
Abstract
The number of patients with dementia admitted to hospitals is increasing. However, the care and treatment of these patients tends to be suboptimal. A response to this is a widespread implementation of educational initiatives. Nevertheless, the effect of such initiatives is questioned. The aim of this study was to investigate the impact of a dementia education intervention by examining the self-reported outcomes of general hospital staff and exploring the staff’s experiences of these outcomes. An explanatory sequential mixed-methods design framed the study method. The quantitative data collection included repeated questionnaires: pre-intervention (n = 849), one month post-intervention (n = 618), and five months post-intervention (n = 468) followed by a qualitative data collection using interviews (n = 16). The GRAMMS guideline was followed. The integration of the quantitative and qualitative results suggests that the impact of the education intervention can be ascribed to the interdisciplinary focus, which facilitated a comprehensive commitment to creating careful solutions for patients with dementia. A prioritization of person over task seems to be assisted by an improved interdisciplinary cooperation initiated by the inclusion of all employed staff at the hospital in a dementia education intervention.
Keywords
Introduction
To meet the needs of a population with a rising prevalence of dementia, national strategies concerning dementia care and treatment in hospitals advocate for an increased focus on staff education and training.1–5 This focus is requested from different viewpoints: hospital staff experience a lack of knowledge and competencies concerning how to understand dementia, how to manage dementia symptoms, and how to provide person-centered dementia care,6,7 and patients with dementia and their relatives express feelings of stigmatization and dissatisfaction with care and treatment in hospitals.8–12 As a result, dementia-friendly educational initiatives and training programs have been widely implemented in hospital settings in the last few decades. 13
Background
Emerging evidence suggests that staff training in hospitals can improve the knowledge, attitude and competence in dementia care and treatment and can influence person-centered dementia care by facilitating a more individualized approach.14,15 However, the long-term effect of education and training initiatives is unknown since most studies report on their short-term effect.16,17 Some evidence exists concerning the elements that are essential to the successful implementation of dementia educational initiatives in hospital settings. These elements consist of education with minimum duration of one day, tailor made content about dementia, and available dementia experts to support hospital staff in the clinical setting.18,19 Nevertheless, knowledge about the effects of dementia education tends to overlook the complexity of interplaying factors in educational interventions in hospital settings. This complexity involves several issues that go beyond an immediate effect on outcomes such as knowledge scores measured on specific hospital staffing groups.17,19 Knowledge is needed on how learning outcomes translate into clinical settings at the clinical level as well as the organizational level following dementia educational initiatives, and such knowledge is considered to be of high priority in evaluating such initiatives.14,20–22 Similarly, the evidence of the effect of educational initiatives is limited when it comes to the inclusion of interdisciplinary staffing groups, including the ancillary staff.17,19,23,24 Research suggests that the narrow focus on care and therapeutic staffing groups in dementia education interventions will reduce the effect of such interventions because patients with dementia interact with a large variety of staffing groups during hospitalization.21,25 One study that included all hospital staff found that a multidisciplinary education had some effect on the ancillary staffing groups and recommended the inclusion of these groups. 26
The above-reviewed literature reveals a need for evidence on how to best evaluate the effect of dementia education initiatives and the impact of such initiatives on the approach of general hospital staff towards patients with dementia. Furthermore, alternative methodologies to pre-test–post-test analysis are needed when evaluating the long-term effect of dementia education initiatives and the impact on staff behavior towards patients with dementia in complex settings such as hospitals.17,27 Such methodologies could extend our knowledge concerning the perceived effect described by the involved hospital staff and the practical changes resulting from dementia education initiatives. 20 A mixed-methods approach could serve as a way to embrace the complexity in evaluating hospital dementia education interventions by measuring the effect quantitatively and explaining these results by qualitatively exploring the essential elements related to the associated changes following an education intervention. To our knowledge, no studies have examined the long-term effect of a dementia education intervention in hospitals with the inclusion of all staffing groups or within this added knowledge about the experiences of staffing groups regarding the impact of the educational intervention.
Aim
The overall aim of this mixed-methods study was to investigate the impact of a dementia education intervention by examining the self-reported outcomes of general staff and explaining these outcomes by exploring the staff’s experiences.
Research question
How can qualitative interview data, exploring general hospital staff’s experience of the impact of a dementia education intervention, explain the self-reported knowledge, attitude, and competence scores from a quantitative measure?
Method
The philosophical assumptions of pragmatism informed this study. According to pragmatism a rejection of the dichotomy between object and subject is valued, since a complementary approach that acknowledges both objective and subjective knowledge based on what best addresses the aim and research question is respected.28,29 In our study a quantitative approach was needed to provide results that could be further explained by qualitative results. Thus, an explanatory sequential mixed-method design was applied (Figure 1). 30 This mixed-methods approach guided the study, allowing the results from one type of study to broaden and explain the results from another type of study. The quantitative phase aimed to provide an overall picture of the impact of an education intervention on the knowledge, attitude, and competence scores of general hospital staff regarding patients with dementia. These results were connected to the qualitative data collection in order to recruit participants who could elaborate on these results. Further, a connecting point between the quantitative and qualitative methods was the development of the interview guide in the qualitative phase based on the quantitative results showing the overall picture of the impact. Lastly, the quantitative results and the qualitative results were connected and integrated with the aim of explaining through interpretation. 30 During the integration phases, the mixed-methods research question: ‘How can the qualitative interview data help explain the quantitatively self-reported scores?’ served as guidance. The guideline for Good Reporting of A Mixed Methods Study (GRAMMS) was followed in this study. 31
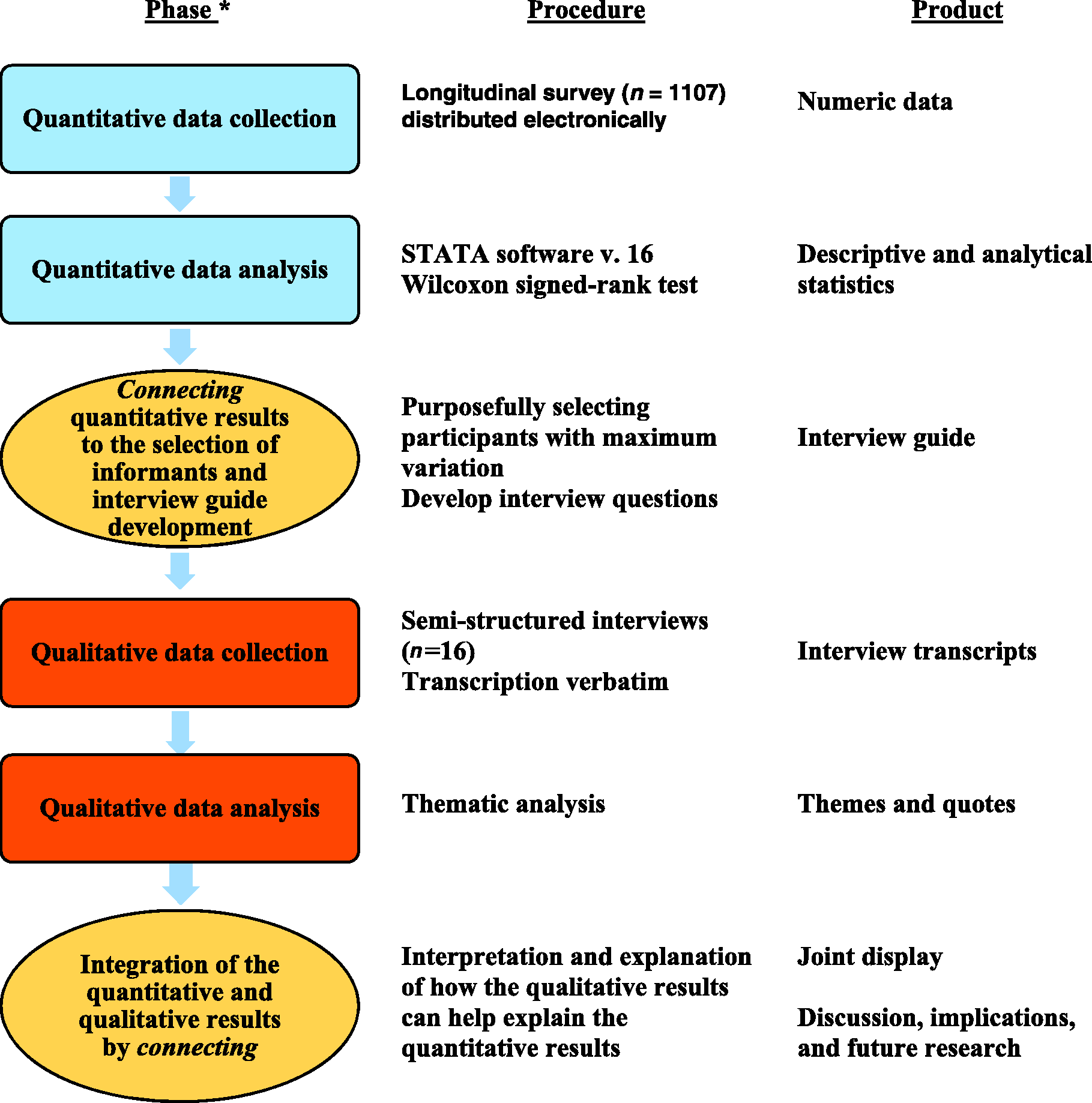
Explanatory sequential design.
Setting
This study took place at a smaller hospital within the University Hospital. The hospital has approximately 1600 employees and represents a broad range of functionalities and diversity of professions. The hospital participated in a national large-scale dementia-friendly hospital project from 2017 to 2019 and implemented a variety of initiatives with the common goal of improving the care and treatment of patients with dementia.
Intervention
The dementia education intervention was inspired by a national plan to develop dementia-friendly hospitals 2 with the aim of improving basic competencies among the entire workforce in a general hospital setting. The improvement of basic competencies and the development of dementia-friendly hospitals serves as guidance to assess the impact of the aim and research question of this study. The intervention consisted of three elements. First, a mandatory e-learning course about patients with dementia in hospital settings to be completed before participation in the one-day course. The e-learning course did not have a limited timeframe, however, when signed up for the one-day course it was possible to access and complete e-learning. The one-day course was conducted in interdisciplinary teams at the hospital from August 2018 to June 2019 and lasted six hours. The content was related to the following topics: dementia – pathophysiology, diagnosis, non-pharmacological treatment, delirium, person-centered care, communication and therapeutic approaches, ethical issues and legislation, staff-specific self-protective skills. Inspired by principles of peer learning, 32 the teaching methods varied and consisted of classroom teaching and interdisciplinary group work in small groups. This approach was suitable given the variation in learning conditions and educational backgrounds among the staff participating in this study. The educators were all related to the dementia-friendly project hospital team and represented geriatricians, nurses and healthcare assistants. Parallel to the course period, problem-based learning sessions (PBL) were initiated in all departments with the aim of translating knowledge from the intervention elements into practice. 33 The PBL sessions were continuously facilitated by educated dementia specialists in all departments with the aim of initiating reflections close to the clinical setting and to identify challenges and jointly suggest future solutions. Though not mandatory, there was a request from the dementia-friendly hospital project team to conduct them regularly with a mix of professions if possible and when the workload allowed. During the education period from August 2018 to June 2019 a total of 878 hospital staff participated in PBL sessions, evenly distributed regarding departments and period.
Quantitative phase
This phase involved examining the impact of the dementia education intervention on the knowledge, attitude and competence scores of the general hospital staff.
Participants
A total of 1107 participants were invited to participate in the quantitative phase. The invited participants included the entire workforce (referred to in this article as general hospital staff) from all departments at the hospital who were signed up for the one-day education course. The invited participants represented nursing staff, physicians, therapists, leaders, service personnel, porters, secretaries, laboratory staff, radiographers, and building and craft workers.
Data collection
A questionnaire was developed and validated by the researchers and healthcare professionals associated with the study. The questionnaire was distributed to all participants by email two weeks before the education day. The email gave information about the study and research ethics including the safeguarding of anonymity and contained a link to the survey. Measures were repeated one month after the answering of the pre-intervention questionnaire and five months after the answering of the one-month post-intervention questionnaire. Data were collected from August 2018 to December 2019.
Questionnaire development and validation in brief
The first draft of the questionnaire was developed from discussions with dementia experts and existing validated questionnaires regarding knowledge, attitude, and competence in dementia care.34–38 These three areas were chosen because of their relatedness since knowledge is suggested to be a predictor of attitude and competence.37,39 To determine face and content validity, we pilot tested the first drafts with the inclusion of participants similar to the target population in the study in a preliminary pilot test (n = 16) and a subsequent pilot test (n = 32), which resulted in a refinement and rewording of items. The pilot tests included interviews and written comments from the participants. The next stage of the validation procedure consisted of a field test with 106 respondents, also similar to the target population of the study. To refine validity, we conducted cognitive interviews with five participants in addition to the distributed field-test questionnaires. 40 This stage aimed at determining the psychometric properties of the instrument and included the assessment of test–retest results through the calculation of intra-class correlation. Further, internal consistency was calculated using Cronbach’s alpha coefficient with acceptable results from 0.68–0.92. This created evidence for inter-correlational components of the scale.41,42 Additionally, floor and ceiling effects were examined43,44 presenting a tendency toward ceiling effects of a few knowledge items. Based on the above-mentioned examinations, necessary revisions were made.
Instrument
The questionnaire included a total of 58 items. A 10-item introduction and demographic section to provide detailed information on respondents including their age, gender, profession, department, seniority and one item regarding previous knowledge about dementia as well as five items regarding education intervention adherence. The outcome variables in the survey were divided into three sections (knowledge, attitude, and competence) and addressed different aspects of dementia, dementia care, and treatment. Knowledge items (n = 16) were assigned a score of 0–27 with one point for each correct answer and were assessed on dichotomy and multiple-choice scales. Knowledge items included e.g. ‘The number of people with dementia is expected to decrease in the future in Denmark’, ‘Dementia is caused by physical changes in the brain’, ‘People with dementia can experience difficulties in expressing themselves in words’. Attitude items (n = 11) included statements with which the participants rated their agreement, such as ‘People with dementia notice if you are kind to them’, ‘It makes no sense to try to communicate with a person with dementia’. Competence items (n = 11) included statements about how well the participants felt that they could manage different tasks e.g. ‘Understand the way people with dementia behave’, ‘Manage challenging behavior from a person with dementia’, and ‘Communicate with a person with dementia who is not able to express herself in words’. Attitude and competence scores were measured on a five-point Likert scale with anchored ratings with possible scores from 1–5 and possible total scores ranging from 11–55 in each section. An overall increase of all items post intervention indicates a positive outcome of the education intervention. Lastly, the questionnaire contained four closing items, e.g. ‘How did you perceive the clarity of the questions’.
Quantitative data analysis
The non-normality of scores and the ordinal scales made non-parametric methods necessary. The guiding research question was: What is the impact of a dementia education initiative on general hospital staff’s knowledge, attitude and competence? The Wilcoxon signed-rank test was used to test differences in median scores of total knowledge, total attitude, and total competence between pre-intervention and one month post-intervention and between pre-intervention and five months post-intervention. Additionally, inter-quartile ranges (IQR) were calculated. P-values less than or equal to 0.05 were considered statistically significant. To detect whether there were any differences between groups, we sorted all professions into groups of authorized and non-authorized health professionals (Law of Authorization). 45 Data were collected and managed using REDCap electronic data capture tools hosted at Odense Patient data Explorative Network (OPEN) 46 and exported to Stata version 16.047 for analysis purposes.
Qualitative phase
This phase had the aim of exploring how general hospital staff experience the impact of the dementia education intervention.
Recruitment and sampling
Purposeful sampling with maximum variation guided the sampling among hospital staff who had completed the one-day education course and the repeated measure survey. Due to the increased workload during the Covid-19 pandemic, two exceptions were made: participants 13 and 16 were dementia specialists who had extensive knowledge about dementia. The maximum variation strategy was determined by the results from the quantitative phase in order to explain the measured effect by including authorized and non-authorized staffing groups, as the demographics and the statistical results indicated the same tendencies in these groups over time. Participants were recruited with the help of dementia specialists and leaders in the departments.
Participants
Invitations to participate in the qualitative phase targeted all staffing groups who had responded to the three repeated questionnaires n = 468. All staffing groups were considered as suitable participants due to the overall aim of the dementia education intervention of improving basic competencies and the quantitative results to be explored.
Qualitative data collection – interviews
Semi-structured in-depth interviews were used as the data collection method as described by Kvale and Brinkmann. 48 An interview guide was developed based on the aim of this mixed-methods study and the results from the first phase in order to elaborate on how general hospital staff experience the impact of the education intervention, including the one-day course, e-learning, and PBL sessions. Introductory interview questions included: ‘Can you tell me about what you have learned about dementia during the education intervention at the hospital?’ and ‘How would you describe your own and the collective approach to patients with dementia before the education intervention compared to after the intervention?’ These questions were followed by more specific questions aimed at collecting data that could help explain the quantitative results. Examples of such questions were: ‘Did you experience an increase in knowledge following your participation in the education intervention?’ followed by questions such as ‘Can you describe in more detail, what facilitated this change?’ The first interview was conducted face to face and the remaining as telephone interviews. The interviews were planned in accordance with workload and variable working hours from March 2020 to May 2020. The duration of the interviews ranged from 14 to 32 minutes. The interviews were audio recorded and transcribed verbatim by the first author.
Qualitative data analysis
The analytical approach to the data was guided by thematic analysis.49,50 The analytical process was non-linear and followed six steps: 1) Familiarization involved the reading and rereading of transcripts to obtain familiarity with the content of data; 2) Generating codes included writing initial codes in the margin in all transcripts; 3) Constructing themes involved the systematic division of codes into themes and the drawing of a preliminary thematic map; 4) Reviewing themes entailed a review of the codes and their alignment to the developed themes; 5) Revising and defining themes included an analytical refinement and adjustment of the definitions; and 6) the sixth step embraced the description of the final analysis and thus, the reporting of results.49,50 The first author conducted steps one to three, and all authors discussed the last steps. Following the explanatory sequential mixed-methods design, the analysis was guided by the results identified in the quantitative phase; 30 thus, the increase in knowledge, the change in attitude and competence informed the analysis. The guiding research question was: How do general hospital staff experience the impact of a dementia education intervention?
Ethical considerations
The ethical considerations were guided by the Helsinki Declaration 51 and approved by the Regional Danish Data Protection Agency (18/14259). All participants were informed about the study and agreed to participate before the data collection. The participants had the opportunity to withdraw at any time upon request.
Results
In the quantitative phase 860 participants from the study sample (n = 1107), consented to take part in the study and 11 participants were excluded at pre-intervention (T0) due to missing data. A total of 849 (77%), 618 (56%) and 468 (42%) responded to questionnaires pre-intervention (T0), one month post-intervention (T1), and five months post-intervention (T2), respectively. The distribution of participants is characterized by a dominance of female hospital staff at all measure times (83.6%, 85.0%, 83.5%). Median age was 48 years at inclusion at T0. The representation from different department sections at the hospital, Surgical, Medical, Para Clinic, and Technical Administrative was equally distributed throughout measures (Table 1).
Participant characteristics (quantitative).
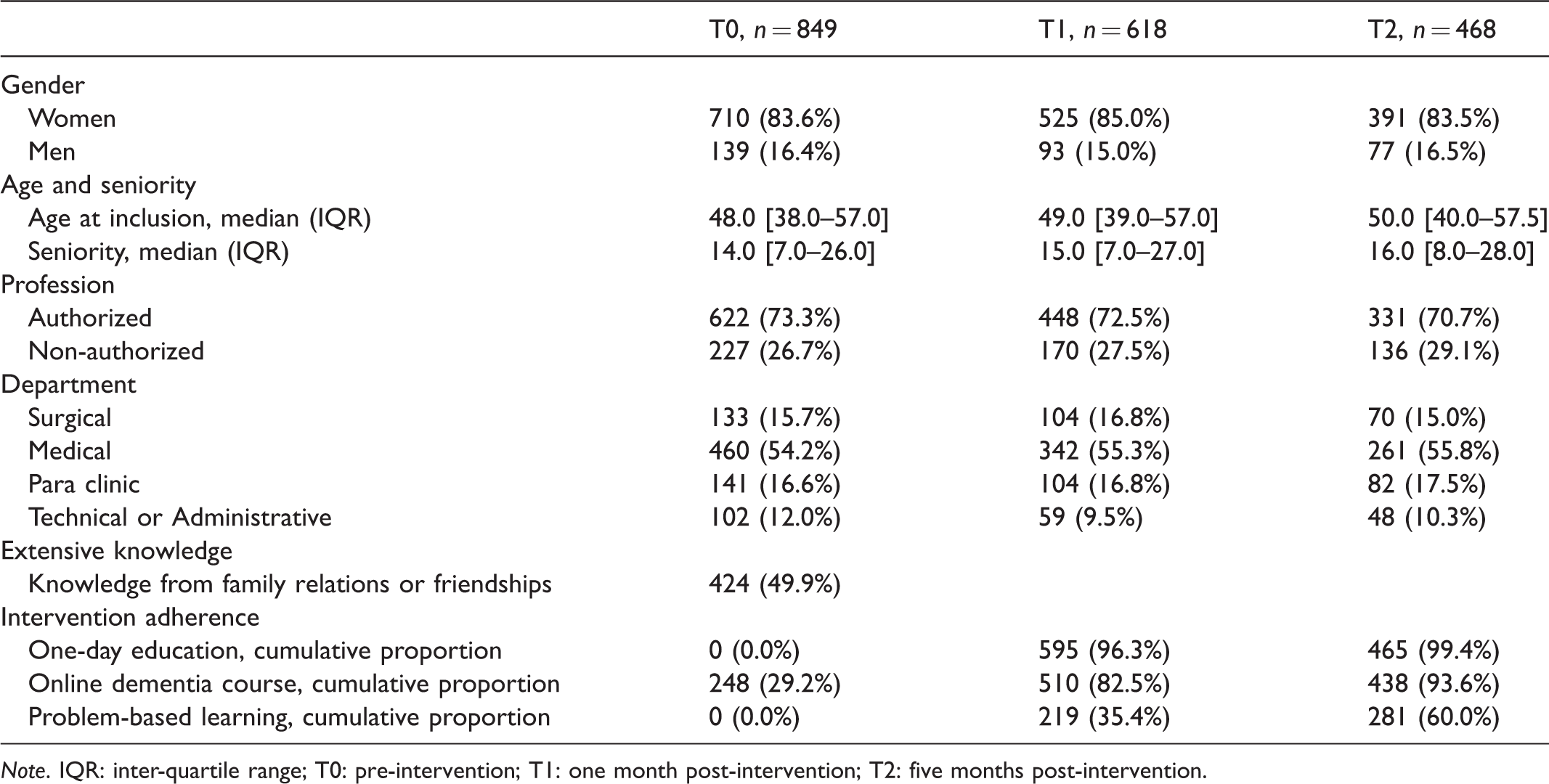
Note. IQR: inter-quartile range; T0: pre-intervention; T1: one month post-intervention; T2: five months post-intervention.
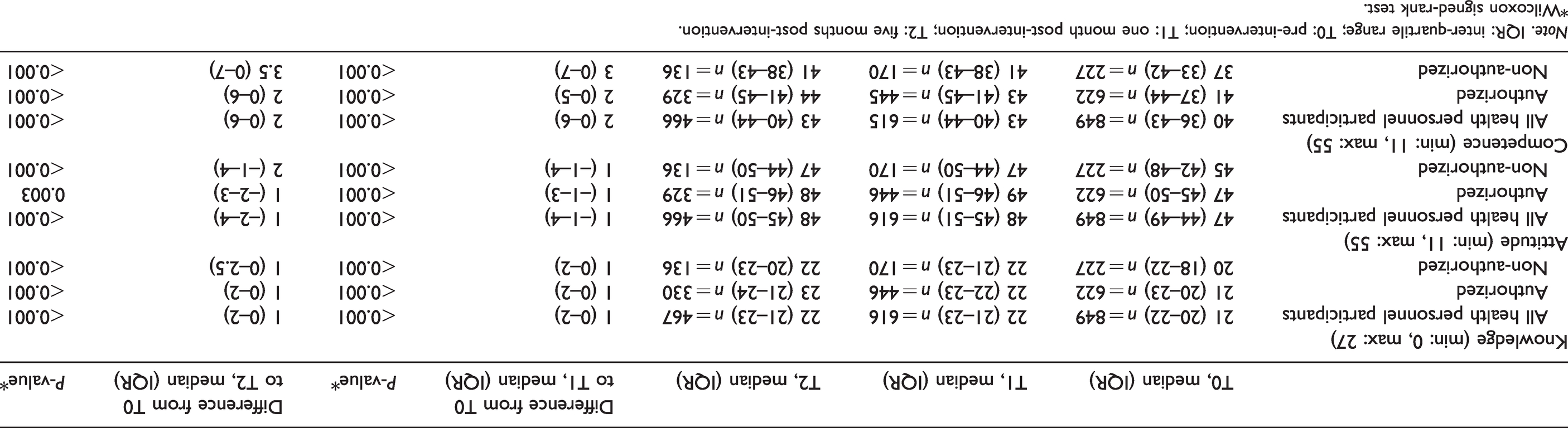
The Wilcoxon signed-rank test revealed that knowledge, attitude, and competence score medians from T0 to T1 and from T0 to T2 increased significantly for all participants following a dementia education intervention. Correspondingly, this picture was applicable in the groups of authorized and non-authorized health personnel (Table 2).
Results (quantitative).
Note. IQR: inter-quartile range; T0: pre-intervention; T1: one month post-intervention; T2: five months post-intervention.
*Wilcoxon signed-rank test.
Knowledge score
The knowledge-score (median (IQR)) at T0, T1, and T2 was 21 [20–22], 22 [21–23], and 22 [21–23], respectively. The score increased 1 point between T0 and T1 (p ≤ 0.001) and 1 point between T0 and T2 (p ≤ 0.001). For authorized health personnel, the score was 21 [20–23] for T1, 22 [22–23] for T2 and 23 [21–24] for T3. The score increased significantly in both groups of authorized and non-authorized health personnel at both time intervals (p ≤ 0.001).
Attitude score
The attitude score (median (IQR)) at T0, T1, and T2 was 47 [44–49], 48 [45–51], and 48 [45–50], respectively. The score increased 1 point between T0 and T1 and 1 point between T0 and T2 (p ≤ 0.001). The score increased significantly for both authorized (p ≤ 0.01) as well as non-authorized (p ≤ 0.001) health personnel at both time intervals. The largest increase was seen for non-authorized health personnel from T0 to T2 (Table 2).
Competence score
The competence score (median (IQR)) at T0, T1, and T2 was 40 [36–43], 43 [40–44], and 43 [40–44], respectively. In the total group the score increased significantly between both time intervals (p ≤ 0.001). For authorized health personnel, the score increased 2 points from T0 to T1 and 2 points from T0 to T2 (p ≤ 0.001). For non-authorized personnel, the increase was 3 points from T0 to T1 and 3.5 points from T0 to T2 (p ≤ 0.001) (Table 2).
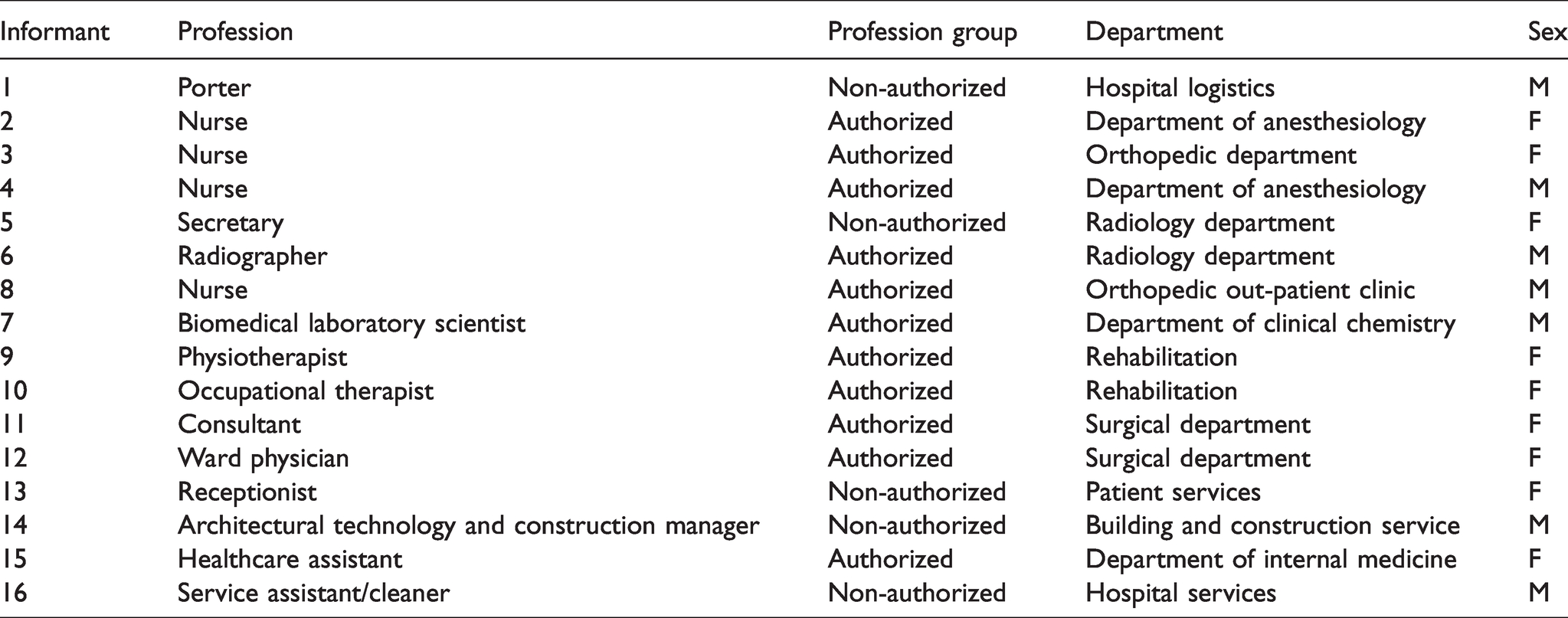
In the qualitative phase a total of 16 participants were included in the qualitative phase represented by nine female and seven male participants. The participants represented the different department sections at the hospital: Surgical, Medical, Para Clinic, and Technical Administrative and represented a wide variety of professions. The participants had a median age of 49 years and a median seniority of 12 years (Table 3).
Participant characteristics (qualitative).
Three themes were developed as a result of the analysis of the qualitative data: cumulative wisdom, inter-occupational cooperation, and shared proficiency. These themes explain and elaborate on the quantitative results and are presented below with example quotations.
Cumulative wisdom
An overall element of the participants’ experiences regarding the effect of increased knowledge and the associated changes was centered on the cumulative effect of all staff having increased knowledge about dementia following the education intervention.
A common point in the participants’ experiences of the knowledge gain was that new or refreshed knowledge contributed to a changed approach to patients with dementia because this new knowledge made them feel more capable of acting and reacting appropriately to the specific requirements called for in situations of patients with dementia. This was described as an individual gain of importance and an invaluable starting point. I really learned something new and I am now acting in a new way in many situations. For example, the thing about singing was new to me. I didn’t know that. (Informant 1) My knowledge has been refreshed, but what is most valuable is that we now have a common frame of reference among the departments. (Informant 2) And what is particularly valuable is that I can contribute when we work together concerning the patient with dementia. Together, we know more. (Informant 7) The shared knowledge base facilitates a moving away from a self-oriented way of working because you are more committed. (Informant 9) You are committed to contributing, now that everyone is part of the education intervention and has gained new knowledge. Then you also have to contribute. (Informant 14)
Inter-occupational cooperation
An overall pattern that was visible in the participants’ experiences of the changed attitude towards patients with dementia following the education intervention was that this change fostered an inter-occupational cooperation that was described as a common ground from which staffing groups could exchange ideas and experiences in a professional fellowship.
Numerous references were made to this overall pattern, which was described as a disseminated underlying value that served as a determining factor for the way these patients were approached. It is a kind of organizational ethos when the values change. I perceive that the attitude toward these patients has changed and that we are approaching them in a new way. (Informant 4) An altered approach to dementia has been disseminated as a result of the inclusion of all staff. (Informant 13) When everyone has learned the same thing, then it changes something and focal point becomes the patient rather than the specific task to be solved. (Informant 6) It has changed something in the way we approach patients on their terms. (Informant 5) Something has changed in the way we now focus on professionalism rather than emotions, and it is caused by the collegial discussion because we now have a common ground. (Informant 10) A common ground has been created. I think that a consistency is guiding the way patients with dementia are approached, no matter what department you are from. (Informant 12)
Shared proficiency
The qualitative data suggest that the dementia education intervention facilitated a shared pathway in the efforts to improve and maintain competencies towards patients with dementia. Keywords in this consistent element in the participants’ experiences were expressed as increased dialogue and helpfulness between staffing groups with the overall aim of approaching the patient with dementia in the most attentive way.
The participants’ experiences included a clear tendency to highlight that the education intervention and the focus that followed implied that dialogues about patients with dementia changed their focus and were initiated before the situation to prevent an escalating situation as well as during and after to learn from a shared experience. There is more dialogue about how to plan and I feel that this is a visible result. (Informant 6) We are helping each other to avoid merely doing the usual routines, but instead observing the individual patient. (Informant 5) The shared interpersonal understanding facilitates cooperation. Professionals from all disciplines are important in dementia care. I think that we are more aware of that throughout the hospital—that we have all committed ourselves to contributing. (Informant 10) Previously, you could feel quite alone with these patients, the rule was kind of ‘it’s my patient so I will try to solve it myself’, but now we are more open to asking for help. Then you can avoid being frustrated and helps to solve things together. (Informant 5) The interdisciplinary approach is absolutely what facilitated changes. When we move in the same direction, things happen. (Informant 12) So, now the hospital is dementia-friendly, but I think that there is a lot more work to be done. (Informant 2)
Integration of quantitative and qualitative results
As an overall result of the integration of quantitative and qualitative results, we illustrate how the significant changes in knowledge, attitude, and competence scores are explained by an improved committed interdisciplinary cooperation around patients with dementia with no differences detected between authorized and non-authorized groups. While the quantitative results provided information about the extent of the impact on scores, the qualitative results confirmed and expanded these results as the integration enhanced an explanatory understanding of the impact of the education intervention. The integrated results are shown in Figure 2 as a joint display illustrating that the phenomenon of interest: the impact of a dementia education intervention in a general hospital setting can be explained in depth by elaborating the interpretation of numbers with the exploration of participants’ views. The feeling of commitment was mentioned throughout the interviews when the participants’ experiences of the impact were explored and identified as a common frame of reference that strengthened the impact of the education intervention. Within this overall framework, the increase in knowledge was described as a synergic effect that is explained by a shared knowledge base valued over individual knowledge. Additionally, the change in attitude and improvement in competence is explained as a facilitation of an emerging comprehensive inter-occupational cooperation that reflected an increased attention to patients with dementia and an awareness of including the person behind the dementia diagnosis. Besides, this awareness included an on-going nurturing of dementia-friendliness.
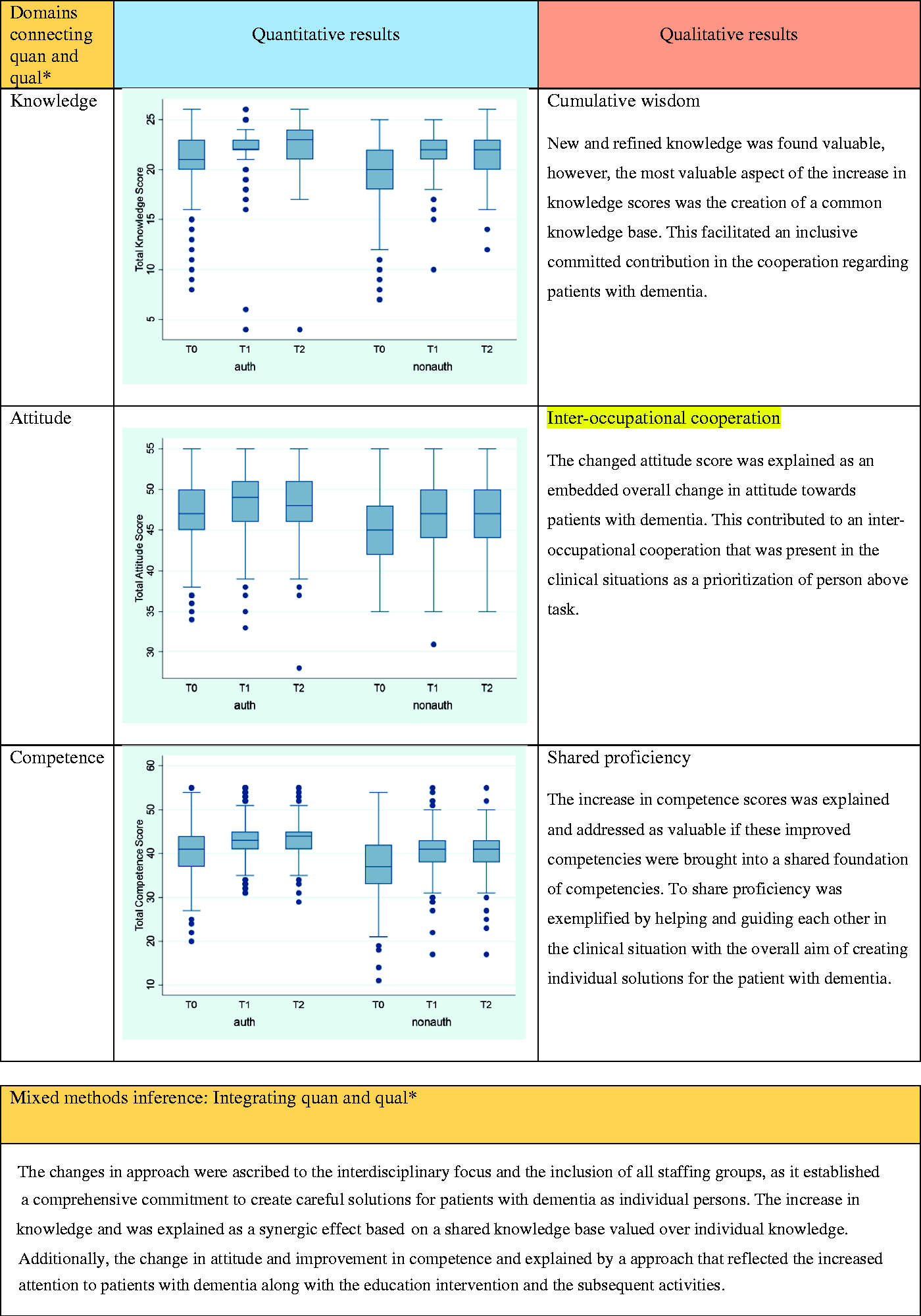
Joint display.
Discussion
Our integrative findings suggest that the impact of a large-scale interdisciplinary education intervention with the inclusion of the entire workforce goes beyond the separate effect on specific outcome measures by adding a new dimension: the consistent change in approach is related to a committed interdisciplinary cooperation. Our results add two notable contributions to the existing knowledge base of dementia education in hospitals:
An interdisciplinary approach with the inclusion of all staff members in dementia education interventions seems to be a prerequisite to creating consistent changes in general hospital settings. The improved interdisciplinary collaboration and overall commitment following a dementia education intervention seem to facilitate a comprehensive focus on person rather than task.
The interdisciplinary focus in education intervention activities was found to play a pivotal role in terms of a changed approach towards patients with dementia in this current study. This universal point was reflected in the explanations of the increased scores and highlighted the joint accomplishment of changes to be more valuable than the individual/personal gain of the educational initiative.
Though some participants in our study explained the increase in scores as an individual gain from the education intervention, the common frame of reference from the education intervention was expressed as more valuable as it facilitated changes in approach to patients with dementia because of the contribution of all involved staff. This is in line with the findings of Brody and Galvin, 23 who argue that if the goal is interprofessional teamwork and the creation of careful solutions for patients with dementia, education initiatives need to be interprofessional rather than parallel training sessions to different staffing groups. 23 This underpins that embedding changes and translating knowledge into the clinical settings go beyond increase in measured scores. Extensively, our results indicate that the interdisciplinary focus was a mediator towards an inclusive learning culture as the contribution of all staff was welcomed and needed if a changed approach was going to succeed. This is further supported in the results of a mixed-methods study examining an education program to improve dementia care and treatment. These results point to team education as an important element in the construction of collaborative teamwork around patients with dementia, and underpin that shared values contribute to changed attitudes and continued improvements in practice. 52 Additionally, the results from a qualitative study stress that training is recommended for maintaining an interdisciplinary focus if a change in practice is to be embedded and dementia care is to be enhanced. 53 Correspondingly, Baillie et al. argue that it is possible to embed a cultural change in dementia care following a dementia education that involves the whole workforce because it facilitates shared experiences across professions. 54
The commitment to improve dementia care and treatment was expressed consistently in the participants’ explanations of the increased scores. This commitment to participate in interdisciplinary cooperation was regarded as a unique result of the education intervention as it assisted the setting aside of professional boundaries and replaced it with a culture of helping, guiding, and reminding each other across occupations and seniority. This additional element of commitment of dementia education interventions in hospital settings is also stressed by Petty et al., 55 who found that dementia care and treatment in hospitals requires the incorporation of different levels of seniority and a variety of professions in dementia education planning. They argue that this will be beneficial due to the exchange of knowledge and experience and stress that that this can facilitate discussions and interdisciplinary reflections about dementia-friendly routines. 55
Our integrated results suggest that the interdisciplinary focus in the dementia education intervention facilitated an improved awareness of the person with dementia. The ability to approach and see the person behind the dementia diagnosis was exemplified as being more empathic in that it aimed at accessing and recognizing the patient’s emotional attitude based on the common foundation of increased outcome scores. Results from a qualitative descriptive study of the term ‘dementia-friendly hospital’ support the importance of this finding, as these results underpin that seeing the person behind the dementia diagnosis is the key element to dementia-friendliness in hospital settings. 56 Seeing the person behind the dementia diagnosis is comparable to the pioneering work of Kitwood 57 and the further development of his work around the philosophy of person-centered care for people with dementia. 58 This work is the constitutive element in recommendations for person-centered care in healthcare settings. 59 However, a review of qualitative studies confirms that even though agreement exists among healthcare professionals that a person-centered approach is the best approach to caring for patients with dementia, the clinical context complicates its execution. 60 The authors stress that the best way to overcome this challenge is to educate using an interdisciplinary approach since education targeted to specific professions makes only a slight difference. Further, a narrow focus on selected professions poses the risk of suspending the opportunity to create an interdisciplinary, person-centered care culture. 60 This supports our finding that the interdisciplinary approach in dementia education intervention can be one key facilitator to improving person-centeredness in hospitals. Thus, our results fill a gap in evidence regarding how person-centered care approaches can be translated into clinical settings as requested by Fazio et al. 59 With a greater focus on the shared responsibility of prioritizing person over task, our results showed that the improved interdisciplinary cooperation enabled increased scores in knowledge, change in attitude, and improvement in competence to be used as assessable resources in a joint reflexivity. Additionally, this shows that to succeed with dementia education interventions in hospital settings, a commitment to an interdisciplinary pathway is a prerequisite to a continued changed approach. Comparable to this, a systematic review indicates that person-centered care interventions in clinical contexts are a promising line for enhancing person-centered care as long as these interventions go beyond one isolated training intervention and add some continued support and the opportunity to discuss dementia care. 61 Additionally, results from a survey study with a focus on person-centered care in hospital settings 7 showed that staff training can improve knowledge and attitude among hospital staff, but that these improvements alone failed to result in increased competencies. The results indicate that education interventions in dementia care and treatment need to have a broad content and focus on both intellectual and attitudinal skills if person-centeredness is to be implemented. 7 This adds support to our findings, which explain the increase in scores with the comprehensive committed cooperation that was manifested following the dementia education intervention as a promising pathway for delivering and jointly nurturing a person-centered approach.
Methodological considerations
An overall strength of our study was the use of a mixed-methods approach. The integration of results from the quantitative and the qualitative phases added a nuanced insight into how the impact of a dementia education intervention can be explained and understood, and it underpinned that the examination of educational effects should be accessed from broadly as requested by Abley et al. 20 Limitations in our study included a lower response rate in post-intervention measures in the quantitative phase, which is also reposted in similar studies.62,63 This serves as a validity threat, since we do not know if these participants represented hospital staff with either high or low scores. However, the homogeneity in respondent groups across measure times compensates for this validity threat. Another limitation concerns the included participants in the qualitative phase, as we included two dementia specialists with extensive knowledge about dementia. This decision could have influenced the qualitative results. However, we did not find that their experiences varied compared to those of the participants who had attended the one-day course. The process by which participants were recruited to the qualitative phase adds some further limitations to our study since the use of gatekeepers can result in participant selection bias. The data collection methods also revealed some additional considerations to be elaborated. The quantitative instrument was not able to detect whether there were associations between knowledge, attitude, and competence scores, which could add useful knowledge about how learning outcome was perceived. Moreover, the questionnaire showed some limitations concerning ceiling effects in the validation process. The quantitative results could be influenced if the participants were limited in response options, which might explain the equality of results at T1 and T2. Additionally, the fact that other dementia-friendly initiatives were implemented concurrently with the education intervention may have affected the results. However, the mixed-methods approach provided an opportunity to go beyond the ceiling effect with the addition of explanation in the qualitative phase. Moreover, the use of telephone interviews in the qualitative phase requires some additional consideration since this approach could result in the omission of contextual and non-verbal elements in the interview situation. 64
Conclusion and implications
The results of this mixed-methods study demonstrated that dementia education interventions can facilitate improvements in knowledge, attitude and competence scores of general hospital staff. However, these improvements do not necessarily lead to changes in approach to patients with dementia. The impact of changes in approach to patients with dementia can be determined by the inclusion of the whole workforce in educational initiatives as this facilitates a comprehensive commitment to interdisciplinary cooperation with regard to person-centeredness.
Our study adds some future implications for practice concerning dementia education interventions in hospital settings. Interdisciplinary education that focuses on scholastic learning outcomes and practice learning is needed, as this approach includes the creation of a common knowledge base as a foundation for acknowledging the contribution of all staffing groups in dementia care and treatment. Further, our study results recommend that dementia education interventions be implemented throughout all hospital departments as this makes the embedding of changes possible.
Our results indicate that there is probably no additional long-term effect of the education intervention on knowledge, attitude, and competence scores comparing median scores at T1 and T2 for all health personnel; however, the qualitative results suggest an embedded impact. Future research is required regarding the sustainable effects of large-scale dementia education interventions. Such research could be conducted as an observational study to explore whether interdisciplinary cooperation is maintained and how the person-centeredness is implemented. In addition, the perspectives of patients and relatives on the effect of educational initiatives are required in future research to ensure that important users are included in the descriptions of dementia-friendly person-centeredness.