
Abstract
It is a challenge to ensure high-quality palliative care. The aim was to investigate the perceptions of health care professionals (HCPs) working in a combined acute oncology-palliative care unit regarding the quality of the palliative care received by the patients and how important the care was to the patients. A Swedish total-survey cross-sectional study including 41 HCPs (54% response rate) was conducted with the 52 items Quality from the Patient’s Perspective – Palliative Care instrument, answered in two different ways: as actual care received and subjective importance. The STROBE-checklist was used. The areas for improvements were related to symptom relief, spiritual and existential needs, information, patient participation, continuity of care, care planning, cooperation and coordination of care, as subjective importance scores were higher than corresponding scores for care received (p ≤ .025). Providing high-quality palliative care alongside curative treatments for cancer patients is known to be challenging and could explain the results in this study. Implementation of a person-centred palliative care model based on the hospice philosophy could be a solution.
Keywords
Background
A major challenge for healthcare services globally, today and in the future, is to ensure high-quality palliative care for the increasing number of patients living with complex symptoms and needs at the end of life as a result of advanced cancer and its treatment.1–4 Patients and their families should be confident that when facing a life-threatening illness and in need of palliative and end-of-life care they will receive high-quality care, focused on providing comfort and dignity according to their needs and preferences. Modern palliative care aims to relieve suffering and promote wellbeing and quality of life for patients and their families through early identification, thorough assessment and treatment of physical, psychosocial and spiritual symptoms and problems.5,6 Through the focused holistic, individualized, family and team view of care, palliative care incorporates principles of person-centred care, and supports patients and their families to live a meaningful life, which has been shown to be crucial for achieving quality palliative care.7–10 This approach involves the patient as the centre of care, emphasizing a multi-professional team approach, and healthcare professionals (HCPs) being respectful and responsive to patients’ and their families’ life situation, preferences, needs and values.4,11,12
Hospice and specialized palliative care units, in which palliative care is performed exclusively, are often referred to as the gold standard for palliative care. However, the majority of palliative and end-of-life care in Sweden and Europe is provided outside these settings and is often instead carried out at general wards in hospitals.13,14 This means that palliative care is often performed alongside curative treatments. Concurrently caring for patients with different goals of care represents a challenge for HCPs.15–17 However, studies evaluating quality palliative care in acute or combined care settings are scarce. In addition, several areas for improvement have been identified across settings regarding fundamental cornerstones for palliative care, such as symptom control, communication and shared decision making.18–22 Consequently, the need to continuously evaluate palliative care to guide improvements and promote care quality is evident.3,23–26
Quality of care is multi-dimensional and complex, comprising diverse levels and perspectives. 26 In this study, the quality of palliative care is assessed using an instrument based on the theoretical model Quality from the Patient’s Perspective (QPP) developed by Wilde et al.,26,27 which has been adapted to be used from different perspectives and contexts. In line with the person-centred and palliative care philosophy, development and improvement of palliative care ought to be based on patients’ and their families’ perspectives. 10 However, since actions and abilities of HCPs have an impact on quality of care, 28 it is essential to also investigate the care phenomena from their perspective. It is also well known that the experience of providing high-quality care is related to high job satisfaction among HCPs, as well as an overall higher quality of care.29,30 However, it should be kept in mind that HCPs have been shown to assess palliative care quality differently compared with patients. Sofaer and Firminger 31 conclude that nurses tend to overestimate the importance of trust, empathy and competence, and underestimate the importance of nursing skills, provision of equipment and access to care. Physicians seem to underestimate the importance of information and provision of care, while they overestimate performance with regard to availability and waiting times. Other studies using the QPP instrument to assess care quality show that HCPs tend to underestimate actual care received and overestimate how important different aspects of care are, compared with patients’ perceptions.32,33 Nevertheless, examining HCPs’ perceptions of care provided, and how important they perceive the care to be for patients, allows important knowledge for improvement and development of palliative care to be obtained without burdening fragile patients and their families. This study aimed to investigate perceptions of HCPs working in a combined acute oncology-palliative care unit regarding quality of palliative care received by the patients and how important the care was to the patients.
Method and design
The present study was conducted as a total survey with a cross-sectional design. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cross-sectional studies was used. 34
Setting
This study was conducted in a combined acute oncology-palliative care unit at a county council hospital in Sweden, consisting of a ward and three specialist palliative home care teams. The ward had 20 beds, of which 12 were allocated for acute oncology patients and eight for palliative patients. The teams mostly cared for patients in palliative phases but also patients receiving curative treatments. The service by the specialist palliative home care teams included access to support by the teams during daytime and to the ward during evenings, nights and weekends.
Participants
All eligible HCPs (n = 76) comprising medical doctors (MDs), registered nurses (RNs) and healthcare assistants (HCAs), were invited to participate. The HCPs working on the ward rotated between acute oncology and palliative care, thus caring alternately for patients receiving curative treatments and patients at the end of life. The specialist palliative home care team included three to nine RNs and one to two MDs each. One RN worked both at the ward and in the palliative home care teams. All HCAs worked at the ward.
Data collection
Data were collected during two weeks in February 2018. The HCPs were given verbal information about the study at professional meetings at the care unit by two of the authors (EE and MR). Thereafter the questionnaires were distributed to all HCPs’ post boxes at the care unit, together with written information about the study. Completed questionnaires were returned in an envelope in a locked post box or by ordinary mail. A reminder was sent via email after one week.
Instrument
Quality from the Patient’s Perspective (QPP) is an instrument developed to measure the quality of care from the patients’ perspectives. 26,35 A modified version of the QPP instrument has been developed for advanced home care and palliative home care services.10,25 Sandsdalen et al. 10 further developed the instrument to fit various palliative care contexts, and has psychometrically evaluated the instrument version specific to Palliative Care (QPP-PC). The 52-item QPP-PC instrument comprises four dimensions of care quality – ‘Medical-technical competence of the caregiver’ (MT) (two factors and ten items), ‘Physical-technical conditions of the care organization’ (PT) (one factor and three items), ‘Identity-oriented approach’ (ID) (four factors and 20 items), and ‘Socio-cultural atmosphere’ (SC) (five factors and 16 items) – as well as three single items: medical care, personal hygiene, and atmosphere. In addition, the instrument includes two open-ended items (not used in this study).
The adaptation to the professional version comprises: changes to the wording to measure the HCPs’ perceptions of the care patients received, and the response alternatives to ‘yes’ or ‘no’ for three items in the ID dimension; information about responsible physician and RN, respectively; and patients’ opportunity to participate in an individual care plan. The results of these three items are presented in the text. Each of the 52 items of the QPP-PC was answered in two ways: how the HCP perceived the quality of care received by the patients (perceived reality, PR scale), and how the HCP perceived the importance of each aspect of care to the patients (subjective importance, SI scale). The PR of the quality of care was measured by items related to the sentence: ‘This is what I perceive that patients experience …’ (e.g. the best possible help for their pain). The items measuring the SI of care aspects were related to the sentence: ‘This is how important I perceive this to be for the patients …’ (e.g. the best possible help for their pain). A four-point Likert-type scale, ranging from 1 (do not agree at all) to 4 (fully agree), was used for the PR. For SI scales, the scale ranged from 1 (of little or no importance) to 4 (of the very highest importance). A not-applicable response was available for both scales. For the QPP-PC dimensions and factors, a mean value was calculated based on the individual participant’s response to the items in the respective dimension or factor.
Data on HCPs’ characteristics comprised age, gender, profession, academic degree, specialized education relevant for palliative care, employment, and work experience in healthcare, and in palliative care (eight items).
Statistical analysis
To analyse the data, IBM SPSS Statistics Data Editor Software, version 25, was used. Healthcare professionals’ characteristics and perceptions of palliative care (PR and SI) were examined using descriptive statistics. The Wilcoxon signed-rank test was used to explore differences in HCPs’ perceptions of care quality regarding the PR and SI scales. To avoid type 1 error, the statistical significance level for all the analyses was reduced to p < .025. Cronbach’s α was performed for the QPP-PC at dimension and factor levels of both subscales (PR and SI), and values > .7 were regarded as desirable (Table 1). 36
Internal consistency of the QPP-PC HCP instrument for dimensions and factors.
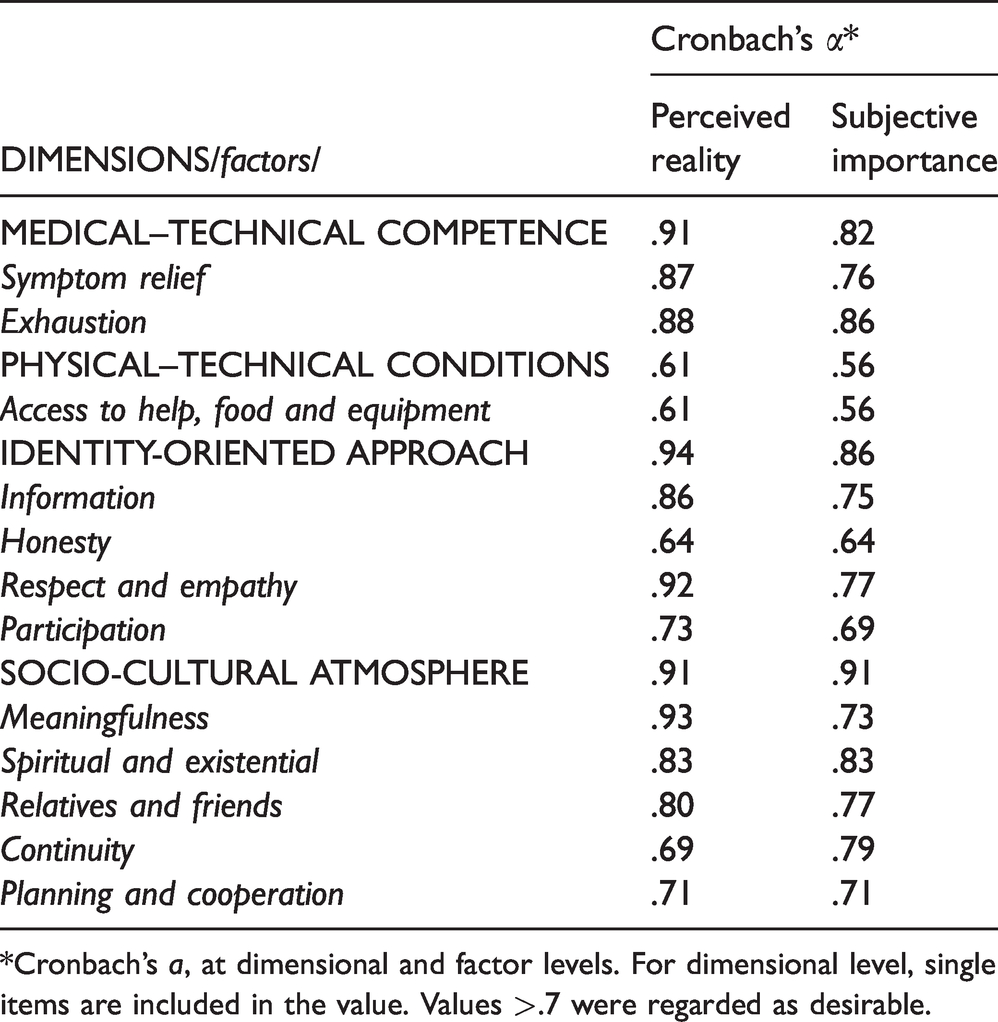
*Cronbach’s a, at dimensional and factor levels. For dimensional level, single items are included in the value. Values >.7 were regarded as desirable.
Ethical considerations and approval
The study was carried out in accordance with ethical principles and guidelines. 37 The study was approved by the Research Ethics Committee at Karlstad University (DNR No. C2018/131). The head administrator of the ward and the specialist palliative home care teams gave management approval for the study to be conducted. The head administrators, leaders and HCPs were informed verbally and in writing about the study, that participation was voluntary, and that the results were to be published. Completed and returned questionnaires implied consent to participate.
Results
Of the eligible and invited 76 HCPs in the ward and in palliative home care teams, 41 returned the questionnaire (response rate (RR) 54%), divided between RNs (n = 28, RR 60%), HCAs (n = 6, RR 54%) and MDs (n = 7, RR 36%). Place of work was for responding RNs: ward (n = 14), home care teams (n = 13) and rotation between ward and home care team (n = 1). All HCAs worked at the ward and all MDs were responsible for all patients irrespective of place of care. Median age of the participants was 50 years, with a range of 22 to 65 years. Most participants were women (80.5%) and most were in full-time employment (78%). Median experience in healthcare in general was 22 years, with a range of 1 to 46 years, while median experience specifically in palliative care was six years (range: <1 to 30) (Table 2). The non-respondents were registered nurses (n = 18), healthcare assistants (n = 5) and medical doctors (n = 12).
Participants’ characteristics (n = 41).
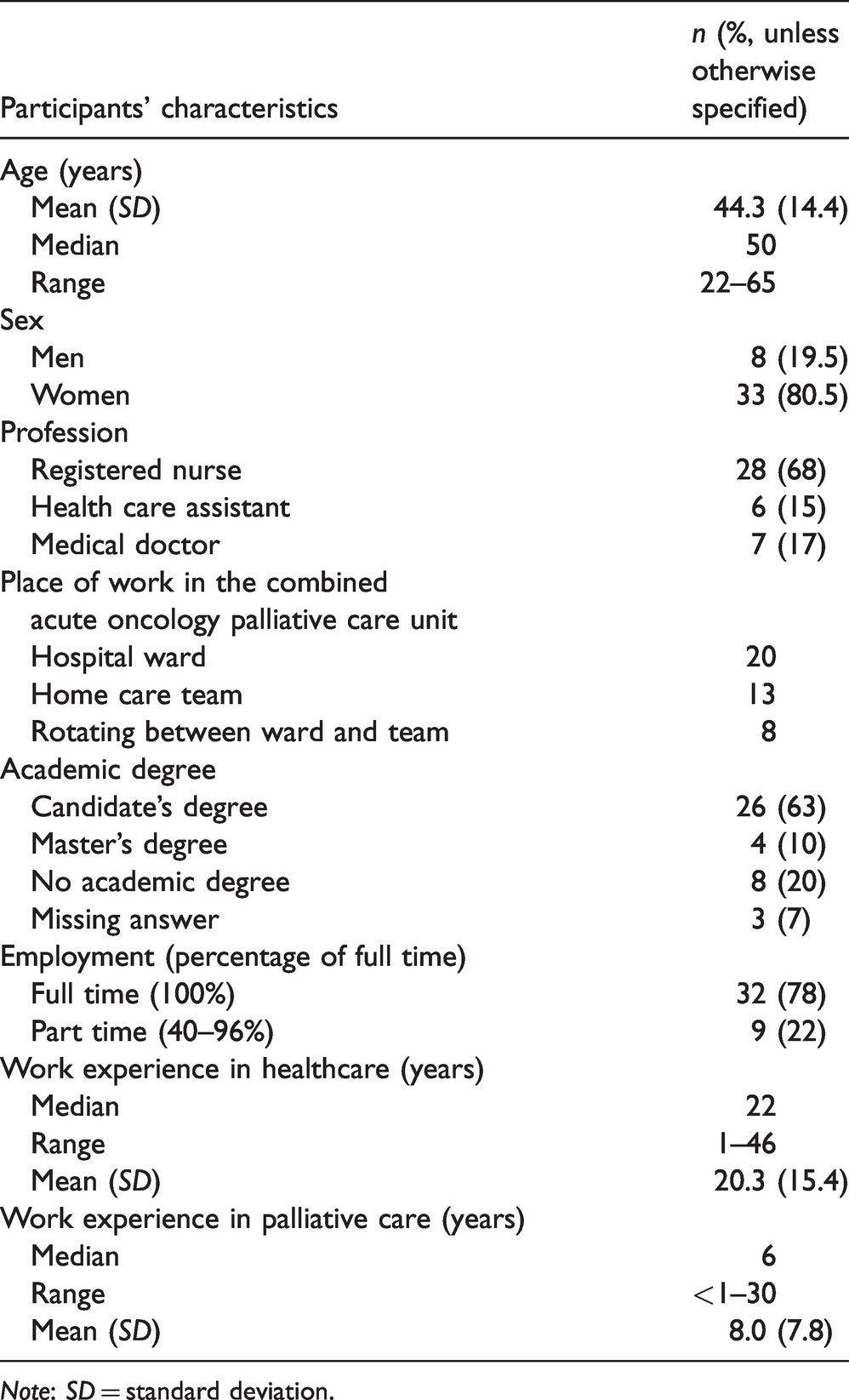
Note: SD = standard deviation.
Participants’ perceptions of the quality of care
The mean values and standard deviations (SDs) for dimensions, factors, items and single items in both the PR and the SI scale are presented in Table 3 together with p-values (Wilcoxon signed-rank test). In the text below, the results are presented in terms of the levels of PR (HCPs’ perceptions of care received by the patients) and SI (HCPs’ perceptions of the subjective importance of each aspect of the care). Levels of PR and SI are classified as high (≥3.50) or low (<3.00). The PR and SI scores are then compared.
Healthcare professionals’ perceptions of how the care quality was experienced by the patients (perceived reality: PR), and of the importance, to the patients, of each aspect of care (subjective importance: SI), by dimensions, factors, items and single items, and difference between PR and SI.

Notes: Wilcoxon signed-rank test. The level of statistical significance was assumed to be p < .025. Response scale four-point Likert-type scale, ranging from 1 (do not agree at all) to 4 (fully agree), was used for the PR and SI scales: 1 (of little or no importance) to 4 (of the very highest importance). SD = standard deviation.
*‘Other personnel’ refers to: assistant nurses, priests, physiotherapists, occupational therapists or social workers.
For the PR scale, none of the dimensions, factors or single items were scored high (≥3.50). At an item level, high levels of PR were scored for two items in the ID dimension, ‘RNs and health care assistants are respectful towards the patients’ and ‘Other personnel are respectful towards the patients’, and one item in the SC dimension, ‘Patients’ relatives and friends are treated with respect’. The HCPs gave low scores (<3.00) for the SC dimension, as well as for six factors: ‘Exhaustion’ (MT), ‘Information’ (ID), ‘Participation’ (ID), ‘Spiritual and existential’ (SC), ‘Continuity’ (SC), ‘Planning and cooperation’ (SC). None of the three single items were scored low, but 21 out of the 49 items measuring MT, PT, ID or SC were.
All dimensions and all factors on the SI scale were scored high (≥3.50) by the HCPs, except the two factors ‘Exhaustion’ (MT) and ‘Continuity’ (SC). At an item level, all three single items and 38 of the remaining 46 items were scored high. No dimension, factor, item or single item was scored low (<3.00) on the SI scale.
When comparing the HCPs’ perceptions of given care (PR) with how important the HCPs perceived the care to be to the patients (SI), the SI scores were found to be statistically significantly higher than the PR scores for all dimensions and factors. At an item level, SI scores were statistically significantly higher than PR scores for 43 out of 46 items. No significant difference was found for three items: ‘Loss of appetite’ (MT), ‘Best possible help for constipation/diarrhoea’ (MT), and ‘Other personnel support and assist patients in living the rest of their life in a meaningful way’ (SC). Regarding the three single items, SI scores were statistically significantly higher than PR scores, except for ‘Personal hygiene’ (MT).
For the three items in the ID dimension with the ‘yes’ or ‘no’ response alternatives, the results were as follows (not shown in the Table): asked about information about the responsible MD, 61% answered ‘yes’, 34% answered ‘no’, and 5% did not respond. Asked about information about the responsible RN, 90% answered ‘yes’, 3% answered ‘no’, and 7% did not respond. Regarding whether opportunity was given to patients to participate in their own individual care plan, 56% answered ‘yes’, 34% answered ‘no’, and 10% did not respond.
Discussion
The aim of this study was to investigate the perceptions of HCPs working in a combined acute oncology-palliative care unit regarding quality of the palliative care received by the patients and how important the care was to the patients.
When interpreting the high and low levels of QPP-PC PR and SI scores, there is no right or wrong, and no cut-off value exists. In the present study, the values are interpreted as high (≥3.50) meaning that participants’ responses are between ‘partly agree’ and ‘fully agree’ (PR) or ‘high’ to ‘very highest’ importance (SI), and low (<3.00) reflecting participants’ scores of ‘not agree at all’ and ‘not agree’ (PR) or ‘of little or no importance’ or ‘some importance’. This interpretation of QPP scores was inspired by previous studies of a patient population in a palliative care context.25,38 The results of HCPs’ perceptions of care quality results, and specifically, comparison of the PR and SI scores, may be interpreted in the following way: (1) Areas for improvement – care areas in which the SI score was significantly higher than the PR score may be seen as areas for improvement, in that the care received was perceived as insufficient compared with preferences; (2) Ability of services to meet patients’ preferences for care – care aspects with no significant difference between PR and SI, indicating a strength when a balance of high PR and SI scores is present. 26 Furthermore, the results need to be discussed in terms of strengths and areas for improvement.
Quality care at end of life follows a palliative care approach which addresses physical symptoms, and social, emotional and spiritual needs. Good communication, continuity and coordinated care are fundamental to quality care. 5 It should be kept in mind that HCPs tend to underestimate actual given care and overestimate the importance of different aspects of care compared with patients’ perceptions.32,33 In the present study, HCPs scored low values regarding perceptions of given care (PR) for a great number of items related to symptom relief, spiritual and existential needs, information, patient participation, continuity of care, care planning, cooperation, and coordination of care services, all of which are important components of high-quality person-centred palliative care. 4 None of the care areas received balanced high PR and SI scores, which is interpreted as indicating that the ability of services to meet patients’ preferences was low. These low scores, together with the fact that SI scores were significantly higher compared to PR scores in all dimensions, factors, and in 43 out of 46 items, imply that the overall findings of this study can be interpreted to mean that the HCPs perceived given care was insufficient and in need of comprehensive improvements. In addition, our findings add to previous studies concluding that the provision of palliative care in an acute care setting, with a care culture emphasizing cure, constitutes a challenge for HCPs.17,39
The assessment and management of symptoms is a major focus in palliative care,5,40 and optimal symptom relief is paramount for achieving comfort, maximizing quality of life and preserving patients’ self-image, enabling patients to live their lives as well as possible.41,42 In this study, areas for improvement were identified for all common symptoms causing great suffering, such as pain, nausea, dyspnoea, anxiety, and fatigue. This contrasts with the study by Ó Coimín et al. 24 reporting that pain and symptoms other than pain are well managed by hospital staff. One explanation for our findings could be that the HCPs in this study also perceived deficiencies related to planning and continuity of care, which are fundamental for optimum management of symptoms. Symptom relief regarding loss of appetite and fatigue (described as tiredness and drowsiness in the present study) was not only identified as an area for improvement, but PR values were low and SI scores indicate that relief of these symptoms was perceived by HCPs to be of less importance. It should be noted that the National Comprehensive Cancer Network (NCCN) expert panel 43 emphasize that eating and nutrition should not be forced on the patient. On the contrary, patients are expected to lose appetite at the end of life, and nutritional interventions may even be futile. 44 Similarly, fatigue may provide protection and shielding from suffering for the patient, and therefore interventions may be detrimental.43,45 The low SI scores could therefore be explained by HCPs referring to patients at the end of life, which would reflect high competence on the part of the HCPs. However, the low PR scores indicate the opposite and in fact they indicate a need for continued education in symptom management in palliative care.
Fundamental to all aspects of healthcare, and particularly to palliative care, is timely, sensitive and clear communication with the person who is seriously ill and their family members. Useful and honest information about care and what to expect in the future enables patients to participate in decisions regarding their own care and to live a meaningful life.10,42 However, HCPs in the present study gave low scores regarding whether patients were given useful information regarding different aspects of care, including what to expect in the near future. The risk of anxiety about dying, plans left incomplete, and important conversations not held is obvious. In addition, the factor ‘Participation’, where the questions applied to medical care, nursing care, and choice of where to receive care, also got low scores, and only just over half of the HCPs perceived that the patients had the opportunity to participate in their own care plan. Ability to participate in planning and decisions regarding one’s own care has been shown to be crucial for patients’ sense of autonomy and integrity and is a prerequisite for person-centred care. 12 This is also reflected in European and Swedish policy and regulatory documents, which highlight the need to incorporate patient participation in palliative care.6,20,44–47 Furthermore, care should be based on respect for patients’ self-determination and integrity, and promote supportive relationships between HCPs and patients. A positive finding was, however, that HCPs perceived that patients, as well as their families and friends, were treated in a respectful manner as they gave high scores regarding these items. Moreover, most HCPs perceived that the patients knew who their responsible RN and MD was. Being treated with respect as a person in a good relationship with responsive HCPs has been shown to be a crucial aspect of patients’ preferences for palliative care 11 and to be fundamental for preserving dignity in end-of-life care. 48
Hence, this study shows that a vulnerable group of patients, and their relatives and friends, were at risk of not receiving quality palliative care according to their needs and preferences. However, the wellbeing of the HCP is also at stake. Not being able to give the care perceived to be needed, and instead giving insufficient care, or even futile care, has been shown to be related to stress of conscience, burn-out and low job satisfaction among HCPs.49–51 Previous studies have shown that experiences of stress and dissatisfaction with care outcomes are common among nurses providing palliative care in acute care settings.15,16 Furthermore, studies have shown that low job satisfaction is associated with missed nursing care, inadequate time and resources in nursing homes 51 and an insufficient number of skilled staff in hospital care. 52 Furthermore, Kvist et al. 52 have shown that general job satisfaction of nursing staff is positively related to patients’ perceptions of overall quality of care. Therefore, future studies evaluating palliative quality care in acute care settings should also include measures related to job satisfaction and stress of conscience among the HCPs, as well as organizational and competence issues.
Patients and their families should be confident that they will receive high-quality palliative care at the end of life, irrespective of the care setting. However, we found areas for improvement regarding fundamental cornerstones of palliative care, based on HCPs’ perceptions of the palliative care quality. Our findings are in agreement with previous studies evaluating quality of palliative care in acute care settings.17,39,41 In addition, our findings are in line with studies evaluating quality of palliative care from the families’ perspective.24,41,53 Therefore, we stress the need for developing palliative care quality in settings outside hospices and specialist palliative care units. Consequently, intervention studies are needed. These should use person-centred care frameworks, as the recognition of the patient as a person contributes to experiences of dignity.11,12,54 The 6S model for person-centred palliative care has been developed based on the hospice philosophy of care, to enhance palliative care quality independently of the care setting.11,12 Self-image is the core of the 6S model, while the other concepts that are included are symptom relief, self-determination, social relations, synthesis, and strategies. The intention with the 6S model is to integrate the physical, psychological, social and existential needs of patients, and to be a tool for planning, documentation, interventions, evaluation, transfer of information between caregivers, and quality improvement of care provision. The model is based on the notion that care is co-created between the patient and the HCP, which enables the patient to live as meaningful and dignified life as possible. The 6S model therefore seems to facilitate realization of palliative care philosophy, and the content is aligned with the WHO definition of palliative care. 5 Moreover, the content of the 6S model is in congruence with the care areas of improvement identified in this study. It would be interesting to investigate whether a person-centred care model such as the 6S model is associated with higher perceptions of care quality on the part of HCPs.
Methodological discussion
The QPP-PC has been developed based on patient perspectives. It has been psychometrically tested 10 and has been adapted from the generic instrument of quality of care, the QPP. Beattie et al. 55 showed in their systematic review that the QPP has appropriate validity and reliability. The instrument used in the present study is adapted from the patient version. Adaptation consisted of changes of wording from a patient’s perspective to suit the professional perspective. However, the items were not changed in relation to content and meaning.
The original version of the QPP26 has in several previous studies been adapted and used in the same way.38,55 The QPP and QPP-PC are examples of patient-reported experience measures (PREMs). Such PREMs measure how patients experience the care they receive and should focus on aspects that are important to patients. 56 Professionals’ perspectives cannot fully replace the patient perspective and it must be kept in mind that HCPs have been shown to assess palliative care quality differently to patients. In addition, in studies using the QPP, HCPs tend to underestimate actual care received and overestimate the importance of different aspects of care compared to patients.32,33 It is also well known that MDs, RNs and HCAs tend to over- and underestimate different aspects of care quality in different ways and therefore it is desirable to be able to differentiate their answers. 31 In this study, the few responding HCAs and MDs made subgroup analysis inappropriate for both statistical and ethical reasons as individual HCPs could risk to be recognized. There is also a possibility that the differing ways of assessing items depending on profession could work in opposite ways to each other, e.g. that RNs’ underestimation for one item could mask MDs’ overestimation for the same item. However, in our study the risk for this is low thanks to the low number of MDs.
The overall RR in the study was 54%, varying among different groups of professionals, which needs to be considered when interpreting the results regarding the possibility to draw valid and reliable conclusions. The recent trend that it has become increasingly difficult to achieve high or sometimes even acceptable RR in surveys, with RR often far below 50%, is an important issue for the research community. 57 The RR was lowest for MDs (36%), and highest for RNs (60%). In absolute numbers most of the participants were RNs (68%). A limitation of this HCP study is that the results essentially represent RNs’ perceptions as the RR among MDs and HCAs was low. Repeated information about the study at workplace meetings and an extra reminder, as well as possibility to choose between questionnaire either on paper or via web could be one way to increase the RR. Moreover, as RNs were in a great majority among the responders it is reasonable to assume that the result largely reflects their perceptions. Therefore it is important for future studies to ensure an equal response rate across healthcare professions.
In the present study the QPP-PC showed α values >.7 for most dimensions and factors. Similar results were found in a previous study where QPP-PC was used to measure patients’ perceptions. 25 However, these dimensions and factors consisted of only three items, which may have influenced the low Cronbach’s α values. 36 The QPP-PC instrument measures both the perception of care received and the importance of the care aspects, contributing to the content validity of the instrument and the study. HCPs in our study scored most of the care aspects as being of high importance, which is in line with previous studies of patients in palliative care. 25 These results support that the QPP-PC professional version has appropriate validity. Since the PT dimension and four of the factors had low alpha values, analysis was performed at item level as well as dimension, factor and single-item levels. To avoid a type 1 error the significance level was reduced to .025, as recommended by Field. 36
Conclusion
In this study, conducted in a combined acute oncology-palliative care unit, providing high-quality palliative care was perceived to be a challenge by the HCPs. The results show that HCPs perceived comprehensive quality deficiencies and the need for improvements in fundamental aspects of person-centred palliative care such as symptom relief, spiritual and existential needs, information, patient participation, continuity of care, care planning, cooperation, and coordination of care services. However, these findings need to be confirmed in a larger sample with a higher RR. Future studies should investigate the effects of implementation of person-centred palliative care models based on the hospice philosophy of care quality from patients’ and families’ as well as HCPs’ perspectives. These studies should also include HCPs’ experiences of job satisfaction and stress of conscience, which have been found to be important mediators for overall quality of care.
Footnotes
Ethics approval and consent to participate
The study was approved by the Research Ethics Committee at Karlstad University (DNR No. C2018/131). All participants in the project have given written informed consent.
Author contributions
Study design and data collection: CO, EE, MR, and ML; data analysis: CO, EE, MR, and ML, manuscript preparation: CO, TS, BWL, ML, and critical review of the manuscript: CO, TV, BWL, EE, MR, and ML. All authors approved the final manuscript.
Acknowledgements
The authors would like to thank all HCPs in the participating unit.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.