 In contrast, this review aimed specifically to establish in-depth knowledge about various didactic and pedagogical methods to involve patients, public and users in academic nursing education. Concerning other studies within the area, the findings from the present study differ by having adopted narrower outcomes. The research question in this review was how we may derive in-depth knowledge about didactic and pedagogical methods for patient, public and user involvement in academic nursing education. Several other reviews have explored patient and public involvement more broadly. Thus, different types of evaluations and studies with descriptions of patient and nursing students’ experiences emerged from our literature search. These studies did not focus on specific didactic or pedagogical methods, and they were therefore excluded. When looking at nursing education in its entirety, i.e. both the theoretical and clinical realms, the clinical realm stands out as significant for the general education of nursing students as far as inclusion of patients and public involvement in nursing practice are concerned. Therefore, a proposal for future research may be to gather the evidence within patient and public involvement within both theoretical education and clinical education. This may be done, for example, by conducting an umbrella review.
Conclusions and implications for research and practice
Based on systematic literature searches, this scoping review identified and mapped 21 relevant studies that reported on a total of 16 didactic and pedagogical methods for involvement of patients, public and users in academic nursing education. Although the material varied with respect to methods, most studies represented the method dubbed Experts by experience. In addition, most studies were conducted within mental health nursing education.
Since this review aimed to identify methods within the academic realm of nursing education, results from this review cannot draw conclusions about whether similar methods are used in clinical education. Based on the design of this study, we were unable to draw conclusions on the degree of effect that each individual method may have on the level of involvement. It would be interesting to investigate this aspect in the future. Finally, this review demonstrated a need to develop patient, public and user involvement methods beyond mental health nursing education.
Teachers within both the theoretical and clinical realms of nursing education may, based on this review, gain insight into concrete methods, tools and techniques to improve the quality of their teaching/education practice. This review does not examine how educators and clinicians experience this changed practice, but it would be highly relevant for future research in this field to examine this perspective further.
Supplemental Material
sj-docx-1-njn-10.1177_20571585221085989 - Supplemental material for Methods for involvement of patients, public and users in academic nursing education: A scoping review
Supplemental material, sj-docx-1-njn-10.1177_20571585221085989 for Methods for involvement of patients, public and users in academic nursing education: A scoping review by Rebecca Bauer Tørring and Stinna Bibi Pedersen in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
The authors take this opportunity to express their gratitude to the research programme ‘Professional Development and Educational Research’ at University College of Northern Denmark for their support.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.