
Abstract
Cultural diversity in the healthcare sector is increasing, but knowledge about culturally diverse teams is limited and is needed to meet the challenges of the 21st century. The purpose of the study was to explore the contribution of an inclusive climate to the work of culturally diverse healthcare teams. This study had a qualitative descriptive design and was based on 17 interviews with healthcare professionals in an acute unit of a regional hospital in Sweden. A general inductive approach was used for analysing qualitative data. The COREQ checklist was used. The findings demonstrated the importance of highlighting the value of differences and similarities, by emphasising each individual’s uniqueness and looking beyond cultural differences; stimulating meaningful interactions by boosting social exchange and inspiring mutual support; and establishing engagement structures by encouraging structures for engaged leadership, fostering structures for cultural awareness, creating structured learning areas and striving to structure teamwork practices. In conclusion, the findings demonstrate the importance of introducing an inclusive climate into healthcare organisations and of reaping the benefits of cultural diversity in healthcare teams. It is also important to promote inclusive practices proactively and consistently in the workplace.
Introduction
Cultural diversity, defined here as a perceived and subjectively experienced presence in one social system of people with distinctly different group affiliations of cultural significance, 1 in the healthcare sector is increasing, and the delivery of care is more and more performed by team constellations 2 composed of culturally diverse individuals (cf. Ellis). 3 However, knowledge about how such teams function and how they should be managed is limited. 4 To meet the challenges of 21st-century healthcare systems, professionals require a common vision centred on a commitment to meet patients’ needs.
Five core competencies have been identified for all healthcare professionals, regardless of discipline: the delivery of person-centred care; working as members of an interdisciplinary team; an emphasis on evidence-based practice; a focus on quality improvement approaches; and the use of informatics. 5 However, the training of healthcare professionals still largely focuses on the knowledge and skills of individual practitioners. 6 Recent developments, however, indicate a shift toward more team-based healthcare delivery, driven by the expectation of improving delivery processes and patient outcomes, and lowering costs in comparison with non-team-based approaches. 7 The development of team-based work has been shown to be key in improving the quality of a nation’s health systems, 8 and ‘as an essential tool for constructing a more patient-centred, coordinated, and effective healthcare delivery’.9(p.3) Yet hurdles in creating effective teamwork processes in healthcare often lead to adverse events, accounting for up to a third of all incidents,10,11 and healthcare practitioners are not typically trained for team-based work.
Work in healthcare teams (e.g. palliative care teams, rehabilitation teams, and stroke teams) is particularly challenging. 4 Such work is highly interdependent and requires a collaborative effort to address complex issues through an integrative set of approaches. 12 Group diversity in age, gender, social class, and/or culture may offer a variety of benefits, but brings complex challenges to the effective functioning of healthcare teams. 13 More specifically, the literature points to diversity that goes beyond demographics, and indicates that cultural diversity is probably the most challenging issue these teams need to address, given the varied needs of a heterogeneous population. 14
The literature on healthcare teams has tended to focus on work processes such as communication, collaboration, and decision-making, 15 and their performance implications for patients and teams. These include patient safety, 16 accuracy in team diagnosis, 17 and team effectiveness. 18 This body of literature needs further development regarding the power and influence of diversity in healthcare organisations. 4 More specifically, empirical research is slow to accumulate, particularly regarding cultural diversity 13 and contextual aspects such as organisational culture, organisational structures, and leadership qualities that enable healthcare teams in their performance (cf. Kirkman et al.). 19
Recent theoretical and rare empirical studies on team cultural diversity suggest that inclusiveness of the organisational and team-related climate, leadership, and practices may lead to improved outcomes for diverse teams.20,21 For example, Gonzalez and Denisi 22 and Nishii 23 suggest that an inclusive climate contributes to employees’ perception that their teams or organisations value diversity and individual differences and promotes interpersonal integration among diverse employees, and employee involvement in decision-making. It is further suggested that inclusive leadership that is accessible, available, and modelling openness 24 will bring out the best in diverse teams. Finally, several studies5–26 suggest that inclusive practices in the workplace may facilitate the functioning of culturally diverse teams. Only a few studies could be identified that explored cultural diversity in healthcare teams with a specific focus on these teams’ functioning.26–29 The findings of these studies suggest that to understand how culturally diverse team function, one has to gain a better understanding of the characteristics of the context they operate in. Thus, the purpose of this study was to explore the contribution of an inclusive environment to the work of culturally diverse healthcare teams.
Materials and methods
This study has a qualitative descriptive design. 30 Data were collected through semi-structured interviews with healthcare professionals in an acute unit of a regional hospital in Sweden during 2018. The unit was chosen for its team-based organisation and for the dynamism and complexity of the assignments performed by its teams. The content analysis was inspired by Thomas’ 31 general inductive qualitative content analysis approach for analysing qualitative data. The consolidated criteria for reporting qualitative research (COREQ) were used. 32
Participants and recruitment
The selection of participants was purposive, i.e. they needed to have experience of working with individuals of cultural backgrounds different from their own. The unit was chosen for its team-based organisation and for the dynamism and complexity of the assignments performed by its teams. A total of 17 healthcare professionals (seven physicians, five registered nurses, and five nurse assistants) participated in this study (Table 1). The researchers first received permission from the head of the clinical unit, and then TU and EE provided verbal information about the study during staff meetings where the authors also described the background of their interest on the research topic. The staff also received written information about the study that emphasised the voluntary nature of participation and the right to withdraw at any stage. Interested staff members were asked to contact a research team member by email to set up an interview. All study participants signed an informed consent. No participant withdrew from participation during the study.
Sample characterisation.

Data collection
Semi-structured individual interviews were conducted by either TU or EE and took place in a secluded room at the unit without the presence of any observer. The interviews were based on an interview guide, that was pilot-tested with a registered nurse (RN), experienced in working in culturally diverse teams (test interview not included in the analysis). Our interview guide focused on the interviewees’ experiences of working in culturally diverse teams and started with an initial discussion on cultural differences in the healthcare context. Thereafter, the interviewer introduced a question related to the interviewees’ experiences of working in culturally diverse healthcare teams, followed by questions related to organisational structure and team-related outcomes. Throughout the interview, follow-up and probing questions were asked to deepen the narratives. For example, the participants were asked to exemplify and reflect on their experiences of their work environment. The interviewers also ensured that the interviewees did not deviate into sharing general professional experiences, and only revealed culturally diverse team-specific experiences. The digitally recorded interviews lasted about 30–50 minutes and were professionally transcribed verbatim. All transcripts were checked for accuracy by the authors.
Data analysis
The data analysis was inspired by a general inductive approach as described by Thomas. 31 The analysis was conducted in five steps: 1) performing an initial reading of the text, 2) identifying specific text segments (i.e. meaning units) related to the aim, 3) labelling segments to capture content (i.e. coding), 4) grouping related labels into sub-themes, and 5) reducing overlap and redundancy among the sub-themes and grouping them into themes. 31 The analysis process was performed as a constant movement between the text and the labels, and the labels and the themes. All authors performed the initial reading of the text, while the first and second authors conducted steps 2 and 3. All authors were involved during the last two steps (4 and 5) of the analysis. The overall analysis proceeded until all four authors reached consensus.
Authors’ preunderstanding and experience
The group of authors is diverse. They have education and work experience in healthcare; EE and AKE are both female registered nurses and SP is a male physician. TU (male) has a background in business administration and a research focus on multi-cultural teams. EE and AKE have in-depth experience in qualitative methods, and in interview studies in particular, and TU and AKE hold PhDs. TU and SP have a non-native background, while EE and AKE are native Swedes. All authors have experience of working in culturally diverse teams.
Ethical consideration and approval
The study was conducted in accordance with the Declaration of Helsinki on ethical principles. 33 Formal ethical approval was received from the Research Ethics Committee in Lund, Sweden (2018/77). There is always a risk that participants might feel pressured to participate in a study; therefore, the voluntariness and the right to withdraw were stressed on several occasions in the study. To safeguard confidentiality, all data were coded for name and other aspects that could identify the participants or their workplace. Data were kept apart from the coding list and stored in a security locker without access by unauthorised persons.
Results
The analysis revealed that an inclusive environment contributed to the work of culturally diverse healthcare teams by highlighting the value of differences and similarities, stimulating meaningful interactions, and establishing engagement structures, represented as main themes with internal variations seen as sub-themes (Figure 1).
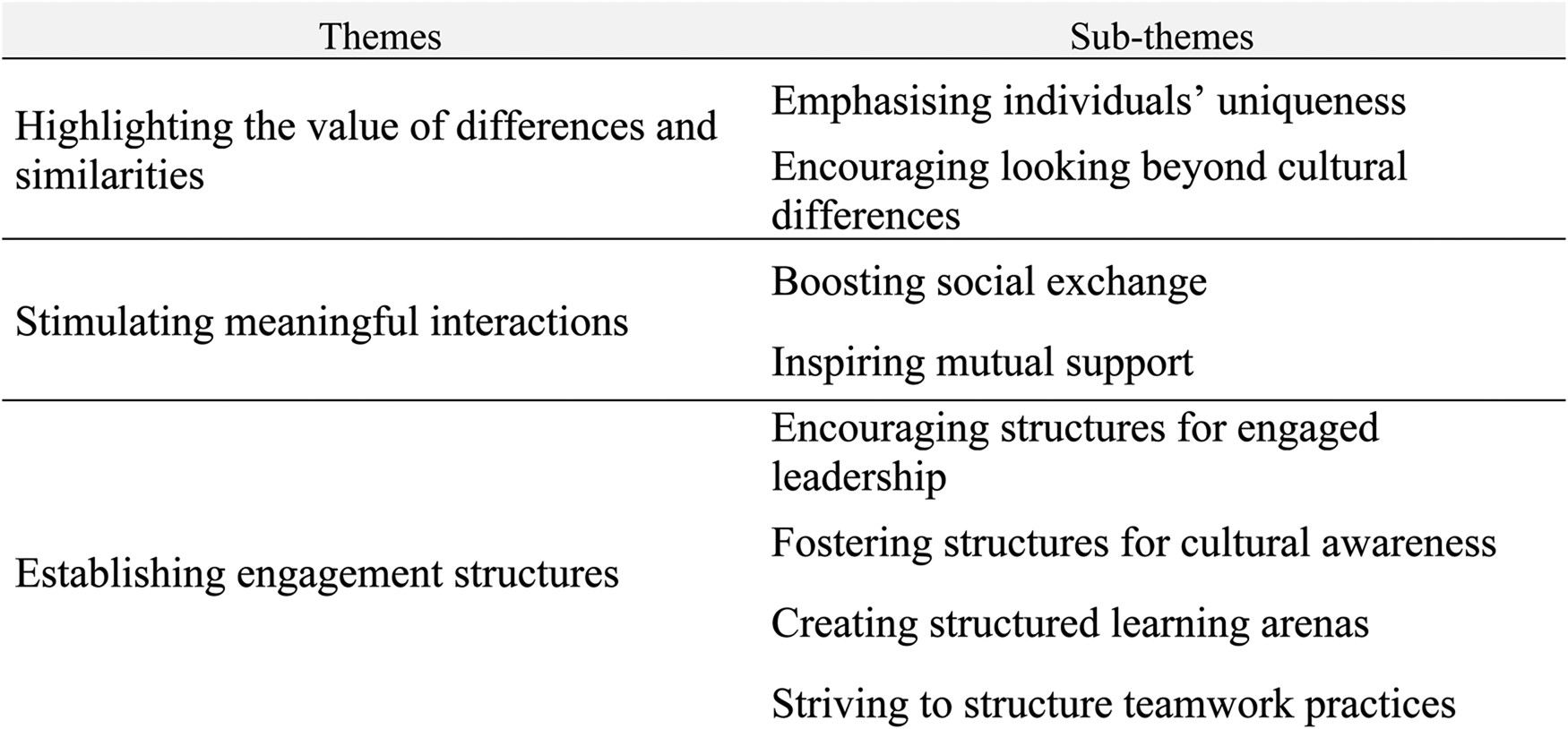
Themes and sub-themes.
Highlighting the value of differences and similarities
Emphasising individuals’ uniqueness
The interviewees reported that their work context predisposed them to see the value of individual uniqueness and the benefits of the uniqueness represented by cultural dissimilarities. Discussions between staff members on the benefits of cultural differences were said to arise primarily regarding interactions with diverse patients. These discussions usually highlighted the patients’ needs and described how the linguistic and cultural diversity of the staff helped to meet these needs. The staff also suggested that focusing on the benefits of individual differences in their interactions led to a realisation of the importance of ‘bridge builders’ – individuals possessing knowledge of both Swedish and foreign cultures and languages. These ‘bridge builders’ were considered integral to the environment and teams they operated in and were praised for their contributions to improving teamwork, reducing patient–professional misunderstandings, and developing an increasingly person-centred approach toward patients. As one physician (I16) explained: [Having her/him] is amazing, lucky for us … This person has a [multiplicity] of cultural backgrounds … And this person understands both Western culture and [the other culture] and … can translate [between them]. This person can explain why it was wrong, and … might also say ‘But if you do this instead, I think it will be smoother’. So, this person can help us to avoid cultural clashes.
The interviewees viewed exchanges of experience and knowledge in different domains as essential in their work environment since these encourage interaction between culturally different individuals. The interviewees felt that, in their work context, emphasis was placed on the value brought to the team by culturally diverse members and on the knowledge and experiences embedded in cultural differences. Emphasis on the benefits of cultural differences was related to the learning approach utilised in the workplace. Cultural differences were described by interviewees as opportunities to learn from each other and as a source of inspiration. One nurse assistant (I2) explained: Yes, we have someone who comes from a different culture … And we ask that person many questions. And that person answers gladly, on many ‘whys’ and ‘hows’ … You can sometimes react to why they do what they do in some instances, patients’ families, I mean. And then that person may have an answer, they do it like that in their country or in their religion or … yes, I don’t know how to explain it. Then you get a different view and understand it better.
Interviewees felt that a learning approach was ingrained in the inclusive practices of the context and brought opportunities for unexpected knowledge and skills to emerge and for staff to feel appreciated. The interviewees with a foreign background felt that their skills were highlighted as unique and instrumental in a variety of situations. They also felt that the work environment allowed quick entry and fast integration.
Encouraging looking beyond cultural differences
The interviewees felt that the working environment provided them with opportunities for open discussion about the difficulties associated with cultural differences in teamwork, and for reflection on how to overcome these difficulties. They explained that these open and reflective discussions brought them together and helped them to look beyond these differences, instead of emphasising the personal characteristics and experiences that either did or did not align with the aims of the healthcare team. Rather than dwelling on the initial difficulties experienced by foreign staff, these discussions often moved further to focus on the importance of personality, characteristics, social skills, and ability in becoming part of the group. Irrespective of background, all the interviewees expressed their awareness of the initial hardships of fitting into the organisational context, especially for those with a foreign background. They also expressed understanding of the time needed to prove oneself as a person and come to understand the new environment. According to one physician (I16): It is difficult [to comprehend] the Swedish way of working and … to understand linguistically what we [in the team] and the patients have said and [to absorb it].
The interviewees considered cultural background and personality to be intertwined, and said it was sometimes difficult to identify the initial cause of difficulties in understanding Swedish values and their applicability to healthcare. They also emphasised that the environment predisposed them to view each other as people who were valuable assets for the organisation; thus, when difficulties arose, these were primarily attributed to personal qualities rather than to cultural differences. Most interviewees stated that looking beyond cultural differences and focusing on personal traits and their value were important context characteristics. One of the physicians (I11) explained: My starting point is that we must always understand where we all stand. We must strive to have communication, and it can take some time to find out where the language difficulties are and where there are different ways of thinking.
Interviewees also explained that their environment was characterised by a solution orientation, and that even when individuals in the environment differed in some dimensions, they were predisposed to look beyond these differences to concentrate on common ways of resolving situations. Thus, the focus was on how to move past these difficulties to address whatever situation may arise.
Stimulating meaningful interactions
Boosting social exchange
Throughout the interviews, irrespective of cultural background, the interviewees described their environment as one that encouraged interaction through open communication and joint activities, resulting in a respectful and social team climate. The interviewees said that the environment predisposed them to socialise outside of work and beyond professional or cultural differences. They felt that by encouraging socialisation, the environment supported teamwork better due to the resulting social connections. The interviewees further recounted how special care was taken of newcomers, irrespective of background, to enable their smooth transition into the new context and make them feel welcomed. The interviewees reported that the openness of the environment and the freedom to express opinions in various forums were other aspects that made culturally diverse teamwork a positive experience. One nurse assistant (I5) summarised: We have a friendly climate, and we accept and respect each other. And I think it is because … we encourage respect for the one who is coming [into the team] as a new person. People are valued as much [when new] as when they have been in the group for a long time. People try. And I think that is very important.
The environment was also characterised by the interviewees as playful and flexible, which led to constructive problem-solving while maintaining positive relations at work. Even when stressful situations arose, putting strain on teamwork, the situations were solved. The interviewees also commented that an environment of calmness and politeness was conveyed through the tone of conversations and the ways in which people expressed their opinions. When discussing her experience of joining the department and working in it, one registered nurse (I8) summarised: Everyone is very open. They talk to you. You aren’t left out of the group. There is a very playful level here, very easy going. The atmosphere is very good. And it’s like … You notice that some days when it is very stressful, people try … so that it is very positive anyway. So, I think it made me feel welcome in the group because it was so … There are hardly ever any hard words. There are no sour faces.
Inspiring mutual support
The interviewees reported a feeling of willingness regarding mutual support in both the department in general and the teams they worked in, particularly during stressful or difficult situations. The interviewees said that taking care of each other, being helpful, and being able to ask for help were engrained in the work climate. They saw this as being very helpful when working within a culturally diverse healthcare team, since this mutuality allowed the team members to focus on tasks rather than on differences. Mutuality and mutual support were reported to reduce the hierarchical differences between team members, allowing freedom of action in different situations. A nurse assistant (I1) explained: And I think that relationships among the staff here are like … Everyone is taking care of everyone else … And people offer help to others. Even if you have a lot yourself, you offer help anyway, like, ‘I can help you. I can do it so that you manage to eat a bit and so on’. And we … Yes, we are all simply very caring toward each other.
The interviewees reported that the focus on mutual support inspired by the environment allowed fluid decision-making through which professional differences became salient and emphasis was placed on the patients and on their needs and safety. The interviewees reported that different professionals delegated decisions to each other and supported the resulting decisions; they felt that this shifted the focus within teamwork from differences to an appreciation of each other’s competences and the value these brought. One of the physicians (I11) recounted: The joint focus has until now been on the patients. There is a high degree of responsibility. We help each other. Rather prestige-less. Someone might say, ‘I don’t understand that. Would you please consider helping me to think?’ That is how we do it. And I think that the department benefits from it.
Establishing engagement structures
Encouraging structures for engaged leadership
The interviews revealed that the managers on all levels had an important and positive impact on teamwork functioning and on integrating new staff into the team. The nurses and nurse assistants said that the unit managers were always present and engaged in the daily work and viewed being available for questions when uncertainty arose as a natural aspect of the work environment. The availability of and support from the managers was seen as especially valuable for newly recruited staff from different backgrounds, as it allowed them to find their role in the profession and in teamwork more easily. One of the nurse assistants (I3) explained: Our unit manager is after all … like, here every day. And [NN] is in and out of here and checks how we are with the workload and how we work. And you can ask [NN] for help if there is a need, and [NN] is happy to help. So that’s how it is. [NN might] have limited insight into whether we are doing what we should. But at the same time, that manager is here if there is something.
The presence and involvement of the manager was seen as particularly important when support was necessary in difficult situations and when disagreements arose between team professionals regarding the care of patients who were severely ill. The staff reported a conscious strategy on the part of the managers to provide support to all professions, regardless of background, so that everyone felt included in the workplace and, subsequently, in the teamwork. The managers were frank about their conscious strategy of inclusion and said that they both aimed to create an inclusive environment and were inspired by the inclusive environment to apply structured leadership when necessary. As one of the leading physicians (I12) explained: I want to be inclusive, and I hope I am, but if I am, it can only be known by them [subordinates]. That’s my intention.
Fostering structures for cultural awareness
The managers reported that they actively worked on recruiting staff from different cultural backgrounds and helped them to integrate into the working group. The interviewees expressed an awareness of the benefits and drawbacks of cultural differences yet suggested that cultural differences were a natural part of society, and that being aware of these differences and openly discussing how to address them was a way forward. A physician (I12) explained: I believe in human development in some way, and then I still think that if you have people from different cultures in a working group, that it creates a habit, maybe you can call it, that helps you in dealing with situations.
The interviewees reported that to facilitate inclusion in the working group, the superiors openly discussed different values and views regarding immigration in general which they felt increased awareness and encouraged a reflexive way of approaching these differences. It was said to be rare for staff with different cultural backgrounds not to work well with other professionals or not to be included in teamwork. In the rare cases when this happened, management intervened by addressing the issues in an open and culturally aware manner, thus gaining support from the department employees. When describing a situation in which a foreign-trained physician was offered help to integrate into the environment, but failed to do so after several months of training and support, one of the physicians (I14) recounted: We tried to help bring that person in as well … so that person could act as a physician, but we felt that it was not working properly. And then the management was absolutely committed, because then it was also about resources. Should we hire this person and invest another six months, or even permanently hire them, or not? It was a very, very difficult decision to make, and ultimately, we did not offer this person the position.
Creating structured learning arenas
All the interviewees expressed an awareness of the difficulty and importance of understanding each other’s cultures and how the learning experiences from working with different individuals could facilitate teamwork. They explained that within the work environment, common arenas where this learning took place were provided by the organisation and were embedded into the institutional structure and practices. For example, start-up meetings in the morning, reconciliation meetings in the afternoon, coffee breaks, and meetings related to work improvements and development served as arenas where everyone was encouraged and expected to participate, yet was given sufficient flexibility to opt out. To facilitate teamwork, the department had clear procedures, and clearly communicated and documented expectations that provided guidelines for joint decisions, where cultural aspects were taken into consideration. This environment and the learning arenas it created were felt not only to facilitate teamwork, but were also felt to serve the important function of recruiting new talents into the department and teams. One physician (I14) recounted: But when I came here, I remember that an argument for me to come was that people here worked a lot with change management and work improvements. I had a boss then who was driving it, a lot; and then it was like this—it was included in everything. Everyone would come up with suggestions. Everyone would be involved in these processes. So, I got involved early in a [developmental] process at the department.
However, the interviewees reported a need for even more common space to increase cultural competence, such as training days and opportunities to reflect with the team on different cultural aspects of caring situations. The interviewees expressed willingness to learn more about cultural differences and how to deal with different work situations. One registered nurse (I6) explained: I want a day where, as a staff member, you can speak without anyone getting upset. Do you follow? So that you should be allowed … so that we should be allowed to vent to each other: ‘How do you do it?’ and ‘How do I do it?’ … This [i.e. cultural diversity] is nothing that goes away. It doesn’t disappear. It will increase. It will be part of our everyday life. I’d rather have seen someone training us even more; that we had been taught even more.
Striving to structure teamwork practices
An inclusive environment was considered ingrained in the workflow of the department and within the teams. The interviewees felt that people were encouraged to cooperate with each other regardless of profession, and that exchanges between team members were dictated by the approaches toward teamwork learned in the workplace. Furthermore, there was an acute awareness of the importance of teamwork and how teamwork was organised. The interviewees explained that teams were constructed on daily basis, and that during team formation, team members’ experiences were taken into consideration so that new members could work with more experienced ones. This was considered a smooth way of accommodating differences and transferring knowledge, while access to peer learning and a practice of supervision was important for successful team integration. The staff felt positively about how such aspects were routinised in their work, and about how this had deepened their understanding of one another and of how teamwork functioned. One registered nurse (I8) summarised: I think it is very much about how people encounter each other, and what kind of introduction you get. Here, you have a very long introduction process. You follow a couple of different [people] and you get into the group very well, I think. Everyone is very open.
Discussion
Inspired by the literature on the inclusiveness of organisational and team-related climates,20,21 the purpose of this study was to explore the contribution of an inclusive environment on the work of culturally diverse healthcare teams. The findings provide an understanding of how positive aspects of cultural diversity manifest themselves in everyday practices of healthcare teams, and reveal three specific contributions that an inclusive climate makes.
The first contributing component of an inclusive climate is that the team members value differences and similarities. This was seen in our results which showed how the team emphasised individuals’ uniqueness and encouraged each other to look beyond cultural differences. Our results suggest that by emphasising differences and similarities, culture-related tensions within the team can be reduced. These findings align with studies in team management research, which point out that inclusive practices emphasise the positive aspects of diversity and promote fairness in team relations (e.g. Gonzalez and Denisi). 22 While previous research alluded to how an inclusive climate could be manifested in interaction and engagement structures (e.g. Uman et al.), 26 it has not been sufficiently clear how the inclusive context empowers culturally dissimilar individual members of the team. Our results give a new insight into this domain by showing how an inclusive context emphasises the uniqueness of individuals and at the same time enables them to look beyond this uniqueness when working in culturally diverse healthcare teams. The results show that an inclusive environment is characterised by the value that each individual brings to the team, which is in line with the review by Shore et al., 21 conceptualising inclusion as involving belongingness as well as uniqueness. An inclusive environment, in turn, appears to create a friendly atmosphere, described by Edvardsson and colleagues to be an important aspect of a person-centred climate,34,35 i.e. a climate characterised by a welcoming atmosphere that focuses on individuals. Thus, highlighting the value of differences, similarities and uniqueness seems to be essential for an inclusive climate, but also is important for a person-centred climate.
The second contributing component of an inclusive climate is that it stimulates meaningful interactions in the team. This was seen in our results which showed how the team was empowered through social exchange and mutual support. It is reasonable to assume that this in turn reduces conflicts and misunderstandings and increases the possibility to view each other as individuals rather than as isolated work units. In other words, work groups appear to become more cohesive in this environment, resulting in more effective team functioning (cf. Delva et al.) 36 and increased team ability to focus on patients’ needs rather than on team dynamics. These findings are in line with recent studies on team effectiveness that suggest that mutual support in a healthcare team is an essential element in the provision of high-quality care. 37 In times of constraint concerning resources and time in the healthcare sector, there is a risk that social and interpersonal aspects may be downgraded in favour of a more task-oriented focus (cf. Beck et al.). 38 However, our results highlight the importance of creating space for meaningful exchange and mutual support even though as it seems to enable work effectiveness, thereby saving time.
The third contributing component of an inclusive climate is that it establishes engagement structures in the team. This was represented in our results by the encouraging structures for engaged leadership, fostering structures for cultural awareness, structured learning arenas and teamwork practices. These support structures are manifested in leadership practices (cf. Chatalalsingh and Reeves) 39 that are integrated into staff awareness of how to work with culturally different others. The findings are supported by leadership literature 24 suggesting that engagement structures based on leaders’ ability to communicate clear expectations and provide inclusive leadership to employees are important facilitators of well-functioning teams in the workplace. 40 Thus, leadership and the organisation of care are fundamental for successful teamwork as initiatives and prerequisites need to be supported by the management. This is in line with the literature on person-centred leadership,41,42 showing that the manager is essential for leadership, and for the development, and maintenance of high-quality care. McCormack and McCance 43 highlight how the organisation and management plays an important role in the care environment and how it in turn affects the teamwork where different professions’ competences can be integrated and taken advantage of. It has to do with shared decision-making, relations within the group and a supportive organisation that allows for development, critical thinking and risk-taking. It is thus important that the leadership support a composition of the team to enable positive results for the patients in their care, where diversity and inclusiveness seem essential.
While this study provides some answers to the question of how an inclusive environment contributes to the work of culturally diverse healthcare teams, there is a need for further research in several areas. For example, it seems important to further explore other components that might enable culturally diverse healthcare, but also the characteristics of inclusive leadership.
Study strengths and limitations
The trustworthiness of the study (cf. Lincoln and Guba) 44 needs to be highlighted. Even though the sample varied concerning profession, age and experience, it should be mentioned that only a few of the respondents themselves had a non-native background, which in turn might affect the transferability of the results, However, they all had extensive experience of working in culturally diverse teams, which was the focus of the study. Even though some of the interviews were relatively short, the data collected were rich and we did not find any diverse cases. We also found the data to be consistent with the findings, and have illustrated this with quotations from the original data in the results. As all authors were involved in the analysis of the data their preunderstanding was constantly challenged. Their diverse backgrounds also strengthened the trustworthiness of the study as their professional backgrounds, experience of the healthcare sector, genders and countries of origin varied and brought different perspectives to the analysis.
Practical implications
This study has several practical implications. To enable culturally diverse healthcare teams, managers need to support an inclusive climate by emphasising the value of diversity, while at the same time stressing the importance of professional norms and values that the team members can unite around. Our findings also support the importance of natural arenas for interaction such as social activities or even just coffee breaks where people of different cultures can meet and interact. There are further implications on the organisational level that point at the importance of fostering engaged and inclusive leadership. These concern both the team and organisational levels. Finally, our findings point to the importance of how healthcare professionals working in culturally diverse teams socially engage with their culturally different colleagues and how they can provide them with unconditional support.
Footnotes
Acknowledgements
We are most grateful to the healthcare professionals for sharing their experiences and to the management of the hospital for supporting accessibility. We are also grateful to Proper English for revising the language.
Author contributions
Design: TU, EE, AKE and SP, data collection: TU and EE, analysis: EE, TU and AKE, drafting the paper: TU had the main responsibility. All authors read and provided substantial input to the final version of the paper.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Platform for Collaboration for Health, Kristianstad University, Sweden. T. Uman acknowledges funding from the Jan Wallanders and Tom Hedelius Foundation, and the Tore Browaldhs Foundation (grant number 20-0263).