
Abstract
Objective:
The goal of this study was to provide a greater understanding of physical activity in patients with early rheumatoid arthritis. The aim was twofold: first to explore if physical activity was associated with factors in the clinical picture of rheumatoid arthritis in this patient group, and second, to explore factors influencing physical activity in patients with early rheumatoid arthritis.
Methods:
A total of 66 patients with early rheumatoid arthritis were included in the study. A sequential explanatory mixed-methods design was used, where quantitative data from a questionnaire were analysed with Mann–Whitney, post hoc Kruskal–Wallis and χ2 test in order to detect differences between groups, and find possible associations between physical activity and independent variables, such as disease activity, health-related quality of life and physical function. Qualitative data were collected in a follow-up questionnaire with open-ended questions that focused on factors influencing physical activity.
Results:
Associations between physical activity, disease activity and health-related quality of life were seen in patients with early rheumatoid arthritis together with strong negative correlations between physical activity and physical function. Patients on sick leave showed the strongest associations between disease-related variables and lower levels of physical activity. The findings from the qualitative analysis showed that physical limitations, awareness as a motivational factor and external environment factors influenced physical activity in patients with early rheumatoid arthritis.
Conclusion:
The results showed a complex underlying motive where physical, psychological and environmental factors influenced the physical activity in patients with early rheumatoid arthritis. In order to provide more effective health interventions, it is important to consider the complex nature of practicing physical activity, where a person-centred approach should be considered. Factors such as physical limitations, economic aspects and time for practicing physical activity should be included in the person-centred approach.
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease that affects 0.7%–1% of the population globally. 1 The early stages of RA – early RA can be defined as 12 months after symptom onset. 2 The incidence is estimated to be between 25 and 50 new cases per 100,000 individuals and years. A combination of autoimmune reactions, genetics and the environment is believed to be the cause of RA, but the precise aetiology is still unknown. 3 The disease involves chronic polyarthritis for the patient, implicating risk of bone and cartilage destruction. The most common symptom of RA is chronic pain, which, however, varies in intensity, localization and quality due to the disease’s relapses and bouts. Apart from the main symptom of pain, the clinical picture of RA also comprises other physical symptoms such as joint swelling, stiffness and tenderness. 1 Mental and physical fatigue are also seen as contributing to the clinical picture. 4 These components may affect, inter alia, the patients’ physical function, 5 as well as the patients’ physical activity (PA) habits. 6
The benefits of practicing PA for the state of RA have previously been reported to include enhanced physical function, improved medical outcomes in patients 7 and increased ability in independently performing physical movement. 8 Due to reductions in other symptoms such as muscle loss, fatigue and pain, PA is thought to be an important element in the treatment strategy of RA in order to prevent these clinical outcomes.9,10 Accordingly, PA helps the patient tackle the development and management of RA symptoms regardless of age. 11 There are evidence-based guidelines for PA in patients with early and established RA. 12 The recommendations for management of early RA are early management, including both pharmaceutical and non-pharmaceutical treatments. 13 Furthermore, patients with RA can also follow the general recommendations regarding PA for the purpose of preventing and controlling the disease and maintaining overall health together with preventing disease-related cardiovascular issues. 14
The mechanisms behind these positive effects of bodily movement and exercise are not fully understood. One hypothesis suggests that PA (especially aerobic exercise) activates the parasympathetic system thus inhibiting inflammation. 15 Other theories propose that PA increases hormone production, thus having a positive impact on the immune system. PA has, however, been shown to be associated with reduced levels of inflammatory proteins such as tumour necrosis factor (TNF)-α in patients with several chronic diseases, and this mechanism has also been suggested as underlying the positive effects in RA.13,16 PA can also counteract RA cachexia by reducing overweight, gaining muscle mass 17 and by reducing levels of TNF-α since this cytokine induces cachexia and thereby muscle loss. 12 Fatigue and pain, together with other physical and mental symptoms of the disease, might also underlie physical inactivity.6,18 PA is shown to improve pain and fatigue and could be a complement to medical treatment.7,12,18
Previous research also examines whether fear and avoidance might underlie the reduced PA in patients with RA, suggesting that symptoms of the disease may be the reason for pain-related fear. These findings suggest that increased disease activity, mirroring increased pain intensity and intensified damage, suffering and impaired physical function, correlate with more pronounced beliefs regarding fear and avoidance in addition to PA. This occurrence is in many cases directly linked to the increased prevalence of tender or swollen joints. 19 In fact, reducing disease activity by performing PA is not only beneficial for reducing the symptoms but also reduces the risk of poor mental health that is present in moderate-to-severe levels in 42% of adult patients with RA. 20 The importance of reducing the disease activity and symptoms in RA patients thus concerns more than just improved physical outcomes, since it has been shown that fatigue, pain and physical impairment are predictive factors for poorer mental health 21 and anxiety 22 in patients with RA.
In terms of the symptoms of RA, PA maintains the flexibility of the joints, improves the balance of the patient, 7 increases the muscle mass and inhibits joint pain. Most patients who practice PA experience these gains, leading to improved physical, 7 emotional and psychological well-being. 20 When applying guidelines for PA on patients, benefits could be gained from applying more tailored solutions to each unique case.7,23 Healthcare providers appear to have paid attention to the role of bodily movement in addition to the disease 24 with reference to the known benefits of PA regarding the clinical picture of RA. However, patients with RA perform relatively low levels of PA in comparison to the general population in spite of the many benefits of practicing PA.24,25 The purpose of this study was thus twofold: first to explore if PA was associated with factors included in the clinical picture of RA in patients with early RA, and second, to explore factors influencing PA in patients with early RA.
Methods
Design
A mixed-methods sequential explanatory design with an inductive approach was conducted in order to gain a greater understanding of interactions between PA and variables such as pain and physical function. The method was used since both quantitative and qualitative methods can provide a complimentary and enriching linking process between the approaches. 26 Integrating both quantitative and qualitative methods can compensate for the potential weaknesses of the two in order to achieve an effective methodology 26 that includes triangulation as part of the process. 27 In this cross-sectional study, quantitative data were analysed for the purpose of finding a relationship between the dependent variable PA, defined as moderate-to-vigorous physical activity (MVPA), and the independent variables described in the data collection. In line with the mixed-methods sequential explanatory design, qualitative data were also collected in order to generate results that provide a greater understanding. 28 The initial quantitative phase and its statistical results provided a general understanding of the research area and formed the basis of the investigation. In the follow-up, open-ended questions were formulated based on the quantitative results. 26 This qualitative data were analysed with a manifest qualitative content analysis,29,30 with the aim of gaining a greater understanding of which factors influence PA in patients with early RA, and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) 32-item checklist in online supplementary file. 31
Patients
A total of 66 patients, 30 men and 36 women with a mean age of 63 (25–90) years, were consecutively included in this study when diagnosed with RA, matching the definition of early RA. All the patients attended a rheumatology clinic in the southwest of Sweden. The patients fulfilled Rheumatoid Arthritis Classification criteria ACR (American College of Rheumatology) 1987 32 and/or the ACR/EULAR (American College of Rheumatology/European League Against Rheumatism). 33
Data collection
Quantitative phase – clinical measurement at inclusion
The clinical measurements were collected at inclusion (July 2014–December 2017), and a basic anamnesis was recorded at the first medical appointment. Disease activity was measured by the composite index Disease Activity Score, calculated on 28 joints (DAS28). 34 This composite index includes the number of swollen joint counts (SJCs), number of tender joint counts (TJCs), patient’s global assessment of global health (PatGA) measured on a visual analogue scale (VAS; range of 0–100 mm, best to worse), erythrocyte sedimentation rate (ESR, mm/h) or C-reactive protein (CRP) scores.DAS28 is a validated index of the disease activity of RA. 34 DAS28 was calculated by the formula ((0.56 × sqrt(TJC) + 0.28 × sqrt(SJC) + 0.70 × Ln(ESR)) + 0.014 × PatGA). Pain and fatigue were measured by VAS (0–100 mm, best to worse). Physical function limitation was assessed using the self-administered and disease-specific Swedish version 32 of the validated Stanford Health Assessment Questionnaire (HAQ) (0–3, best to worse). 35 ESR was analysed by the Westergren method, and CRP, rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA) were measured according to the current laboratory standards at the hospital. Health-related quality of life was assessed by EuroQol-5 dimensions (EQ-5D; range of 1–0.594, best to worse),36,37 a standardized self-assessment scale for health status developed by the EuroQol Group. The EQ-5D serves as a general measure of health for use in clinical and health-economic contexts.36,37 At the inclusion stage of the study, a questionnaire including questions about PA was sent to each participant. PA was defined as MVPA. PA was assessed with two questions concerning the frequency and duration during the previous 7 days (min/week) that participants engaged in: (1) vigorous intensity (jogging or intense exercise) and (2) moderate intensity (walking, gardening or cycling). Patients were dichotomized as being active on recommended levels of MVPA (MVPArec; physically active on a moderate level ⩾150 min/week (moderate physical activity (MPA)) or on an intense/vigorous level ⩾75 min/week (vigorous physical activity (VPA)) or not (sedentary)). 12 Body mass index (BMI) and sick leave were self-reported.
Qualitative phase
An additional second postal questionnaire was sent in December 2017. Based on the qualitative methodology of this study, this questionnaire included four open-ended questions concerning PA and factors influencing PA in patients with early RA. The content of these questions has been formulated from the results of the first questionnaire since MVPA exhibited correlations with disease activity, physical function and health-related quality of life. Associations between factors of the clinical picture of RA and PA have been confirmed in previous studies,4,6 and the open-ended questions were thus: How do you feel that you have changed your physical activity since you were diagnosed with RA?, What influences your ability to be physically active?, What makes it difficult for you to be physically active? and What could motivate you to change your physical activity?
Data analysis
Statistical analysis
The data analysis was performed in IBM SPSS version 24 for Windows. All significance tests were two-tailed and conducted at the 0.05 significance level. The patients were grouped into three groups reflecting the patient’s occupation: working, on sick leave and retired. A Shapiro–Wilk’s test was conducted, which showed that the data were not normally distributed, p < 0.05. Mann–Whitney, post hoc Kruskal–Wallis and a χ2 test were thus performed in order to detect differences between groups. Spearman’s rho was used for calculating correlations between variables (the dependent variable PA compared to the independent variables disease activity measured by DAS28 (TJC, SJC and PatGA), self-reported health measured by EQ-5D, Pain VAS, Fatigue VAS and physical function measured by HAQ) by observing the total number of ranked observations in the groups.
Qualitative content analysis
Qualitative content analysis was used, and the manifest content (what the text says) was analysed in accordance with Graneheim and Lundman. 29 In the analysis process, the intention was to remain close to the text, preserve contextual meanings, and move between the whole and the parts.29,30 The analysis was performed by the main author (M.Q.) and the last author (I.L.) acted as a co-assessor. The entire text (unit of analysis) was read through repeatedly in order to create a general overview of the text as well as its overall central themes. Relevant sentences or phrases were identified, forming 53 meaning units that were based on the aim of the study. This was done in order to highlight the content of the phrases with the intention of remaining close to the text and the very meaning of the statements. In the next stage, the condensed meaning units were shortened and labelled with codes in a further abstraction of the phrases. The analogous codes were then grouped into different categories reflecting the key content of the original phrases. Three categories were identified representing the most fundamental expressions of the patients’ perceptions.29,30
Ethical considerations
The study followed research ethical guidelines according to the Helsinki Declaration including autonomy, beneficence, non-maleficence and justice. It fulfilled the four research requirements of information, consent, confidentiality and safety of the participants. 38 Ethical approval was obtained from the Regional Ethical Review Board at Lund University, Sweden (LU 2012/604). Informed and written consent was obtained from all the participants.
Results
Quantitative phase
Descriptive statistics
A total of 43 of 66 patients (response rate 65%) responded to the first questionnaire and were included in this study. There were no statistically significant differences between responders and non-responders in terms of age, gender distribution, sick leave or any clinical parameter (data not shown).
General descriptive statistics of the included patients at inclusion are presented in Table 1. The patients were divided into three groups: those who worked, were on sick leave and retired. The median age (min–max) of the participants was 63 (29–90) years. The only statistically significant difference between the groups was between the retirees and those on sick leave, where the retirees had fewer TJCs than those on sick leave 3 (0–10) versus 9 (2–18), p = 0.024.
Patient characteristics by occupation at inclusion (n = 43).
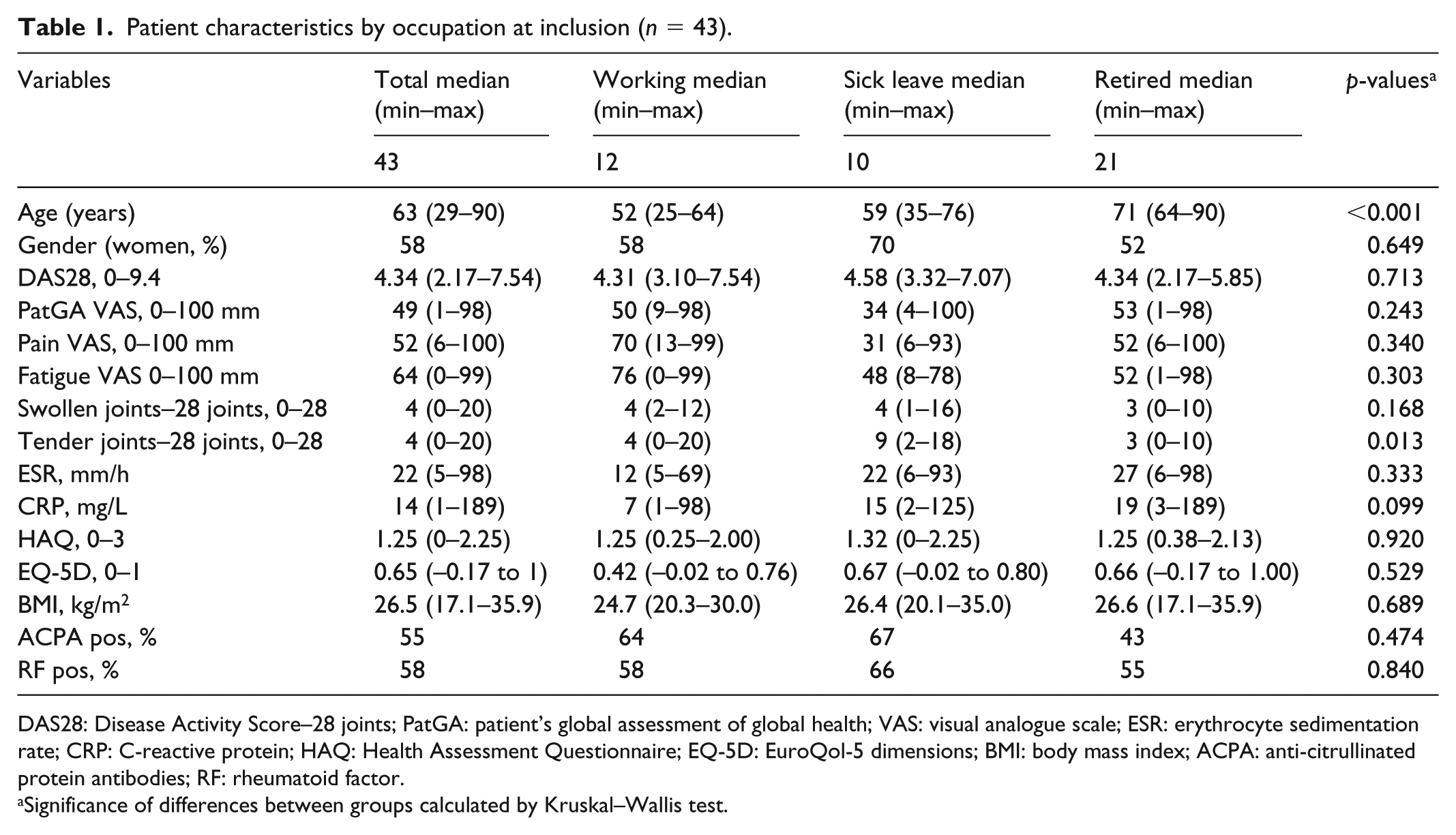
DAS28: Disease Activity Score–28 joints; PatGA: patient’s global assessment of global health; VAS: visual analogue scale; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; HAQ: Health Assessment Questionnaire; EQ-5D: EuroQol-5 dimensions; BMI: body mass index; ACPA: anti-citrullinated protein antibodies; RF: rheumatoid factor.
Significance of differences between groups calculated by Kruskal–Wallis test.
A total of 64% met the recommendations regarding PA, defined as MVPA. The retirees met the suggested criteria regarding weekly MVPA to a greater extent than the others, 86% versus 40% in those with sick leave and 42% in workers, p = 0.010. VPA criteria were met by 33% of the retired patients, 22% of the patients with sick leave and 17% of the workers, p = 0.551. More than 50% of those on sick leave and among the working patients were considered to be sedentary.
Associations between variables
Table 2 presents the correlations between the variables. DAS28 was associated with physical function measured by HAQ in all groups. Disease activity assessed by DAS28 was associated with health-related quality of life (EQ-5D) in all the groups, with a strong correlation in workers and in the retired patients and a moderately negative correlation in patients with sick leave.
Correlations between disease activity (DAS28), physical function (HAQ), health-related quality of life (EQ-5D), meeting criteria for physical activity (MVPA), pain, swollen joint count (SJC) and tender joint count (TJC).

DAS28: Disease Activity Score–28 joints; HAQ: Health Assessment Questionnaire; EQ-5D: EuroQol-5 dimensions; MVPA: moderate-to-vigorous physical activity.
Associations with PA
Overall, MVPA was associated with DAS28, TJC, HAQ and EQ-5D. However, when analysing the separate groups, this association was only found in the group of patients on sick leave. In this group, DAS28, pain and TJC were associated with MVPA (Table 2). No other statistically significant associations were found.
Qualitative phase
A total of 17 patients (response rate 40%), median age (min–max) of 69 (37–82) years, responded to the questionnaire with the open-ended questions about factors influencing PA in patients with early RA
Factors influencing PA in patients with early RA
The qualitative analysis provided a greater understanding of factors influencing PA in patients with early RA. The factors that emerged in the three categories were physical limitations, awareness as motivation and external environment.
Physical limitations
Physical limitations emerged as a barrier to performing PA. One of these limitations was pain, which inhibited the possibilities of being physically active in patients with early RA. The pain was identified as having a negative impact on possibilities for PA, as well as influencing the ability to perform PA in a more vigorous way: Running gives me a pain in my back and my calves get too strained. (No. 7)
Although the patients performed daily activities, they reported that the physical limitation as a consequence of pain seemed to influence their ability to be physically active, when PA was defined as everyday duties that, for example, included heavy lifting. These types of movements were affected due to perceived pain: I can’t manage to lift heavy things anymore. (No. 6)
The patients also expressed that pain and tender joints forced them to change their patterns of PA since these were barriers to PA. For example, the ability to go on long walks outdoors was reduced due to fatigue and tender joints: I can’t walk any further than three kilometers. Then I get very tired and my joints hurt [. . .] I often take the lift instead of climbing the stairs. (No. 6)
Changes in PA occurred as a consequence of impaired physical function due to reduced strength and increased fatigue that occurred after the diagnosis. Patients experienced having limited strength in their hands and could more easily drop things, which thus resulted in them avoiding carrying heavier objects. Climbing on stools or ladders during household activities or gardening was ruled out, due to stiffness and insecurity. The patients also mentioned that the impairing factors influenced their ability to function as they had done prior to the diagnosis. A loss of strength as a consequence of reduced mobility due to the disease was thought to influence the ability to perform PA as the reduced mobility served as a barrier to bodily movement: I felt I had less strength in my wrists [. . .] it still hurts a bit. (No. 15)
Another aspect related to reduced PA was impaired physical function due to stiffness. The patients experienced changes in the general pattern of their PA habits mostly due to having to adapt to the disease, as their physical function was limited. For example, physical activities could take place as a part of a more adapted regimen where physiotherapy and more precise physical movements of rigid joints could constitute the exercise. The experience of stiffness influencing their bodily functions, and thus their possibilities for being physically active, indicates that the patients were defining stiffness as one of the barriers to PA. When exploring what factors could influence the patients to change their PA, the results primarily highlighted having reduced pain and reduced stiffness together with improved physical function: If I wasn’t feeling any stiffness or pain, I would have been much more active. (No. 4)
The physical limitation itself was a barrier to performing PA, which also appeared to influence the PA. Patients felt restricted when performing PA due to the physical limitations caused by fatigue. The patients felt they were impaired in their physical function when exercising, but wished they were well enough to be able to carry out their favourite activities or sports: To not be troubled and be able to run and play ball games. (No. 7)
Awareness as motivation
When the patients explored what could motivate a changed behaviour in terms of their PA, they gained an awareness of which types of PA were good for them. This awareness appeared to function as motivation for performing PA and changing the patterns of PA: If I get to know that a certain physical activity can help. (No. 9)
The motivational factors in this context also appeared to have an impact on the patients’ perspective on their bodily movement in general, since a new awareness of the benefits for PA in terms of overall health was seen as a motivating factor: Factors that affect one positively are the knowledge that the exercise benefits one’s general health. (No. 9)
The results also show that an awareness of the consequences of not performing exercise can motivate the patients to perform PA, for example, an awareness about what impact PA would have on symptoms such as pain was mentioned: I’m mindful about attending exercise classes as I can feel it when I’ve missed one [. . .] then I get stiffer and experience more pain. (No. 13)
Patients also mentioned that exercise and bodily movements had to be adjusted to this awareness. For example, patients had to change the type of PA they performed from a type of exercise that demanded a lot from their bodies to one that was easier and gentler: I have become more cautious with hard training. (No. 4)
Furthermore, fear and caution, due to tenderness and fatigue, were expressed as factors that reduced their ability to perform PA. The patients also stated fear of being injured when performing PA. Fear of movement could influence the motivation to be physically active. These factors could motivate the patients to change their patterns of PA towards a stricter or toned-down exercise regimen. Fear and caution as awareness-related factors were thus mentioned in relation to why the patients reduced their PA and bodily movement: [precautionary behaviour at the gym; the patient felt forced to choose lesser weights when lifting] ‘a bit scared of getting hurt [. . .] my wrists are only on up to 80-90%’. (No. 15)
Another patient mentioned changes in PA due to an awareness of the need for precaution. This appeared to have a motivating effect on the performance of PA, where the patient had found a different way of engaging in exercise since the diagnosis had been confirmed: I do different moves than I did before. I’ve started aqua aerobics. (No. 16)
External environment
Patients’ described the climate as an external environmental aspect influencing PA, for example, nice weather that made it easier to engage in PA. Good weather appeared to have a mitigating effect on joint stiffness and tenderness and thus stimulated the performance of PA: Nice weather is stimulating [. . .] thunderstorms affect my exercising negatively [. . .] since the problems in my joints are affected by the weather. (No. 9)
The mode of transport to the shops or the training facility was discussed as another aspect of the external environment. The patients cycled or walked to their activities as much as the weather allowed them to. Although in poorer weather, shorter walks and more sedentary behaviour was common. Sedentary behaviour also appeared to increase due to seasonal changes when it became darker and colder during the autumn and winter, thus constituting factors of the external environment that hindered the performance of PA. Travelling abroad to a warmer climate could influence PA in a positive way: Trips to warmer countries during the spring, autumn and winter [. . .] I feel that my rheumatic problems are almost unnoticeable then. (No. 8)
Another external environmental aspect that is related to the individual’s personal economy served as a barrier to performing PA since a limited economy appeared to influence the possibilities of engaging in PA. Financial support, such as preferential agreements with the healthcare services or training subsidized by an association, was considered to be necessary for performing PA. The financial support eased the economic burden and made it possible for the patients to exercise for a reduced sum, which served as a motivator for performing PA. There was also an expressed desire to start to participate in water aerobics, but geographical and logistic restrictions constituted a barrier to performing PA, by limiting their ability to engage in these kinds of activities. The patients also mentioned the time needed due to the diagnosis and their working hours as a factor that impacted on their ability to be physically active: Would have gone training a lot more if I hadn’t worked. My day off is dedicated to medical appointments. (No. 11)
Discussion
This study aimed to explore possible associations between PA and factors included in the clinical picture of RA, such as disease activity, self-reported health, physical function and experienced pain. The study furthermore aimed to explore which factors influenced PA in patients with early RA. The findings from this study show important factors concerning the patterns of PA in patients with early RA. This study’s mixed-methods design, through which a multi-perspective of the patients’ perceptions is gained, provides the research field with empirical insights from both qualitative and quantitative data.
Physical limitation-related factors, such as pain together with stiffness and tenderness that are included in the clinical picture of RA, influence PA in patients with early RA. The results of this study indicate pain and stiffness, as related to impaired physical function, constitute a barrier to engage in PA, which also has been reported in other studies. 39 This is the case when PA is defined both as daily activities, that, for example, include heavy lifting and PA as a more vigorous activity.7,39,40 It has been found in earlier studies that patients frequently rate the disease burden of pain as one of the top priorities in terms of the physical limitations seen in RA. Pain has also been found to relate to reduced well-being in general in patients with RA41,42 and is also related to a poorer emotional and physiological health, including health parameters such as sleep habits, functionality in everyday life and the emotional status over time. 42
This study also shows that many patients did not achieve the recommended levels of PA. More than half (58% and 60%) of the two subgroups of patients, those working and those on sick leave, failed to comply with the recommendations for healthy PA patterns (MVPA). The retirees met the recommendations to a greater extent, where 86% of this subgroup met the recommendation. The results of this study thus support previous findings of generally low PA levels among persons with RA,24,25,43 especially in the subgroups of workers and those on sick leave. Besides pain and physical limitations, the patients also mentioned the fear of movement and not being informed about the benefits of PA for the disease as a reason not being physically active, which has also been reported in other studies.44–46 This shows the importance of information and support from healthcare providers, which have been reported as facilitators of PA.47,48 One explanation of the fact that the retirees in this study most frequently met the recommendations for PA, is that retired patients may theoretically have more time for PA due to having more leisure time and that retirees generally perform more PA in comparison to workers. 49 Those on sick leave performed the same amount of PA as the workers, even though the former generally experienced more tender joints, which has also been reported in other studies. 44
MVPA was negatively associated with disease activity and tender joints, and it was also associated with physical function, indicating that improved physical function would benefit from exercising and vice versa as a previous study has suggested. 7 Furthermore, MVPA was associated with health-related quality of life, and in patients on sick leave, it was associated with disease activity, tender joints and pain. This indicates that perceived pain, reduced physical function, more tender joints and worse disease activity have an impact on PA, especially in patients on sick leave. Similar results, to those in this study, have also been reported by Cooney et al. 7 Furthermore, Pedersen and Saltin 50 also suggest that reduced levels of PA may be related to joint pain, limited mobility and fatigue.
The results showed that physical limitations such as pain and reduced PA are thought to be predictors of work disability for people with early RA as found in other studies. 51 The physical limitations themselves, apart from the pain, might even underlie the increased levels of sick leave, as shown by Geuskens et al. 52 Pain could indirectly contribute to the psychological and social influences from RA 53 since the social consequences of the disease comprise limitations in performing functions related to working as well as to family and social life. 54 These findings suggest that there is a multi-faceted picture behind the cause of reduced PA, where pain, tender joints and reduced physical function are factors that not only influence the patterns of PA but also the patients’ health status. Impaired physical function and pain are negatively related to self-reported health, 39 which indicates that there is an interrelationship between the independent variables of this study. This statement is further enhanced in other research, where it is suggested that PA, disease activity and physical function status appear to be interrelated.55,56 The occurrence of rheumatic diseases is related to not only increased risk of different types of physiological changes but also above all impairments. In total, 40% of people with RA in Europe 54 had to withdraw from work due to their illness since the loss of work ability is one of the consequences of the progressive disability in RA. The impact of disability on quality of life is thus dependent on several factors such as reduced income and increased disease-related costs. 54
This study shows that awareness as a motivator is a facilitator for performing PA, which is consistent with previous research. 45 The results indicate that it is important for healthcare providers to gain knowledge about what influences the PA of patients in order to understand the complexity in this context and then to motivate patients to be physically active in more adventurous ways. A motivational factor that influenced PA patterns was awareness-related caution, which served both as a barrier and a motivator for PA. The former has been reported in earlier research, where an expressed fear of pain during exercise contributes to reduced levels of PA. 8 Patients with RA also describe a fear of being injured, a fear of increased pain and a belief that exercise itself might aggravate the negative consequences of the disease. 22
Pain became a barrier to PA when it negatively influenced the patients’ motivation to engage in bodily movements. Since the fear of pain itself might cause a decrease in PA and also impact the quality of life negatively, 42 it is thus important to inform patients that an initial increase in pain might occur during the first exercising session 57 in order to prevent further decreases in PA. It is also crucial to introduce PA carefully and progressively 58 since this kind of PA-related pain might have an impact on future patterns of and beliefs about patient exercise and movement. 57 Motivation and awareness seemed to be related to some extent since the motivation had a promotional function on PA based on the patients being aware of the beneficial effects of PA on overall health. Given that preventing and controlling the disease as well as maintaining overall health requires engagement in PA, 14 the patients’ motivational experiences for encouraging engagement in PA can be emphasized. 14 The findings in this study can thus be useful for support in motivational issues and promoting PA engagement.
Other features of the results in this study are how external environmental factors, such as economy and climate, influenced the patients’ PA. The findings indicate that good weather influences the PA, as has been shown in previous research where the consequences of the illness were reduced in a sunnier and less humid climate. 59 Patients in this study found themselves having doubts about performing PA due to bad weather and the darkness during the winter season, leading to a decrease in PA and an increase in sedentary behaviour under these conditions. For some patients, it can be a struggle to perform PA due to economic limitations together with other motivational factors and pain as barriers to PA. It is thus important to heed the previous findings introducing the link between socioeconomic status, perceived pain and mental health in adults with RA. 20 Patients who experience difficulties such as economic limitations exercise less, 58 which can further broaden the wide range of factors influencing PA in patients with early RA. The healthcare services should apply a multi-faceted and more personalized treatment strategy for patients with RA when providing advice about PA to them. 60 Apart from managing the disease from the perspective of each unique patient, the importance of also having more tailored solutions for PA has been highlighted, as it is essential to maintain daily PA 60 but also PA based on specific recommendations in relation to the diagnosis. 7 Future studies of PA and health-related factors in people with RA should thus include this multi-perspective on what influences PA in patients with early RA. Pain as an impairment was expressed as being related to PA limitations and participation restrictions, as well as to motivational and external environmental factors. These findings highlight the importance of paying attention to the complexity of the clinical picture of RA, including physical limitations and adjustments due to pain, stiffness, tenderness as well as the awareness-related motivational factors. Considering that people with RA perform PA at low levels 24 regardless of the positive effects of the bodily movement, 9 it is important to gain greater knowledge about what can cause this. The results of this study can contribute an empirical rationale for healthcare services to improve PA participation in patients with early RA. In a long-term perspective, this might even contribute to improved overall mental and physical health in people with early RA.
Methodological considerations
Integrating both quantitative and qualitative methods can compensate for the potential weaknesses of the two in order to achieve an effective methodology 26 that includes triangulation as part of process. 27 The benefits of a mixed-methods approach are particularly evident when studying complex procedures in natural settings, which is the case in this study. The results suggest that the relationship between factors in the clinical picture and PA in patients with RA is complex and the strength of using the compensatory mechanism of a mixed-methods is further underlined by the fact that only physical limitations as a category would emerge if the results had only been based on quantitative data. Awareness as a motivational-related factors together with the external environmental factors would also have been missed. The overall picture of PA was shown in a more profound way since the mixed-methods approach allows a greater understanding of the field under study, where the quantitative method provided descriptive raw data and the qualitative data provided greater comprehension by capturing the patients’ experiences. 61
Graneheim et al. 30 have proposed five concepts of trustworthiness: credibility, dependability, transferability, confirmability and authenticity. In order for a qualitative study to have credibility, it is necessary that the focus and context of the study are plausible. Moreover, the credibility is strengthened through the mixed-methods approach together with the collected data being appropriate for seeking answers to the research questions. Furthermore, the study is enhanced by the participants having different experiences, age, gender and employment, thus generating a wider variation of the field being studied. It is important in the analysis that there is a sufficient number of meaning units and that the most suitable ones are chosen. 30 There were no difficulties in identifying the meaning units that corresponded to the aim of the study, greater precision was needed when identifying the correct categories and ensuring that risks for neglecting data were minimized. Another influence on the credibility and authenticity of a study is that the abstraction and interpretation may vary in depth, which can also threaten the overall trustworthiness. 29 According to Polit and Beck, 62 it is an advantage that the coding is performed by one and the same person as was the case in this study and the last author acted as a co-assessor. Credibility is also determined by how well the categories cover the participants’ expressions and that no useful data are neglected. Dependability was strengthened because all the informants were given the same open-ended questions and due to the co-authors’ familiarity with the subject area and the methodology employed. There was a progressive discussion among the authors and the categories were compared and revised until the final classification emerged. The issue of transferability focuses on the capability of the result being transferred to other circumstances or contexts in the eye of the reader. 29 It is possible that due to the mixed-methods design, the result of this study could be transferred to other contexts where patients with RA attempt to cope with the disease in terms of the symptoms and their influence on everyday activities. However, it may be of interest that retired participants answered the open-ended questions to a greater extent than those who worked. A limitation may be that there was no possibility to ask supplementary questions to the written answers. A further limitation is the low response rate and the small number of patients, which might affect the result in the quantitative phase, while there is saturation in the qualitative phase. There is also a limitation when using questionnaires for the assessment of PA and not accelerometers; however, several studies have used questionnaires for evaluating PA.56,63
Conclusion
The results showed a complex underlying motive where physical, psychological and environmental factors influenced the PA in patients with early RA.
In order to provide more effective health interventions, it is important to consider the complex nature of practicing PA, where a person-centred approach should be considered. Factors such as physical limitations, economic aspects and time for practicing PA, when working, should be included in a person-centred approach. There is a need for more knowledge about how to increase the level of PA in different subgroups of patients.
Supplemental Material
Supplementary_file_COREQ_SOM-19-0166R1 – Supplemental material for Factors influencing physical activity in patients with early rheumatoid arthritis: A mixed-methods study
Supplemental material, Supplementary_file_COREQ_SOM-19-0166R1 for Factors influencing physical activity in patients with early rheumatoid arthritis: A mixed-methods study by Maria Qvarfordt, Maria LE Andersson and Ingrid Larsson in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledge MD Annika Teleman and all the patients who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained by the regional ethical review board (LU 2012/604).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed and written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.