
Abstract
Although pro re nata medications (PRNM) are widely used among older patients in long-term care, current knowledge about nurses’ PRNM management is scarce. The study aim was to describe which knowledge sources nurses working in sheltered housing for older people use when making decisions regarding PRNM. This was a qualitative interview study with registered nurses (n = 4) and assistant nurses (n = 4) working in sheltered housings in mid and eastern Norway. Data analysis was based on qualitative and abductive content analysis, where evidence-based practice (EBP) was used in the abduction. The COREQ checklist was followed. Several knowledge sources are used when making decisions regarding PRNM, that represent the four elements of EBP. ‘Practitioner experience and judgement’ was a prominent source of knowledge among the nurses, while ‘Evaluated external evidence’ was less emphasized in PRNM decision-making. The results support previous research on EBP in nursing, and bring new knowledge regarding PRNM in the context of sheltered housing. To achieve appropriate and safe management of PRNM, there is a need to support nurses’ decision-making process, e.g. through PRNM guidelines and systems for documentation and information exchange. EBP in PRNM decision processes should be given attention, utilizing all elements including ‘Evaluated external evidence’ as a knowledge source.
Keywords
Introduction
Medication administration is an important part of nurses’ tasks. Pro re nata medications (PRNM) (also referred to ‘as needed’ or ‘as required’) are administrated as a response to symptom(s) that occur spontaneously and are not treated with regular medications. 1 Although PRNM are widely used among older patients in long-term care, current knowledge about nurses’ administration of these medications is scarce and relies mainly on data from nursing homes. In this article, we focus on the knowledge sources nurses use when administrating PRNM in sheltered housing. For people having medication management assistance, the judgement for giving PRNM is based on both nurses’ and patients’ thinking.2,3 Such clinical decision-making involves deciding when medication should be used, how much to administer, and which medication to administer. 4 To ensure safe and efficient decision-making, nurses need solid and comprehensive medication competence. An integrative review has specified nurses’ medication competence to involve knowledge of anatomy, physiology and pharmacology, as well as skills in communication, interdisciplinary collaboration, information seeking, medication calculation, medication administration, assessment, evaluation, documentation and promotion of medication safety as part of patient safety. 5 A systematic review found insufficient evidence addressing PRNM and patient safety, and suggested that PRNM safety issues and adverse events are under-recognized. 1
Healthcare providers are required by law to contribute to patient safety and quality in the healthcare service, 6 including ensuring safe medication administration. 7 To ensure the correct use of PRNM, decisions about administration should be based on a conscious use of various knowledge sources, including the patient’s preferences, the nurse’s expertise, and the critical appraisal of research evidence. Furthermore, the code of ethics of the International Council of Nurses states that nurses should be active in developing a core of research-based professional knowledge that supports evidence-based practice. 8 The thinking and decision-making process in clinical practice is a multi-layered, multi-component capability that enables nurses to make judgements and decisions in the complex area of healthcare settings. 9 The evidence-based practice (EBP) model was developed from evidence-based medicine, and is recognized as a method to improve healthcare quality and patient outcomes that can be used in clinical practice in such decision-making processes. 10 EBP implies the necessity to use several knowledge sources when making clinical decisions, where evidence is extended beyond research.10–12 The EBP model has four elements: 1) Evaluated external evidence, 2) Stakeholder’s preferences and values, 3) Practitioner experience and judgement, and 4) Context and circumstances.11,13 The decision-making takes place at the intersection of all four, but the size and influence of each element vary with each decision. An integrative review found nurses to be familiar with and positive about EBP, but they perceived their own knowledge and skills to be insufficient for using EBP in practice. 14
Studies indicate that nurses’ part in PRNM decision-making is significant both in care homes and nursing homes,15–17 and may be affected by which healthcare providers are at work and the culture of the clinical environment.3,16,18 Medication management is a multi-step process involving judgements from healthcare providers during different phases: from prescribing to dispensing, administering and evaluating the effects of the medication.7,19 There is a lack of studies reporting on why PRNM are used.20,21 A systematic review regarding psychotropic PRNM in long-term care settings found variations in medication management, and identified a need to explore factors affecting PRNM administration. 21 In nursing homes, frequent use is associated with advanced age, dementia, a higher number of regularly scheduled medications, and length of stay. 20 Most residents in sheltered housing have several PRNM on their medication lists, but the frequency of administration varies. 18 The most commonly used PRNM are mild analgesics, tranquilizers and laxatives.16,18
In Norway, residential care for older people is provided under institutional care (nursing homes) and sheltered housing (assisted housing).22,23 Sheltered housing may have much in common with nursing homes but differs in both economical and juridical organization. 22 Sheltered housing for older people is mostly for people aged > 65 years, and the municipalities are responsible for administrating a suitable service. Sheltered housing is heterogenous with respect to staff numbers and level of care, where the residents may receive help with activities of daily living, including managing medications, if needed. 22 By legislation, the residents live in independent homes and rent or buy an apartment from the municipality, and nurses provide home-based services. 24 In principle, mainly registered nurses (RNs) manage medications, but this responsibility may also be delegated to other healthcare providers, such as nurse assistants (NAs). The responsibility to administer medications is given by the head of unit, who is responsible for verifying that the providers possess the appropriate competence. 19 Furthermore, a nursing home is organized with an attending physician who prescribes PRNM on the patients’ medication lists or in a medication directive valid for all patients in that nursing home.7,25 However, in sheltered housing, residents make appointments with to their general practitioners (GPs) who must prescribe PRNM on the individual residents’ medication lists. Thereby, nurses in sheltered housing must collaborate with several GPs regarding medication management.
There has been a lack of focus on nurses’ decision-making and use of different knowledge sources and evidence regarding PRNM. Although PRNM are on the medication list, nurses must decide whether to administer the medicine, based on judgement of each unique patient situation, where the time allotted is usually short. For nurses in sheltered housing, who are part of home care nursing services, medication administration may also be challenged by contextual factors and lack of continuity, 26 and the decisions made regarding PRNM can vary. 3 The aim of this study was to describe the use of knowledge sources among nurses in decision-making processes of PRNM. This knowledge is important for implementing procedures and improving practice, which is significant for leaders of primary healthcare services and educators of nurses. Subsequently, nurses and their patients will benefit from in-depth knowledge on the topic, as EBP is focusing on healthcare quality to improve patient outcomes. The following research question guided the study: Which knowledge sources do nurses working in sheltered housing for older people use when making decisions regarding PRNM?
Materials and methods
This study used a qualitative design. 27 Individual interviews provide a suitable method to describe nurses’ experiences and perceptions. 28 The COREQ checklist 29 was used as a guide in order to enhance comprehensive and explicit reporting on the study. The authors’ professional backgrounds varied, including two pharmacists (first and second authors), and one registered nurse (third author). All had many years of teaching experience from higher education and experience with qualitative research. However, none had clinical experiences from sheltered housing.
Study setting, recruitment and participants
The study setting was sheltered housing in mid- and eastern Norway, in both rural and urban municipalities. The sheltered housing was connected to home care nursing services; however, the availability of the services varied. In some sheltered housing units the residents had frequent visits by nurses; in others, they only came when the resident called for assistance. The sheltered housing units had 10 to 60 residents.
The strategy of recruitment was to reflect the heterogeneity of sheltered housing; large and small units, localized in small and large municipalities and nurses with different lengths of experience and positions. The inclusion criteria were: working as a RN or a NA in sheltered housing for older adults and holds responsibility for medication management. For recruitment, a purposeful and mixed strategy was chosen. 30 Basically, the recruitment included informants with special interest in PRNM, by self-recruitment through social media. However, only two informants were recruited by this strategy, and two additional recruitment strategies were used: advert distribution by heads of units and word of mouth through author networks. This mixed recruitment strategy resulted in six additional nurses volunteering to be interviewed.
Table 1 describes the study participants’ characteristics; eight nurses, all female, with 20 years’ median experience in sheltered housing.
Participant characteristics.
Notes. RN: registered nurse; AN: assistant nurse.
Data collection
An in-depth interview with each informant was performed by the first author between February and May 2019. The informants selected the interview location: seven were conducted at their workplace, and one took place at the researcher’s office.
The first author developed a semi-structured interview guide with themes based on findings from another study 3 and literature on the field. The first interview served as a pilot. Only minor changes to the wording of a few questions were needed, and, accordingly, this initial interview was included in the analysis. After giving information about the project and asking for background information (education, experience, position, size of housing), the informants were asked to talk about their experience with PRNM decisions, and to explain how they made their decisions. Examples from the interview guide were: ‘Think about the last time you administered a PRNM. Can you describe what happened? What happened when a resident expressed a need for a PRNM, up until a decision was made to give, or not to give, the medication?’. Follow-up questions were used to clarify and elaborate on their responses. The interview ended with a focus on nurses’ role in PRNM decision-making. The frame of the interview was the same for all, but the follow-up questions were customized to the responses and insight gathered during the interview, which is genuine in qualitative research. 31
All interviews were conducted by the first author, and only the researcher and informant attended. The interviews lasted between 26 and 54 minutes. The interviews were audio-recorded and transcribed verbatim. To validate the interviews, the informants reviewed their own transcripts.
Data analysis
The analysis was based on qualitative manifest content analysis inspired by Graneheim and Lundman 32 with an abductive approach also called combined analysis.33,34 The abduction uses existing reference structures to find theoretical patterns in an empirical material, 33 moving back and forth between inductive and deductive approach. 34 The analysis was stepwise, and started with all authors reading the transcripts in order to gain a sense of the whole. With a deductive approach, the text was reviewed by the first author in search of meaning units concerning nurses’ knowledge sources that could be sorted into four predetermined categories derived from the EBP Framework:10,11,13 Evaluated external evidence, Stakeholders’ (residents) preferences and values, Practitioner experience and judgement, Context and circumstances. Then, using an inductive approach, the meaning units were condensed, coded and sorted to outline and label the subcategories within each category. All three authors participated in this last inductive step of the analysis process. Table 2 gives an overview of the categorization. For organization, review and analyses, the NVivo 12 Pro for Windows software was used. While first author transcribed all the interviews, all authors were involved in the analysis.
Overview of knowledge sources used by nurses in PRNM decision-making, and resulting subcategories and categories according to evidence-based practice.
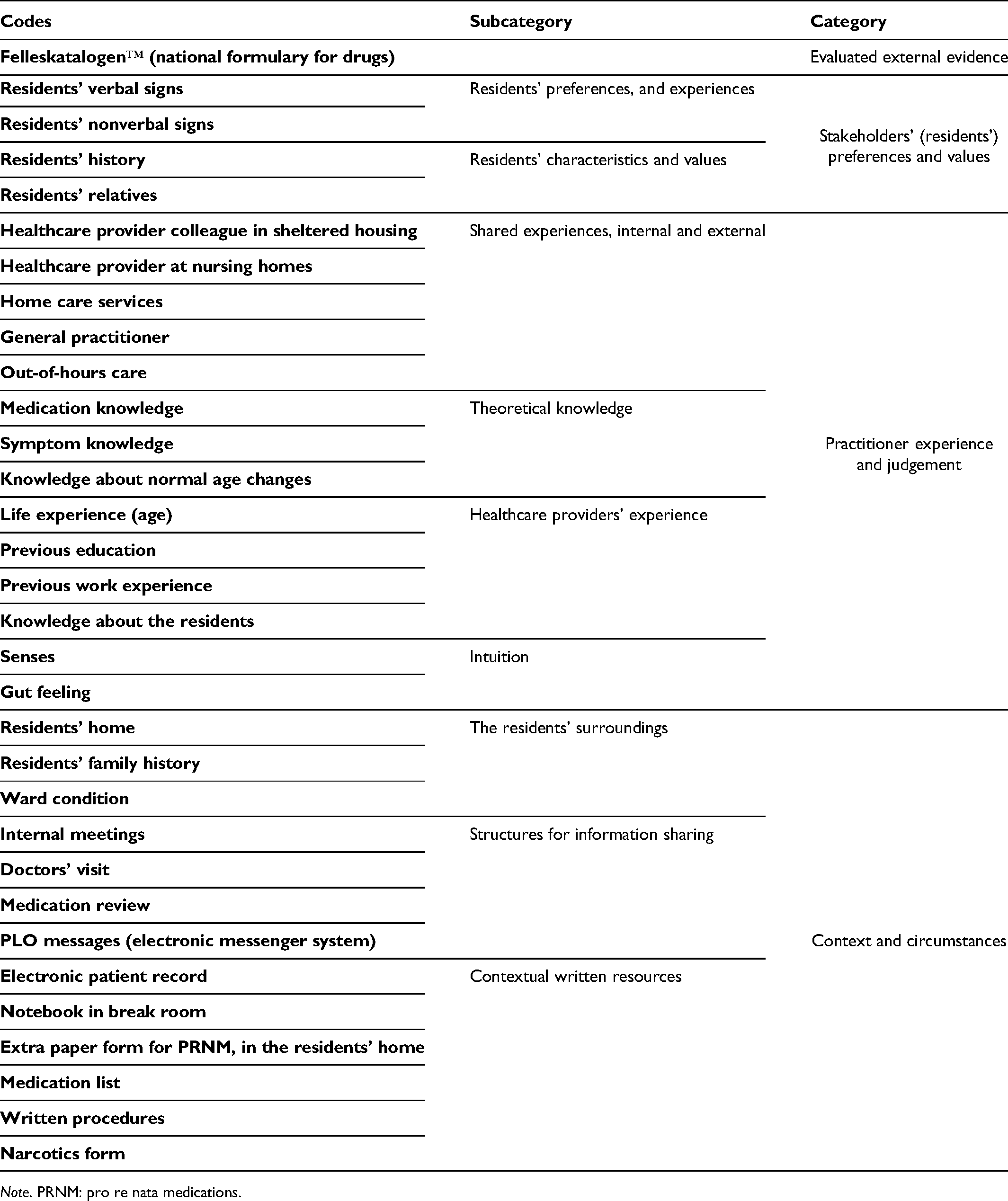
Note. PRNM: pro re nata medications.
Ethical considerations
The study utilized sensitive personal information, and the Norwegian Centre for Research Data (NSD) approved the project (Reference 57803). The ethical principles emphasized in the Declaration of Helsinki were followed. 35 Participation was voluntary, and written informed consent was received from all informants.
Results
Nurses’ use of knowledge sources when making decisions regarding PRNM can be described by four categories and nine subcategories, presented in Table 2. The knowledge sources represent the four elements of EBP, but are used to varying degrees by the nurses. While ‘Practitioner experience and judgement’ was a frequently used source of knowledge, ‘Evaluated external evidence’ was less emphasized in the PRNM decision-making process. The categories and their respective subcategories are presented below, illustrated by quotations from the interview text.
Category: Evaluated external evidence
In the Evaluated external evidence EBP category, one nurse mentioned using a national formulary for drugs (FelleskatalogenTM). ‘I am good at conferring with literature when I feel uncertain. I have to be sure’ (RN, 11 years’ of experience (YOE)). No one referred to research-based evidence.
Category: Residents’ preferences and values
This category represents how the nurses assessed and incorporated the residents’ preferences into the PRNM decision-making process. The category is presented in two subcategories: Residents’ preferences and experiences; Residents’ characteristics and values.
Residents’ preferences and experiences
When making decisions concerning PRNM, having knowledge about the resident’s preferences and experiences, and health status was emphasized by all informants. This knowledge was gathered by reading their history in the electronic patient record (EPR) or by observing them. We can understand the resident’s state through his voice because we know him so well. (…) When he is in pain, he talks in a special way. I observe how he sits and the complexion, this tells me if he is in pain. (NA, 30 YOE)
How well nurses knew the residents influenced this knowledge source, in terms of interpreting health conditions and behaviour patterns. To know the residents well and see them regularly were highlighted as essential for keeping information about the patient up to date. I’m dependent to discuss the case because I’m rarely in the housings. With this resident, it is something new each time I arrive (…) I can’t make the decision on my own, at least not decide if he should have more oxazepam or not. (NA, 2 YOE)
Residents’ characteristics and values
Knowledge about residents’ characteristics was gained through communication with the residents or their relatives. The informants wanted to give the residents’ values a central position in decision-making, but sometimes they tried to convince the resident to take the medicine despite knowing the resident was sceptical. We have a resident now who actually has a lot of pain-related challenges in regard to posture, among others. But his relationship and beliefs about tablets is very strict, and he doesn’t want them, do not want to take painkillers … During the care on Wednesday night, there was a lot of pain and tears. And then I saw that it was there (paracetamol 1
Category: Practitioner experience and judgement
This category represents how nurses utilized their own experience and knowledge in PRNM decision-making, also involving intuition. Furthermore, this category describes decision-making as a collaborative practice, where PRNM decisions are shared among others. The knowledge sources in this category were frequently and broadly referred to by the nurses in this study. Hence, the knowledge sources were apparently highly valued, and were given substantial strength of influence in PRNM decisions. The category is presented in four subcategories: Shared experiences, internal and external; Theoretical knowledge; Healthcare providers’ experience; Intuition.
Shared experiences, internal and external
‘Shared experiences’ was by far the most mentioned knowledge source in this category. Several additional persons, both externally and internally, helped the nurses obtain a broader picture of the situation before administering the medication. Often the providers reached out to those higher up in the decision-making hierarchy, but RNs would also often ask experienced NAs. The practical home care service could bring in important information about the circumstances. We operate individually, that’s why we have a morning and midday report (…) we discuss a lot, also about residents’ experience of pain (…) sometimes the practical home care attend because they spend more time with the resident and observe changes faster. (RN, 19 YOE)
Most of the informants would primarily share experiences internally, in the sheltered housing, but for medical questions, they would contact the GP, out-of-hours care or the nursing home. The disadvantage of using external information resources was their lack of knowledge about the actual situation. If I talk to the nurse at the nursing home, she can give me professional advice, but she doesn’t know the situation and everything that might affect what’s going on. (NA, 13 YOE)
Healthcare providers’ experience
Several informants referred to their own experience, gathered through general life experience, work experience and formal education. Some informants pointed to practical experience being more important regarding decision-making, in comparison to theoretical knowledge. It might be the nurses with long experience rather than newly graduated nurses that read the situation best. (NA, 23 YOE)
Through extensive practical experience, they also acquired a holistic perspective that made them more capable of managing this complex decision-making process: You can’t always follow the book, they are humans, not machines. You must see the whole person (…) It is to be learned gradually, the judgement depends on the situation and who the resident is. (RN, 21 YOE)
Theoretical knowledge
The nurses also used what could be understood as theoretical knowledge, but described this knowledge to be ‘in their minds’. The knowledge seems to be internalized. You have to know the theory to understand what you are doing. (RN, 11 YOE)
Intuition
Some referred to using their senses when judging a situation. Use of gut feeling was also mentioned, and there were situations in which nurses just felt or understood what to do based on their overall experience. It (the judgement) starts when you open the resident’s door (…) You can understand it in the way the resident greets you. (RN, 19 YOE)
Category: Context and circumstances
This category represents the sheltered housing context where the decision-making takes place, and includes knowledge of both organizational features as well as knowledge of the residents’ circumstances. The category is presented in three subcategories: The residents’ surroundings; Structures for information sharing; Contextual written resources.
The residents’ surroundings
The informants gathered information about the residents’ homes: if the home looked like it normally did or whether there were any discrepancies that could provide information on today’s situation. Knowing the residents’ families could be of importance. Information about the ward situation was considered when making decisions, such as staffing, time allotted for each resident or other demanding residents. It has often something to do with time management, having time to talk to residents instead, for example at evening shifts when a resident calls for help at the same time as everybody else, I understand it could be easy to give oxazepam instead, but it doesn’t feel right at all. (RN, 22 YOE)
Structures for information sharing
Structures for information sharing entailed the possibility to exchange information, both verbally and in writing, and was described by all the informants in this study. The nurses preferred to use written procedures if existing. Physical meetings and reports, with other nurses and GPs, were emphasized; some had weekly meetings with the GP, others had no regular contact. Additionally, properly written, available information and time to read and familiarize themselves with the information were valuable. We hope to reintroduce the doctors-visit, the communication now is PLO messages (electronic treatment and care messages) (…) all necessary information is not visible through this system, it is much easier to talk together, we really spend much time sending these messages back and forth. (RN, 19 YOE)
Contextual written resources
In addition to the residents’ EPR, nurses frequently used several written resources they were not obliged to use, e.g. notebooks, to support the PRNM decision-making process. We have a so-called ‘black-book’ (a notebook) where we write messages on things to remember from day to day (…) when I wrote there that we should give feedback to the GP regarding a patient’s use of painkillers, we followed up the PRNM. (RN, 19 YOE)
Discussion
This study found that, in decision-making processes of PRNM, the nurses used several knowledge sources, and utilized EBP to a certain degree. The ‘Practitioner experience and judgement’ was a prominent evidence base that could include internalized knowledge from additional sources of evidence. This emphasizes PRNM decision-making to be a transdisciplinary practice, where ‘Practitioner experience and judgement’ embraces the other evidence bases to a great extent. All EBP elements were used in the decision process, describing how individual nurses interpret information through reasoning patterns alone or in combination. 36
The findings in this study are in line with previous research on nurses’ decision-making.37–41 This study indicates that nurses’ internal and shared experiences are given great weight in PRNM decision-making, which corresponds with previous studies describing practical knowledge in nursing as social interactions, experiences, documentation and prior knowledge,37,38 experience-based knowledge, 39 and the ability to involve the patient. 40 Experience and practical training are important to be able to interpret resident-specific actions. 41
In the EBP model, ‘Evaluated external evidence’ is a central element. 10 However, nurses in this study made little use of this source of knowledge, regardless of education. An integrative review that determined the current state of nurses’ EBP competencies reported on similar results, where the majority of nurses surveyed never used external evidence to inform their practice. Furthermore, the review concluded that large proportions of nurses do not use research or integrate best evidence into daily practice, despite believing the value of EBP in improving quality of care. 14 This study did not clarify whether not using external evidence resulted from a lack of access to information sources or from nurses not considering it necessary. Access to information sources could be solved by introducing easily available resources to aid healthcare providers searching for evidence. One example is the ‘National network of medicines information and pharmacovigilance centres in Norway’ (RELIS). 42 This requires nurses to be aware of the importance of external evidence, and allocate time to use the sources. A practice solely based upon using experience as evidence is problematic, and may result in varying practices of PRNM administration. Accordingly, the use of PRNM medications will be inconsequent and highly varying, and the practice will undermine quality of care.
Patient experience was important for the nurses, which suggests a patient-centred care approach. Knowledge about the residents was important from the time perspective in the decision process, including in post-administration of PRNM to monitor effects and changes in the residents’ health. When nurses or residents are new to the housing, it would affect the PRNM. The importance of knowing the patient is well established.36,43
The context may influence nurses’ decision-making.9,44 In this study, there was an example where ‘Context and circumstances’ and ‘Practitioner experience and judgement’ conflicted regarding the PRNM decision process, and the ‘winner’ was organizational, not professional. Knowing the context had an impact on the decision-making, nurses in this study indicated that lack of personnel could lead to medication administration as a first resort intervention, despite not wanting to do so.
EBP is a foundation for clinical guidelines and is crucial for clinicians to practice the best possible healthcare. The theory is suited for what can be formal and explicit in healthcare practice; however, clinical practice is more complex, and it is impossible to capture every possible reality. 39 The nurses mentioned guidelines, but there are few explicit PRNM guidelines, as described in a systematic review focusing on psychotropic PRNM. 21 Medication management must be individualized and customized to the respective patient situation, and in utilizing EBP to guide decisions, there might be challenges regarding how evidence should be defined and comparatively weighted. 10 Other models for decision-making and clinical reasoning incorporate the process and illustrate the complexity when using different kinds of evidence in the decision-making process.9,36,45
In this study, the use of tacit knowledge or other easily accessible resources was described. The nurses often referred to ‘Practitioner experience and judgement’ as an applied knowledge source, like ‘mindlines’ described by Gabbay and le May. 46 These are internalized, tacit guidelines with a foundation in many sources of knowledge gathered through practice, like clinical wisdom, and are flexible to adjust to individual cases. 47 For the PRNM decision process, it may be appropriate to apply the ‘mindlines’ thinking due to the complexity,5,9 and the connections between all the knowledge elements being processed in nurses’ minds. However, it would be necessary to have more research evidence to determine the nature of ‘mindlines’ thinking in clinical practice.
Shared experiences, both external and internal, were important according to this study. Studies from hospital settings have found that knowledge sharing is positively correlated with patient safety.48,49 A literature review about nurses’ clinical reasoning and medication management found that nurses utilize knowledge about patients and the organization, in combination with clinical reasoning, to support safe medication practice. However, the literature sparsely describes how nurses utilized clinical reasoning to support the correct use of medications. It was unclear whether this led to safe medication management. 50 Nurses in this study described the possibilities to share knowledge about residents and their PRNM, using internalized knowledge and experience and contextual written resources, as a contributor to ensure appropriate and safe medication management; they felt more secure in joint decisions.
Drug-related problems due to unclear documentation are known. 51 The nurses in this study used written resources; often these were informal and not mandatory to use, e.g. a notebook in the breakroom. It has been reported that information exchange between nurses largely occurs through informal means of communication,52–54 and why this occurs should be of concern. Formal systems and guidelines should be up to date, feasible and easily accessible to users, making additional systems such as notebooks unnecessary. Given a suboptimal documentation practice, nurses might find it necessary to trust experience and judgement, which may pose a risk to patient safety.
Strengths and weaknesses
A strength of this study was introducing novel insights about the PRNM management process in sheltered housings. Studies on PRNM management in primary healthcare are in general scarce, and, as far as we know, no one has previously studied PRNM management in sheltered housing. The sampling strategy resulted in the inclusion of nurses with different approaches to PRNM management, since the informants were employed in different municipalities that organized their services differently. Another strength is that the ethical principles of the Declaration of Helsinki 35 were carefully followed during the whole process.
One limitation of this study is the small sample size, which makes it difficult to draw conclusions about the transferability of the findings. For more power, a larger sample size would be preferred. 55 However, the transparency of the data and the research process make it possible for the reader to decide whether or not the findings are transferable to similar situations in other contexts.32,34 Another limitation is that only women participated. On the other hand, this reflects the gender distribution of nurses in sheltered housing. In addition, we succeeded in having variation among the participating nurses, representing different positions, municipalities, experiences and education.
To enhance trustworthiness, 34 informants read and validated their own transcripts. (One of the informants had an additional comment that was of no importance for the analysis.) The analysis was carried out by all three authors.
Conclusions and implications
Despite a relatively small study sample, we found that several different sources of knowledge are used when nurses working in sheltered housing for older people make PRNM decisions. The knowledge sources recognized represent the four elements of EBP, where PRNM administration is a collaborative decision-making process combining the evidence. Furthermore, the strength of influence from the evidence elements varies in PRNM decisions, where the emphasis on nurses’ experience was pronounced compared to ‘Evaluated external evidence’. Prominent knowledge sources mentioned were internalized or personal to the nurses, but also externalized, i.e. a collective experience and judgement gathered through work and life experience.
Due to the fact that PRNM is a significant part of medication management, a clinical implication is that nurses should reflect on how PRNM decisions are made, and assess the possible impact this may have for the residents.
Furthermore, this study has implications on an organizational level, e.g. facilitating structures for information sharing, and ensuring staffing with sufficient experience and knowledge. Revised and updated PRNM guidelines, including documentation practice, and a system for securing the use of collective experiences and including the patient in the PRNM management, are recommended.
Further research is recommended with a larger sample. PRNM management is a complex process, involving several healthcare providers. Thus, extended knowledge on perspectives of all involved actors (residents, leaders, GPs, and other health professionals) should be elaborated in further studies.
Footnotes
Acknowledgment
The authors would like to thank the participants for their kind contributions.
Author contributions
Study design: MKN, HS, and RMO. Data collection: MKN. Data analysis: MKN, HS, and RMO. Manuscript preparation: MKN, HS, and RMO. Critical review of the manuscript: MKN, HS, and RMO. All authors approved the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.